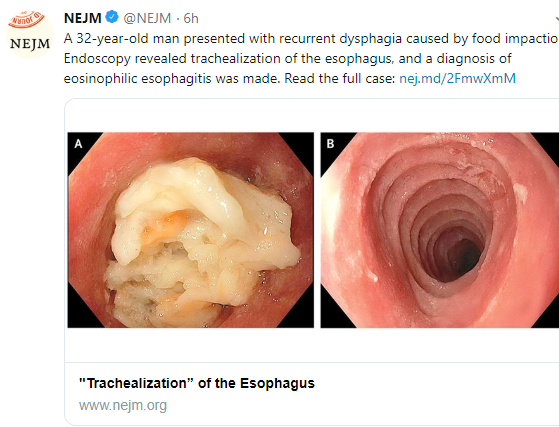
A recent retrospective study (N Nguyen et al. Clin Gastroenterol Hepatol 2019; 17: 2455-2462) describe the feasibility of unsedated transnasal endoscopy (TNE) for monitoring eosinophilic esophagitis (EoE) in children (n=190, subject ages 3-22 years).
TNE was facilitated by distraction with either video google or virtual reality (starting 2016). NPO time was 2 hours before the TNE.
Key points:
- Over 294 TNEs were completed from 300 attempts (98% success)
- Cost of TNE was halved: $4393 compared to $9444 for EGD (does not count pathology costs)
- Adverse events: 8 (2.7%) with vomiting, 9 (3.1%) spit up, 11 (3.7%) with epistaxis
- By 2017, TNE accounted for 31.8% of upper endoscopies in 2017
The authors recommend that TNE be offered starting at age 5 years in those without a known stricture.
My take: I am looking forward to less invasive/less costly ways of monitoring treatment response in EoE. I think TNE can lower costs –though I am a little surprised that the cost of TNE in their institution was still more than $4000. In our outpatient endoscopy center, costs for an upper endoscopy/biopsy with anesthesia are typically about one-third the cost of an EGD in their study and about three-fourths the cost of a study TNE.
Related study: A Krigel et al. Clin Gastroenterol Hepatol 2019; 17: 2489-96. This study showed increasing use of anesthesia assistance (AA) for colonoscopy in adults from 16.7% in 2006 to 58.1% in 2015. This data was derived from the Premier Perspective database with more than 4.6 million patients who had an outpatient colonoscopy. AA was associated with a median increase in cost of $182 for patients with commercial insurance.
Related blog post: Waiting for the String Test for EoE