Methods: This post hoc analysis evaluated upadacitinib outcomes in patients with fistulizing disease in the following studies: phase 3 induction (U-EXCEL, U-EXCEED) and maintenance (U-ENDURE) trials. It was noted that there were 1021 patients in U-EXCEL and U-EXCEED; 143 (14.0%) had any fistulas at baseline (66 draining). Most (n = 128) had perianal fistulas (56 draining).
Key findings:
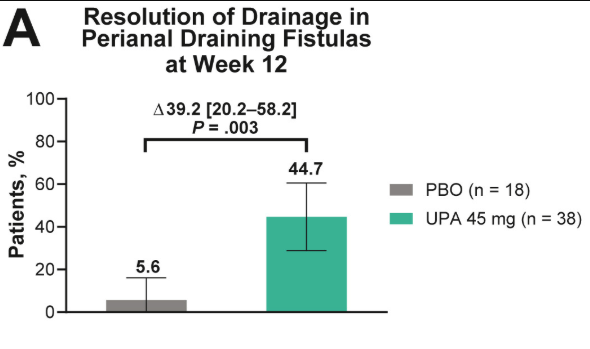
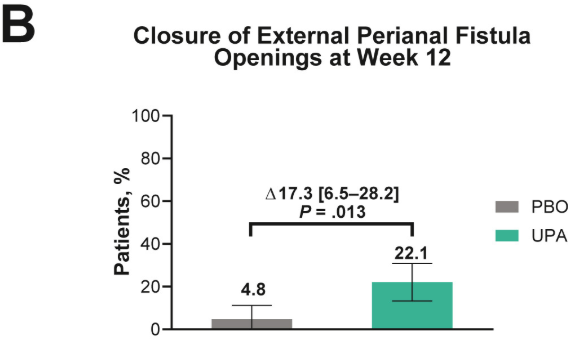
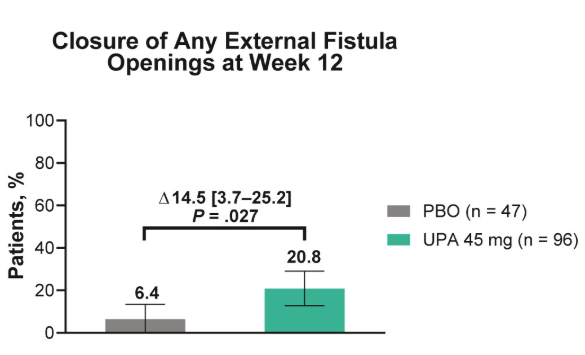
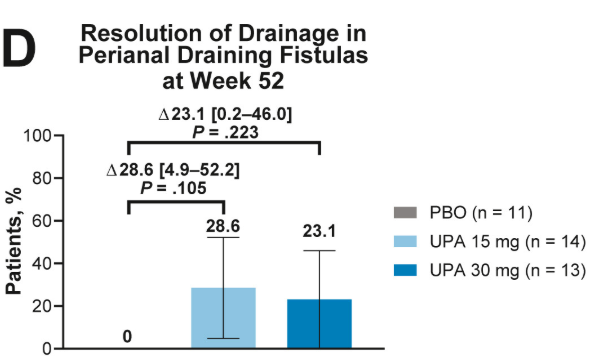
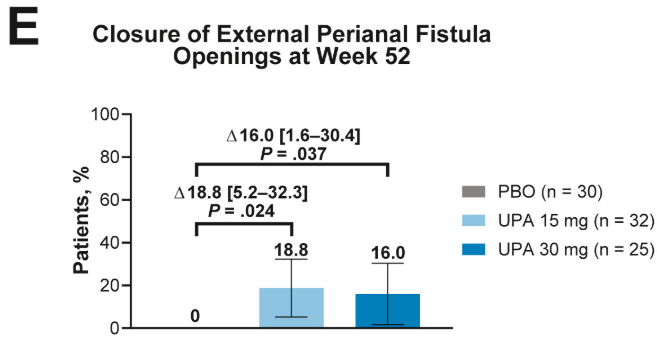
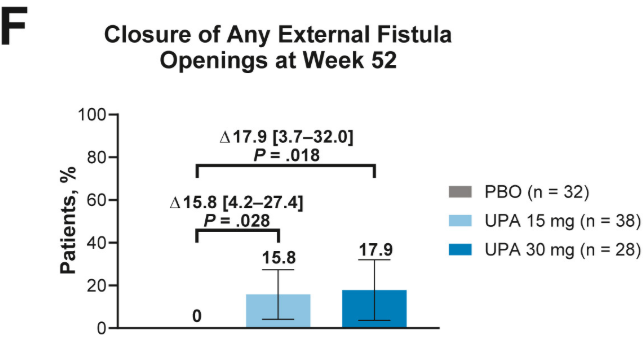
Fistulizing disease (primarily perianal) treated with upadacitinib achieved higher rates of resolution of drainage, closure of external openings, clinical remission, and endoscopic response vs placebo
These slides from Figure 1 show the resolution of drainage in perianal draining fistulas, closure of external perianal fistula openings, and closure of external openings for any fistula at week 12 of the induction trials and week 52 of the maintenance trial.
Discussion points:
Patients with draining fistulas often experience higher disease burden
Most patients in U-EXCEL and U-EXCEED had failed at least 2 prior biologic treatments (which often included anti-TNF therapy), reflecting a more refractory and difficult-to-treat population in CD
Despite the presence of perianal disease, patients with fistulizing CD treated with upadacitinib showed concurrent improvements in CD symptoms (CDAI, SF, and APS), luminal disease (endoscopic response and SES-CD), and markers of inflammation
My take: This study shows that upadacitinib is more effective than placebo; however, the majority of patients continued with ongoing perianal disease.
This case report of four patients provides a good review of metastatic Crohn’s disease (MCD). MCD indicates that there is noncontiguous dermatological spread of CD involving the genitalia and perineum.
Key points:
“Less than 100 cases of pediatric MCD have been reported in the literature to date. These lesions are characterized by swelling, plaques, nodules, fissures, ulcerations, or crusts. In children, MCD typically presents as genital swelling with or without erythema in approximately 85% of cases.”
“Prior studies have shown that MCD co-occurs with CD in 50.8% of children, while others may develop GI symptoms after MCD diagnosis (15.3%) or even lack signs of CD (11.9%).”
“Scrotal histopathology revealed granulomatous inflammation, and genetic testing identified pathogenic variants in NOD2, COL7A1, and Chek2, as well as additional variants of uncertain significance.”
The optimal treatment is not clear. “Prior case reports and case series have shown positive responses to TNF-α inhibitors, but relapses may be common. Similarly, only partial improvement was noted in our patients treated with infliximab and adalimumab.”
Discussion: “Many patients do not demonstrate GI symptoms and may experience significant delays in diagnosis.”
My take: This article provides a good review of metastatic Crohn’s disease which is a rare problem. I have had two patients with this disorder. This problem fits the adage of “the more you see, the more you know; and, the more you know, the more you see.”
This was a cross-sectional study of newly diagnosed pediatric patients (n=869) with IBD at 22 United States sites from 2019 to 2022. 57% were diagnosed with CD, 34% with UC, and 4% with IBD-U.
Key findings:
Overall, the mean time from symptom onset to diagnosis was 265.9 days
Factors associated with longer diagnosis time included CD vs UC (odds ratio [OR], 2.6), and longer travel time to clinic (>1 hour [OR, 1.7], >2 hours [OR, 1.8] each vs <30 minutes)
There was no association with race, ethnicity, birth country, gender, parent education, household income, insurance type, health literacy, and health system distrust
The finding that there is a longer diagnostic delay with CD than UC is consistent with prior studies. The longer travel time has not been widely recognized as a factor associated with delayed diagnosis, though it has been associated with other negative outcomes like higher mortality with chronic liver disease.
Regarding the lack of a negative impact from factors like race/ethnicity and income, my suspicion is that this is probably related to several factors:
Overall, the pediatric age group has a very high rate of being insured as most children without commercial insurance currently qualify for Medicaid. This helps improve access to needed/timely health care
B Kaj‐Carbaidwala et al. J Pediatr Gastroenterol Nutr. 2025; 80:450–454. Determining the time to cholangiocarcinoma in pediatric‐onset PSC‐IBD
Background: “Cholangiocarcinoma is a devastating disease, with up to 80% mortality and limited treatment options…A large retrospective cohort study reported that cholangiocarcinoma occurred in 1000 per 100,000 (1%) of children with PSC, with all occurring in children over 15 years of age and at a median of 6 years after the PSC diagnosis…Primary sclerosing cholangitis (PSC) is associated with a 400× increased risk of cholangiocarcinoma.”
Methods: Review of n = 175 studies resulted in a cohort of n = 21 patients with pediatric‐onset PSC‐IBD‐cholangiocarcinoma
Key findings:
The earliest diagnosis of cholangiocarcinoma was made at 14 years of age.
14% of of patients with pediatric‐onset PSC/IBD developed cholangiocarcinoma within the first 6 months of the second diagnosis
23% of patients with pediatric‐onset PSC/IBD developed cholangiocarcinoma within the first year of the second diagnosis
38% of patients with pediatric‐onset PSC/IBD developed cholangiocarcinoma within the first 2 years.
50% of patients with pediatric‐onset PSC/IBD developed cholangiocarcinoma within the first 7 years
50% of patients were between 14 and 25 years old when diagnosed with cholangiocarcinoma
Based on these data, the authors recommend screening for cholangiocarcinoma in this population of pediatric patients with IBD-PSC. Screening would include ultrasound or magnetic resonance cholangiopancreatography along with serum cancer antigen 19‐9 screening every 6–12 months. At the same time, the authors acknowledge limitations including a highly-selected patient population (selection bias) and relatively small number of patients. The absolute increase in risk for cholangiocarcinoma is not known. This study did not provide an estimate of the number of patients with IBD-PSC who develop cholangiocarcinoma; it only provides data on those with cholangiocarcinoma (thus no denominator to establish risk).
My take: Children, particularly adolescents, with IBD-PSC are at increased risk for both cholangiocarcinoma and colorectal cancer. The optimal surveillance strategy is still unclear. However, particularly in adolescents, I would favor yearly ultrasound and CA 19-9 for cholangiocarcinoma along with a low threshold for frequent colonoscopy (see ESPGHAN guidelines below).
In the news: AP 5/4/25: Cuts have eliminated more than a dozen US government health-tracking programs “U.S. Health Secretary Robert F. Kennedy Jr.’s motto is “ Make America Healthy Again,” but government cuts could make it harder to know if that’s happening…..Among those terminated at the Centers for Disease Control and Prevention were experts tracking abortions, pregnancies, job-related injuries, lead poisonings, sexual violence and youth smoking, the AP found.”
Anantara Resort, Mai Khao Phuket
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Methods: This was a “real-world practice” retrospective study (2017-2022) with 11,992 adult patients who were newly initiating a biologic therapy for UC/CD. 1,293 patients underwent a biologic switch, 64.2% of which were considered an overlapping switch (OS).
Key findings:
Adjusted incidence ratio IR) per 1,000 person years, for any infection, were comparable across switching groups. No significant differences in aHR of infections were found between OS and NOS [any infection aHR: 1.40, P=.17; serious infection aHR: 0.95, P=.93].
My take (borrowed from authors): “Overlapping switches were common and not associated with an increased risk of serious infection versus non-overlapping biologics.” Thus, shortened washout periods appear to pose minimal safety risks to patients while improving UC/CD therapy management.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition..
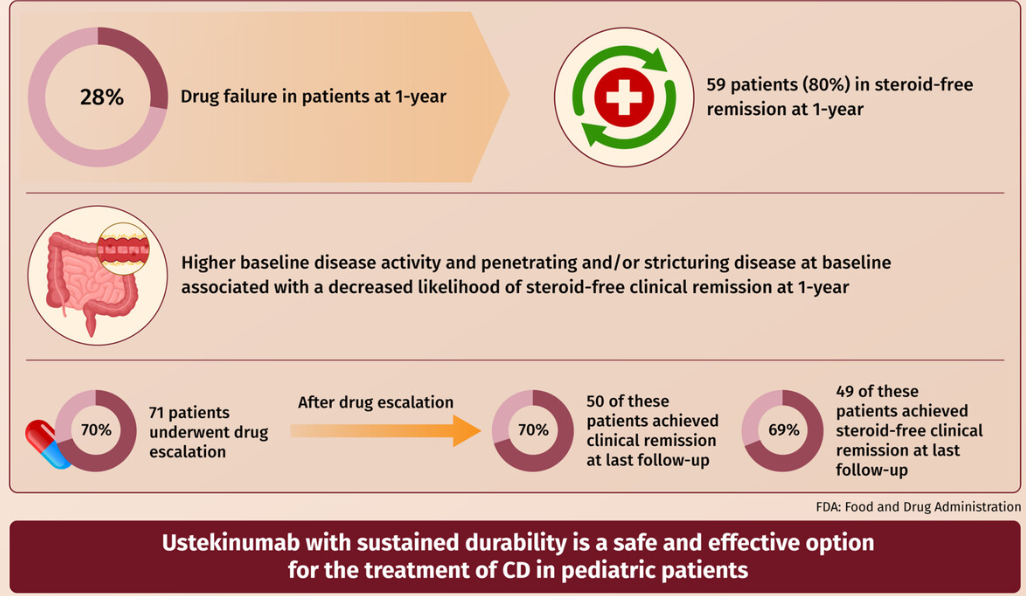
EB Mitchell et al. JPGN 2025;80:653–663. Ustekinumab is safe and effective in pediatric patients with Crohn’s disease
This was a retrospective longitudinal cohort study of 101 children with CD treated with ustekinumab from two large centers between 2015 and 2020. The median follow-up time on ustekinumab was 16.6 months.
Key findings:
Fifty-nine patients were in steroid-free clinical remission at 1 year.
Higher baseline disease activity (odds ratio [OR]: 0.91 (p = 0.01) and stricturing/penetrating disease phenotype (OR: 0.14 p = 0.02) were associated with decreased likelihood of steroid-free clinical remission at 1-year
Ustekinumab drug escalation occurred in 70% of patients, and after escalation, 50 (70%) achieved clinical remission, and 49 (69%) achieved steroid-free remission at the last follow-up
Adverse events were rare and did not require therapy discontinuation
My take: More pediatric data showing efficacy for ustekinumab is important. My sense, though, is that newer IL-23 specific agents are going to eclipse ustekinumab in pediatrics as they are doing in adults.
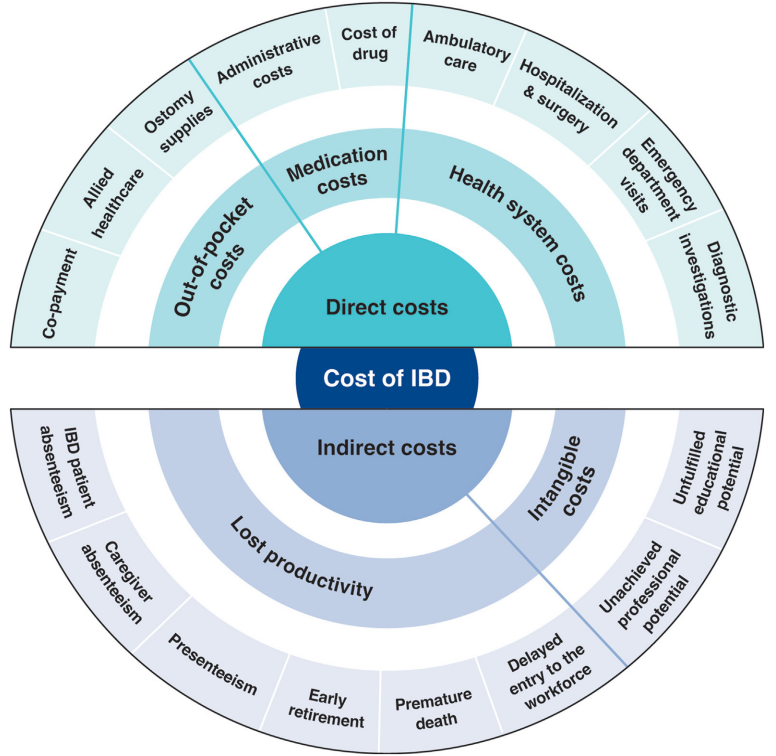
This article is a terrific review of care cost drivers in inflammatory bowel disease (IBD) but it does not actually have useful information on how to make the costs of care sustainable.
Key points:
The most recent data from the United States (U.S.) estimated that the prevalence of IBD was 0.7% of the population, representing 2.39 million individuals living with IBD…the annual cost of IBD in the U.S. approximates $50 billion
All studies demonstrated a shift over time from costs associated with hospitalizations to costs of medications
The costs of prescription drugs for IBD vary significantly worldwide… A particular outlier among high-income countries is the U.S., where manufacturers set prices freely. The lack of nationwide price regulation, coupled with the fragmentation of the U.S. health care system and prolonged market exclusivity periods, result in U.S. drug prices that exceed, on average, international prices by several-fold…Even when insurers are successful at negotiating discounts, patients seldom benefit, as costsharing paid at the point-of-sale is based on the full, non-discounted price
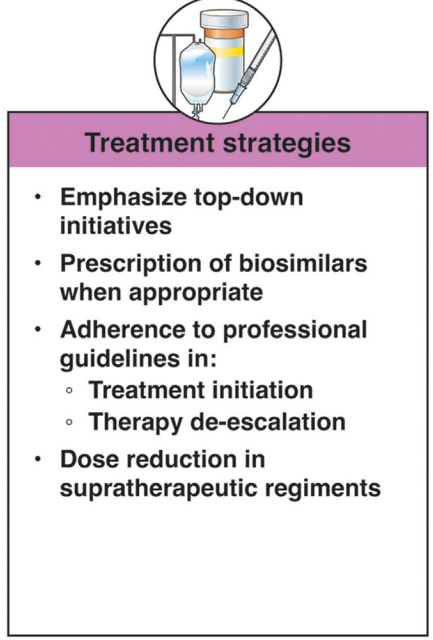
Using a “top-down” clinical paradigm, guidelines suggest starting biologic medications early to induce remission of moderate-to-severe IBD, thereby reducing risk of complications, surgeries, and hospitalizations and improving quality of life.55,58 A randomized controlled trial demonstrated a clear benefit in steroid-free and surgery-free remission among patients randomized to top-down vs step-up care (79% vs 15%; P < .0001) [PROFILE study]
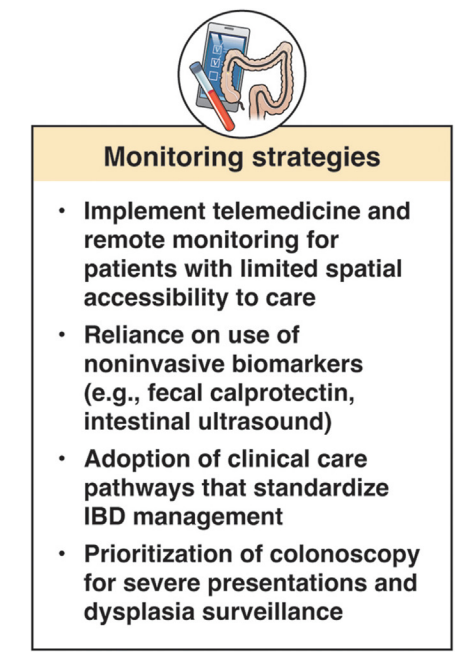
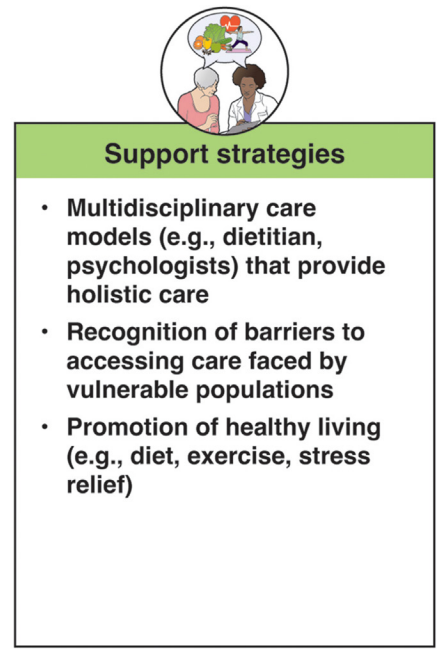
In terms of improving cost sustainability, here is what the authors propose “Strategies for cost reduction in the clinical treatment of IBD”:
My take: This article highlights the cost drivers in IBD but does not identify a path that appears to help address affordability.
This article is one of 11 articles in special issue discussing the future of IBD care.
This retrospective study reviewed adults with Crohn’s disease (CD) who underwent dose intensification of maintenance from 360 mg every 8 weeks to every 6 weeks (n=11) or every 4 weeks (n=11).
Key findings:
Median time to first intensified dose was 228 days
Harvey Bradshaw Index (HBI) improved from a mean of 7.1 to 4.3 after 8 to 16 weeks
There was also improvement (not statistically significant) in mean CRP (1.64–>0.42 mg/dL) and mean calprotectin (774 –>650 mcg/g)
At 8 to 16 weeks, 64% (14 of 22) had a clinical response, 45% (10 of 22) achieved steroid free clinical remission
My take: This small study suggests that the majority of patients with a loss of response to standard dosing can be recaptured with dose intensification.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
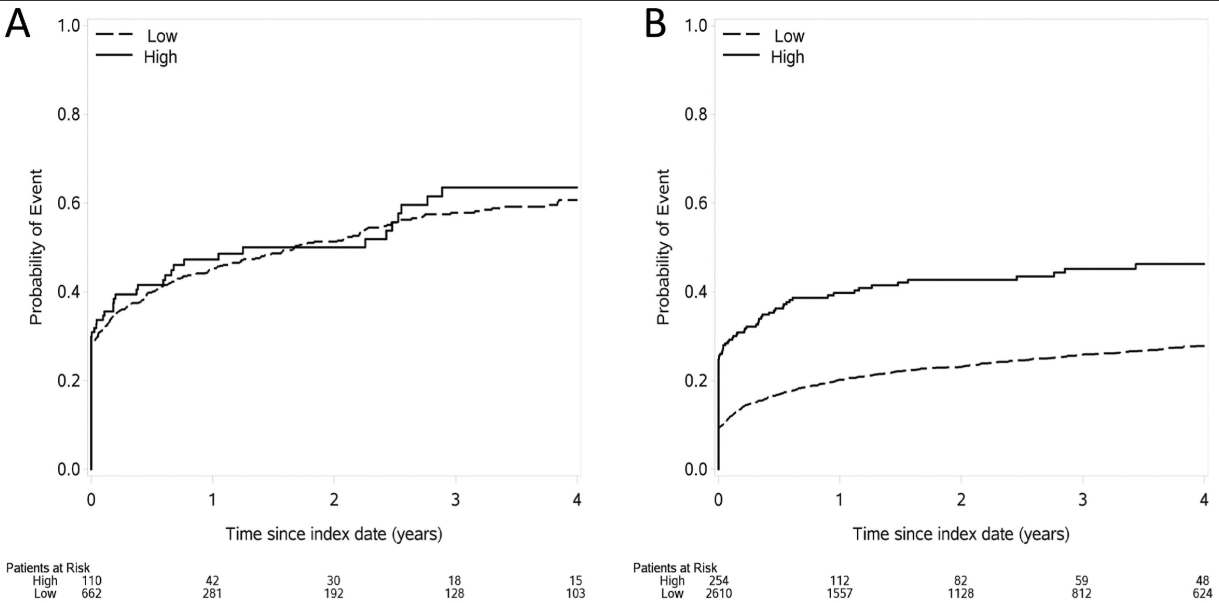
Methods: This was a retrospective cohort of newly diagnosed patients with IBD using data from Optum’s deidentified Clinformatics Data Mart Database (2000–2020). The study included 772 children treated by 493 providers and 2864 adults treated by 2076 providers.
Key findings:
In adults, care from an IBD-focused provider was associated with more use of biologics, combination therapy, and imaging and endoscopy, and less mesalamine use for Crohn’s disease (P < .05 for all comparisons)
In children, none of the associations between provider focus and process or outcome measures were significant. Although not statistically significant among children, the OR for mesalamine use was 0.64, suggesting a similar association as that seen among adults
Time to first dispensing of a biologic therapy in (A) children and (B) adults
My take: This study indicates significant treatment disparities between IBD-focused care providers and providers without an IBD focus in the care for adults, but not in the care of children. This could be related to improved collaboration among pediatric care providers, better training, and parental involvement.
In addition, this study focused on patients with newly-diagnosed disease. Treatment is more complicated in patients who have not responded to initial treatments; as such, IBD-focused providers may be more important in this population.