This year I had the opportunity to give a lecture to our group that reviewed much of the important advances that happened in 2024. Here are some of the slides (if you have any trouble reading the slides, you can search for the original blog post using author name).
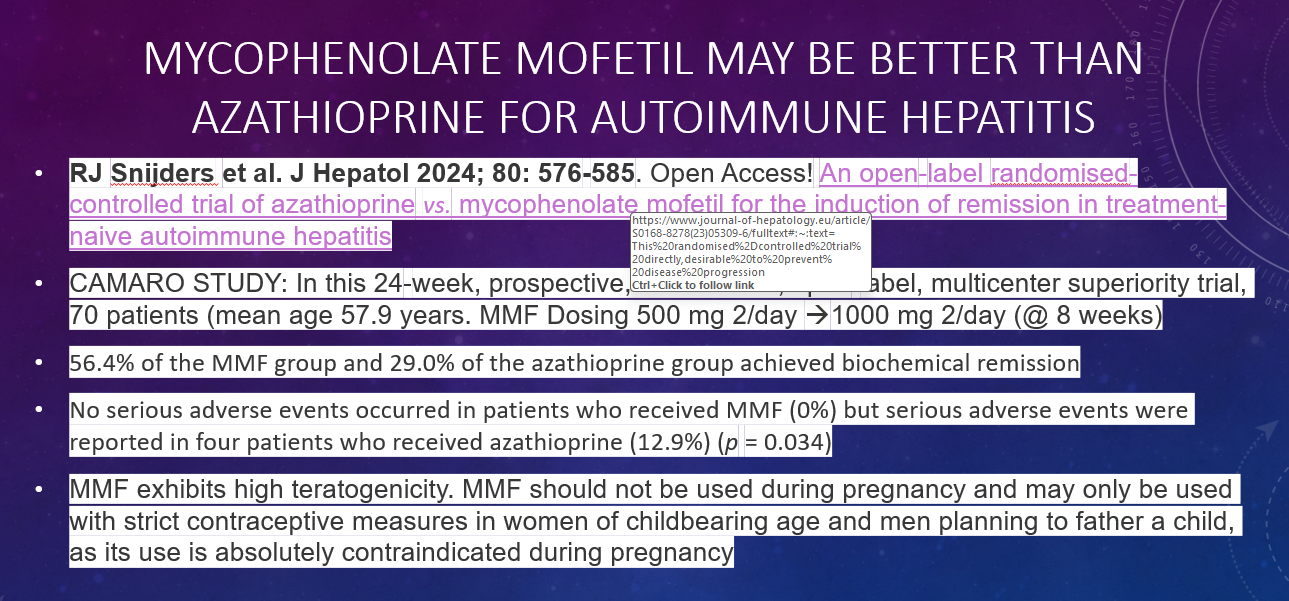
“Today, the U.S. Food and Drug Administration approved Dupixent (dupilumab) to treat eosinophilic esophagitis (EoE) in adults and pediatric patients 12 years and older weighing at least 40 kilograms (which is about 88 pounds). Today’s action marks the first FDA approval of a treatment for EoE…”
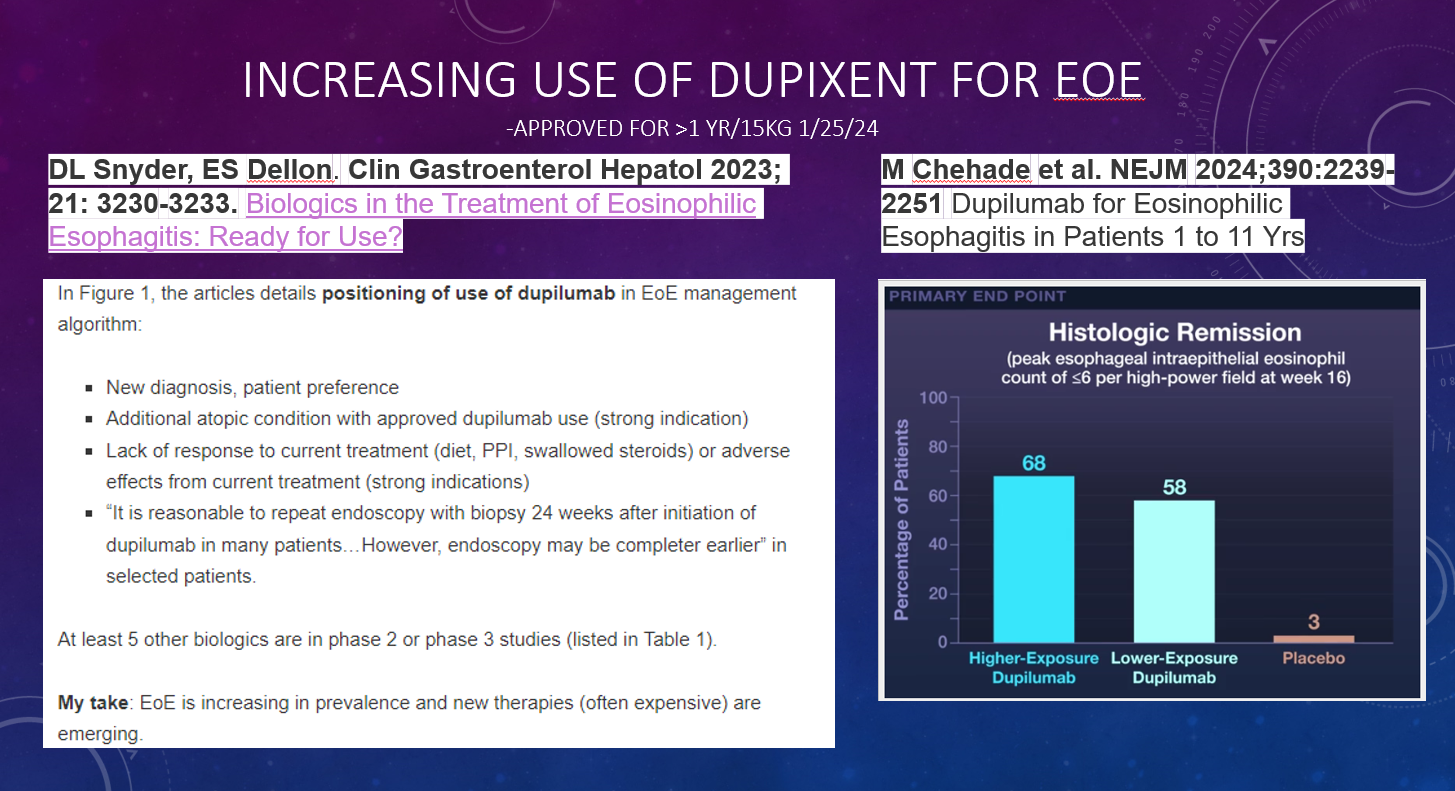
“The efficacy and safety of Dupixent in EoE was studied in a randomized, double-blind, parallel-group, multicenter, placebo-controlled trial, that included two 24-week treatment periods (Part A and Part B)…In Part A of the trial, 60% of the 42 patients who received Dupixent achieved the pre-determined level of reduced eosinophils in the esophagus compared to 5% of the 39 patients who received a placebo…. In Part B, 59% of the 80 patients who received Dupixent achieved the pre-determined level of reduced eosinophils in the esophagus compared to 6% of the 79 patients who received a placebo”
My take: We will need to revise our patient handout and decide how best to position this very expensive therapy. Without insurance, Dupixent (2 pens of 300 mg/2 mL) costs $3,649.97 on GoodRx. For those with insurance, Dupixent has a manufacturer’s coupon (Dupixent MyWay).
In this prospective study, the authors compared Eosinophil-Derived Neurotoxin (EDN) levels in pediatric patients with eosinophilic esophagitis (EoE) who responded PPIs (n=15) to those who did not respond to PPIs (n=21). The publication states that EDN levels of 10 mcg/mL or greater are diagnostic for EoE (sensitivity 97%, specificity 89%) but EDN levels have not previously been studied as a marker for PPI responsiveness.
Key finding: EDN concentration was significantly higher in the PPI-nonresponsive group than in the PPI-responsive group (219.1 ± 229 mcg/mL vs 75.7 ± 60 mcg/mL, respectively, P = 0.036).
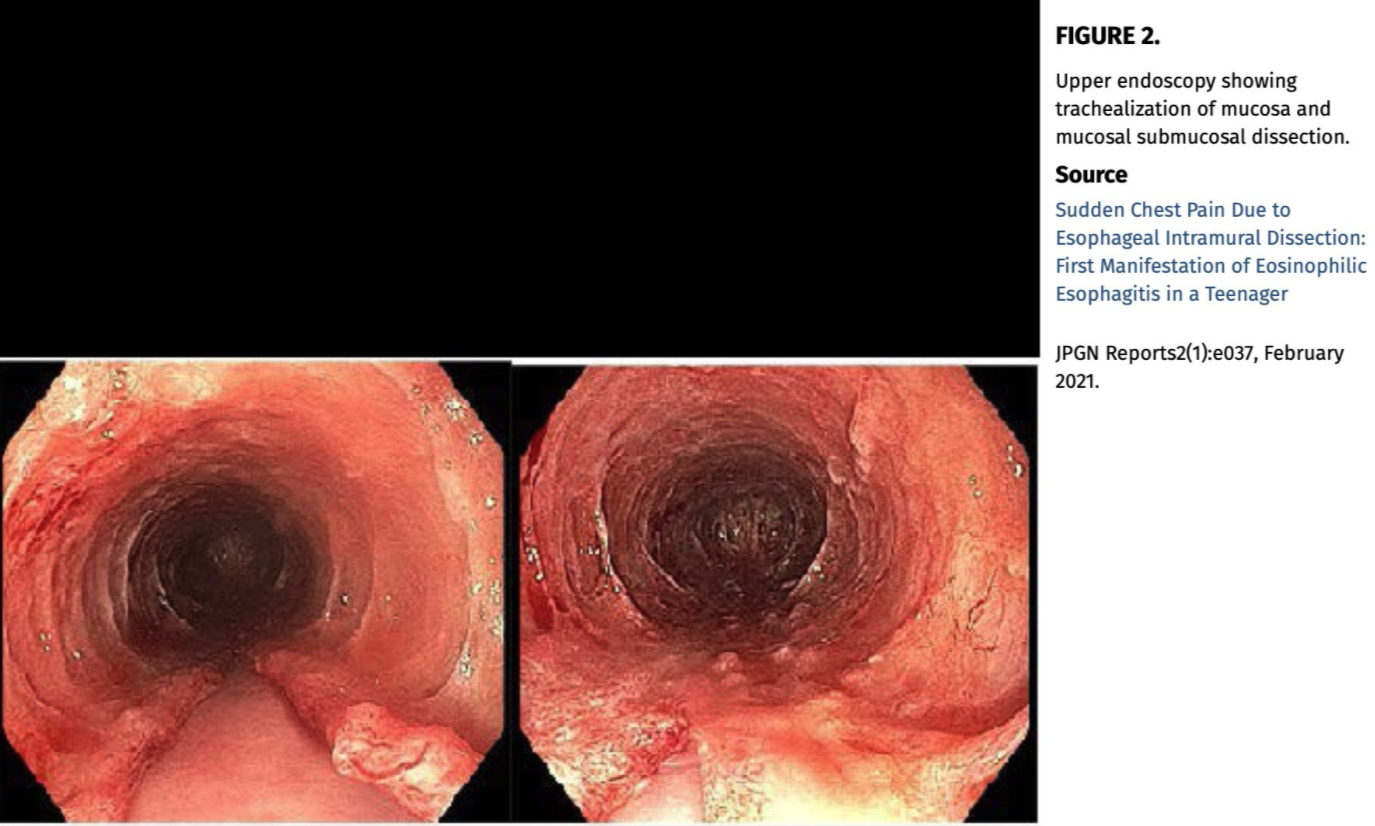
However, Figures 1 (see below) and 2 show that EDN levels while generally higher in those who did not respond to PPIs are not likely to help much at all in predicting who will respond to PPIs, mainly due to a lot of overlap in the levels. While very elevated levels (above ~300 mcg/mL) all occurred in PPI non-responders, this only accounted for 5 patients out of 36 in the entire cohort.
My take: This article’s title is quite misleading. EDN levels are generally higher in PPI-nonresponders but they do not predict response.
This case report examined the effect of benralizumab, a monoclonal antibody against the interleukin-5 receptor (IL5Rα) on eosinophils in 20 year old with asthma and EoE. Histology was notable for resolution of esophageal eosinophilia but demonstrated marked basal zone hyperplasia (BZH) in association with high numbers of CD3+ T cells and tryptase+ mast cells. Subsequently, she improved with the institution of dupilumab with resolution of BZH and mast cell inflammation with significant reduction in T cells.
My take: Even with resolution of eosinophilia, mast cells and T cells appear to be capable of coordinating mucosal inflammation and symptoms of EoE (at least in some patients). This study mirrors my limited experience, in which patients receiving benralizumab had a grossly abnormal-appearing esophagus but resolution of the eosinophils.
Background: “The incidence of EoE during OIT has been estimated at 2.7%.” (AJ Lucendo et al. Ann Allergy Asthma Immunol 2014; 113: 624-629)
Methods: Twenty adults with IgE-mediated peanut allergy were randomly assigned to groups given peanut OIT (n = 15) or placebo (n = 5) in this prospective study. Serial gastrointestinal biopsies were collected at baseline (n = 21, 0 weeks), following dose escalation (n = 10, 52 weeks), and during the maintenance phase (n = 11, 104 weeks)
Key findings:
At baseline: 3 of the 21 subjects (14%) had esophageal peak eosinophil counts ≥15 eos/hpf and all subjects had dilated intercellular spaces (DIS)
At 52 weeks: OIT induced or exacerbated esophageal eosinophilia (EoE) at 52 weeks with peak eosinophil counts ≥15 eos/hpf in 4 of 7 patients [57%] who did not have EoE at baseline. EoE did not develop in patients receiving placebo
At 104 weeks: In 4 of 6 participants (67%), OIT-induced EoE and gastrointestinal eosinophilia resolved by the end of the maintenance phase
One patient developed a clinical diagnosis of EoE.
The discussion notes overlap between EoE and IgE-mediated food allergy. The risk of EoE in patients with IgE-mediated food allergy is 118 times that of the general population (4.7% vs 0.04%) (J Allergy Clin Immunol Pract 2017; 5: 369-375). Also, the authors note that in this study all of the peanut allergic subjects had evidence of epithelial barrier dsyfunction.
My take: This small study shows, that for most adult patients, the development of EoE during OIT is often transitory.
In 2011, leaders of regional endoscopy units in Northern Denmark reached a consensus on a protocol to take eight biopsy samples in dysphagia patients (four biopsies from 4 cm and 14 cm above the esophagogastric junction-“4-14-4 rule”) regardless of the macroscopic appearance.
Key finding: Thenumber of patients with esophageal eosinophilia detected per year increased 50-foldafter the protocol was implemented in 2011 (median of 1 [interquartile range 0-3] vs. 52 [47-56]; P < 0.001), and the number of biopsy samples per patient doubled (median 4 [4-5] vs. 8 [6-9]; P < 0.04). In total, there were 309 with esophageal eosinophilia identified from 2007-2017.
My take: This study provides more data that more biopsies help identify more cases of eosinophilic esophagitis.
Related blog posts:
Best Approach for Identifying Eosinophilic Esophagitis Prior studies have shown higher yield when taking 5 or 6 biopsies rather than fewer biopsies; thus, the location of biopsies may not be as important as the number of specimens. Also, prior studies have shown that having another pathologist review the slides can increase the yield by ~20%; this indicates that careful review of specimens by itself is helpful. Perhaps, more specimen containers will increase the time that a pathologist reviews the biopsies.
Using the Inform Diagnostics database, which is a national electronic repository of histopathologic records from patients distributed throughout the entire United States, the authors performed a case-control study among 302,061 patients undergoing bidirectional endoscopy on the same day.
The database contained 3860 ulcerative colitis (UC) patients, 3330 Crohn’s disease (CD) patients, 1476 patients with indeterminate colitis with respect to UC or CD, and 5296 MC (microscopic colitis) patients.
Key findings:
EoE was less common in the overall IBD, CD, and MC case populations than the control population. Adjusted odds ratios (compared to control) :
EoE and IBD aOR 0.64
EoE and Crohn’s aOR 0.41
EoE and UC aOR 0.97
EoE and Indeterminate Colitis aOR 0.29
EoE and MC aOR 0.68
My take: (partly from authors) “Unexpectedly, the present analysis revealed statistically significant inverse relationships between EoE and CD or MC, but not UC.” Because endoscopy is often undertaken in those with a suspicion of IBD, EoE can be identified in the IBD population surreptiously; however, its frequency is likely less than in the general population.
This study analyzed data from 66 patients who completed the 16-week, double-blind, induction portion of a phase 2 study of RPC4046 (180 mg or 360 mg/wk) vs placebo and then completed a 52-week LTE, receiving open-label RPC4046 360 mg/wk. 20 of the 86 initial subjects (from the 16 week induction study) did not complete the full 52-week duration of the open label extension
Key findings:
Overall, 42 of 66 (64%) subjects had a peak eosinophil count <15 at 52 weeks
In the initially-treated group, 29/57 (51%) had peak eosinophil count <15 at 16 weeks
20/29 maintained a eosinophil count <15 at 52 weeks; 3 had an eosinophil count of 15 or greater at 52 weeks. Thus, 20/23 (87%) with data at 52 weeks maintained response.
In the initially-treated group, 28/57 (49%) had a peak eosinophil count of 15 or greater at 16 weeks
10/28 (36%) had a peak eosinophil count <15 at 52 weeks and 12 continued with an eosinophil count of 15 or greater at 52 weeks. Thus, 10/22 (45%) acquired a response after the induction period.
In the placebo induction group (n=29), none had a peak eosinophil count <15 at week 16
12/29 (43%) had a peak eosinophil count <15 at 52 weeks during open-label treatment; 9 continued with an eosinophil count of 15 or greater at 52 weeks. Thus, 12/21 (57%) developed a response without an induction treatment.
In addition to the improvements in eosinophil count, the authors identified clinical, endoscopic, and histologic improvement. “RPC4046 was well tolerated with little immunogenicity elicited in the LTE period.” Overall, the majority of treatment related adverse events were mild or moderate in severity and “no significant safety concerns.”
My take: This study shows that RPC4046 may emerge as a useful treatment for EoE.
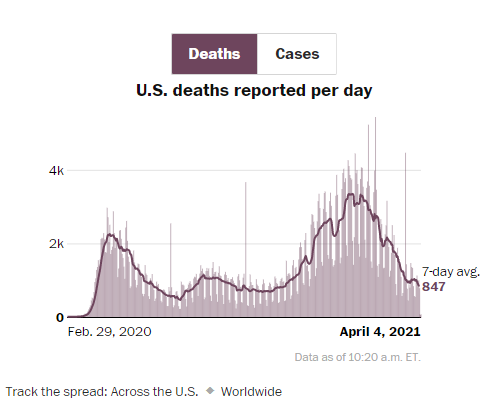
From Washington Post. U.S. Death rate from COVID-19 continues to decline, even though the number of reported daily cases has increased in last 3 weeks. With previous surges, deaths have been a lagging indicator. With the large number of vulnerable individuals vaccinated, it is unclear if the death rate will rise again or will continue to decline.
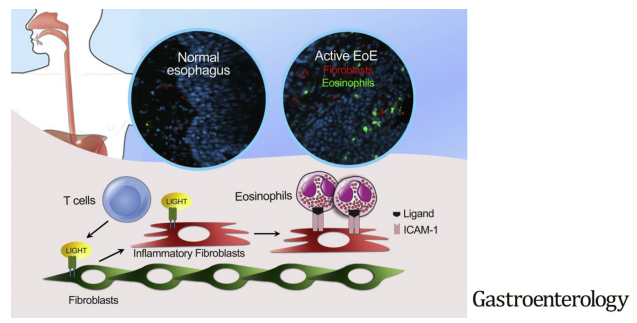
The authors investigated the effects of tumor necrosis factor superfamily member 14 (TNFSF14, also called LIGHT) on fibroblasts in EoE.
Key findings:
LIGHT was up-regulated in the esophageal tissues from patients with EoE, compared with control individuals
Stimulation of esophageal fibroblasts with LIGHT induced inflammatory gene transcription
My take: The authors show that patients with EoE had proinflammatory fibroblasts in the epithelium. Further, they show that eosinophil-fibroblast interaction was dependent on intact LIGHT signaling.