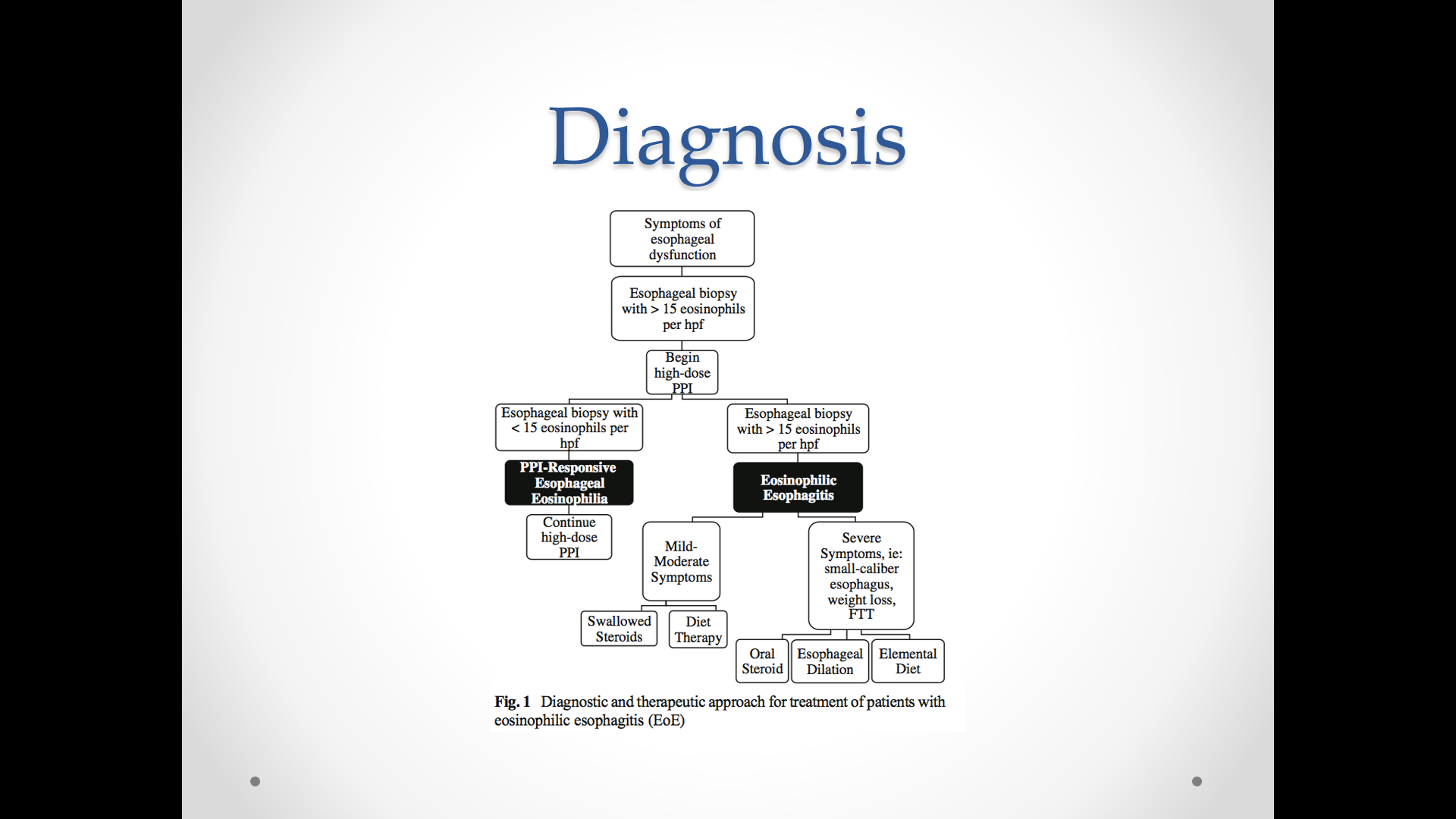
A prospective pediatric eosinophilic esophagitis (EoE) study (C Gutierrez-Junquera et al. JPGN 2018; 67: 210-6) examines the use of proton pump inhibitors (PPIs) for long-term management for this disorder.
After diagnosis of EoE, children received esomeproazole (1 mg/kg/dose BID). For those with a response (<15 eos/hpf), they were maintained on 1 mg/kg/day for one year.
Key findings:
- Of the initial cohort of 109, 72 (66%) had response to esomeprazole.
- 57 of these responders were subsequently followed in this study. At the lower daily esomeprazole dose, 70.1% (n=40) continued with <15 eos/hpf and 29.9% (n=17) had relapse.
- Maintaining response was more common among those who achieved an initial response (with BID esomeprazole) of <5 eos/hpf compared to those who had achieved an initial response of 6-14 eos/hpf. At 1 year, in those with who had a more complete response, 81% maintained eosinophil count <15/hpf compared with only 50% in those with a lesser initial response.
- Adverse events with prolonged treatment were uncommon and included self-resolving diarrhea in three, headache in one and urticaria in one; the latter two adverse effects responded to change to lansoprazole
My takes:
- PPI treatment is effective in probably 40-50% of individuals with EoE (though higher response in this study)
- Some individuals need higher doses of PPIs
- Due to the high response rate, this underscores the need to diagnose EoE prior to using PPIs or after they have been discontinued.
Related blog posts:
- Do we still need PPI-REE?
- Nexium versus Fluticasone for EoE
- Guidelines for Eosinophilic Esophagitis
- Higher Doses of Topical Steroids for Eosinophilic Esophagitis …
- Putting in Place a Big Piece of the Eosinophilic Esophagitis …
- Eosinophilic Esophagitis Slide Set | gutsandgrowth
- MicroRNA signature for eosinophilic esophagitis | gutsandgrowth