After inverse probability of treatment weighting (IPTW) (n = 819), the 5-, 10-, and 15-year cumulative HCC incidence was 3%, 4%, and 9% among treated patients (n = 394) versus 3%, 15%, and 19%, among untreated patients (n = 425), respectively (p = 0.02)
It took 5 years of treatment before there was a significant reduction in HCC risk
The protective effect was mainly in males; it was not observed in females and in patients who were HBeAg negative
The author studied patients with “Indeterminate” HBV; that is, patents that did not fit into the following categories:
The above definitions are AASLD definitions for the HBV categories. In their study, the authors’ definitions required immune tolerant to have ALT <1 x ULN, immune active to have ALT >/= ALT 2 x ULN. Inactive patients had no significant fibrosis or inflammation. The authors gauged fibrosis with either histology or a noninvasive measure (eg. FIB-4, or elastography)
My take: In this subgroup with indeterminate-phase chronic hepatitis B, antiviral treatment resulted in a 70% reduction in HCC risk. Previous AASLD guidelines indicated that treatment is mainly beneficial for immune active HBV; this study indicates that adults with indeterminate-phase HBV benefit as well. Also, as noted in prior blog posts (see below), the term “immune tolerant” is falling out of favor. In addition, updated expert recommendations on expanding treatment have been published: P Martin et al. Clin Gastroenterol Hepatol 2022; 20: 1766-1775 (post: What’s New in the Treatment of Hepatitis B (2022)
This is a very helpful review. Table 1 lists treatment indications by group. For example, AASLD recommendations:
Table 3 compares the effectiveness of current treatments
Table 4 describes the large number (~50) of antiviral agents in development and their mechanism of action
The authors recommend HCC surveillance in those with cirrhosis every 6 months with ultrasound with or without serum AFP
“Although current therapy is associated with improved clinical outcome, it is not curative because of a lack of effect on cccDNA and integrated HBV DNA. Stopping therapy in the absence of HBsAg loss usually leads to relapse to active disease in most patients and thus treatment must be administered long term.”
“Many challenges remain, the sheer breadth of therapeutic approaches in development holds great promise for curing and eliminating chronic HBV infection”
My take: While it is likely that newer medications will help many with chronic hepatitis B, the best hope for eliminating HBV continues to be with prevention and vaccination.
Key finding: In this study with more than 30 years of prospective followup (n=214): n a multivariate analysis, both an HBsAg titer >4.44 log10 IU/mL at 15 years of age and HBV genotype C were predictors of advanced fibrosis (odds ratios, 15.43 and 4.77; P = .01 and P = .02, respectively).
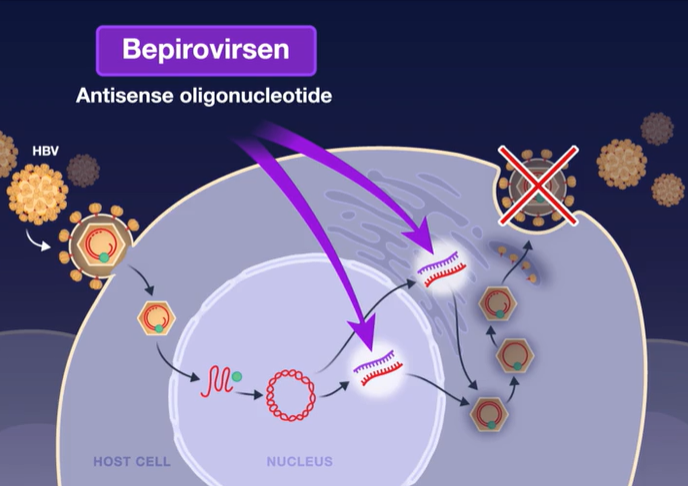
M-F Yuen et al. NEJM 2022; 387; 1957-1968. Efficacy and Safety of Bepirovirsen in Chronic Hepatitis B Infection
This study is nicely summarized in a “quick take” video and also reviewed in an accompanying editorial by J Hoofnagle (pages: 1996-1998).
In this phase 2b, randomized, investigator-unblinded trial involving 457 participants with chronic HBV infection (1/2 receiving nucleotide analogue (NA) therapy), the authors evaluated bepirovirsen is an antisense oligonucleotide that targets all hepatitis B virus (HBV) messenger RNAs and acts to decrease levels of viral proteins.
Background: HBV infection affects 4% of worldwide population and has a prevalence of 0.3% in the U.S. Worldwide, HBV causes more than 1/2 million deaths each year.
Key finding:
Mechanism of Action: Bepirovirsen is an antisense oligonucleotide that targets all hepatitis B virus (HBV) messenger RNAs and acts to decrease levels of viral proteins.
Current therapies (like entecavir and tenofovir) are able to suppress viral replication but have low rates of clearance of HBsAg and most often HBV relapses when medications are stopped. This is due to covalently closed circular DNA which can persist in hepatocytes despite these medications.
In Dr. Hoofnagle’s editorial, he notes that bepirovirsen is one of several RNA-based HBV therapies that are being pursued. There are also “the more malleable small interfering RNA molecules (“-sirans”) are currently in early-phase clinical trials.”
My take: While these studies point to new therapies for those afflicted with HBV infection, the best strategy for reducing HBV mortality and morbidity still relies of wide-scale use of the highly effective HBV vaccine.
This article provides some useful trends in Hepatitis B virus (HBV) epidemiology based on NHANES surveys (National Health and Nutrition Examination Survey). Persons who tested negative for anti-HBc, HBsAg, and anti-HBs were considered susceptible to HBV infection.
Key Findings:
The estimated prevalence of persons living with chronic hepatitis B in the USA has remained unchanged at 0.3% since 1999. During 2013-2018, this accounted for 880,000 US residents who were living with chronic HBV infection. It is noted that only a minority of the 11.7 million residents with a history of HBV develop chronic HBV
The non-US-born population accounted for 69% (610,000) of persons living with chronic HBV and 70% of this group were Asian. Non-US born population had a 9-fold risk of chronic HBV compared to US-born persons
Among adults aged ≥ 25 years who resided in US households, an estimated 155.8 million persons (or 73.4%) were susceptible to HBV infection. Susceptibility was lower in the 25-49 age group (64.8%) compared to the 50 years and older group (81.6%)
Despite vaccine recommendations, at risk groups including those using illicit drugs, hx/o MSM, and HCV exposure continue to have high susceptibility; fewer than 25% of adults “deemed to be at high risk for contracting HBV infection had vaccine-induced immunity
Overall, vaccine-induced immunity increased to 21.4% (2013-2018) compared to previously 17.9% (2007-2012) in those 25 years and older
Limitations: lack of detectable anti-HBs is likely to overestimate susceptibility in those who have previously been vaccinated, participation in NHANES by non-US born persons may have been unequal, and determining timing of HBV acquisition by non-US born persons was not feasible in this study
My take: Lots of adults have chronic HBV and lots more are susceptible. How to identify and encourage adults to avoid vaccine-preventable illnesses is NOT getting easier.
In this review, the authors propose expanding treatment indications for chronic hepatitis B virus (HBV).
The authors review current guidelines (Table 2 lists the major society recommendations). For example, the AASLD recommends HBV treatment for the following:
Antiviral treatment in all patients with cirrhosis and detectable viremia, independent of alanine aminotransferase (ALT) or HBV DNA levels
For patients without cirrhosis, all guidelines recommend treatment in patients with immune active disease; treatment is mainly with a NA (nucleos(t)ide analog) until 1 year after confirmed HBeAg seroconversion for patients who were HBeAg-positive and until HBsAg loss for patients who were HBeAg-negative at the start of treatment
AASLD cut-offs for distinguishing immune active disease: ALT ≥2× ULN or evidence of significant histologic disease and HBV DNA >20,000 IU/mL for HBeAg (+) and >2000 IU/mL for HBeAg (–)
Why Expand Treatment Indications?
The main reason for advocating treatment of patients in the immune tolerant phase is the mounting evidence that persistently high viremia and persistent presence of HBeAg are associated with increased risk of cirrhosis, HCC, and liver-related mortality…In one study of 438 HBeAg-positive patients, the 15-year cumulative risk of cirrhosis and HCC increased from 3.7% and 2.1% in patients who seroconverted before age 30 to 12.9% and 3.2% in those who seroconverted between ages 30 and 40 and 42.9% and 7.7% in those who did so after age 40
Why Not Treat All Patients with Chronic Hepatitis B?
“An important reason for deferring treatment of patients in the immune tolerant phase is that spontaneous HBeAg and HBsAg clearance with remission of liver disease can occur.” This happens in 80% or more over 10-20 years.
Who Else Should Receive Treatment (Beyond Guidelines)?
“Available data support expanding treatment to immune tolerant patients and patients in the grey zones who have evidence of active/advanced liver disease based on liver biopsy or non-invasive tests and those who remain in the immune tolerant phase after age 40. Evidence supporting treatment expansion to confirmed inactive carriers and other immune tolerant patients is lacking.” “Grey zones” indicate that “the course of chronic HBV infection is characterized by fluctuations in HBV DNA and ALT levels, and many patients will be in the grey zone at some point.”
My take: Given the safety/tolerability of newer HBV treatments, these recommendations make sense. If/when HBV treatments improve further (higher loss of HBsAg or HBV DNA), then even more widespread use of HBV treatments would be worthwhile.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
JE Squires et al. JPGN 2020; 70: 79-86. Using a prospective, longitudinal database, this study from ChiLDReN network with 93 children with biliary atresia and native liver found that NO increased prevalence of neurodevelopmental delays. Markers of advanced liver disease (high bilirubin/GGT for those ≤5 yrs, and portal hypertension for those >5 years) did negatively affect neurodevelopmental measures.
C Jaramillo et al. JPGN 2020; 70: 87-92. This pilot study with 21 patients found that degree of fibrosis, quantified by collagen hybridizing peptide, at time of Kasai, was associated with the risk of requiring a liver transplantation by age 4 years. Total bilirubin >2 mg/dL and Albumin ❤ g/dL at 3 months post-Kasai were also associated significantly with need for liver transplantation.
H-S Chen et al. Hepatology 2019; 70: 1903-12. In this study from Taiwan with 182 children (median age of 10.6 at enrollment) with hepatitis B and a normal ALT, a baseline anti-HBc titer of >500 IU/mL was associated with spontaneous HBeAg seroconversion with hazard ratio of 2.81. Over the median follow-up of 19.8 years, 85 subjects (46.7%) had HBeAg seroconversion. Thus, anit-HBc reflects anti-HBV immune response in the HBeAg-positive patients with normal ALT.
Table 4 (pg 1565): provides a refresher on interpretation of serology
Table 5 (pg 1567): Children and Adults Who Are HBsAg Positive:
Can participate in all activities, including contact sports
Should not be excluded from daycare or school participation and should not be isolated from other children
Can share food and utensils and kiss others
Figure 1 (pg 1571) Treatment algorithms.
For both HBsAg-positive/HBeAg-positive and HBsAg-positive/HBeAg-negative patients, treatment is recommended if ALT ≥2 x ULN.
For both groups, treatment is NOT recommended for those with ALT ≤ULN and low HBV DNA levels (<20,000 IU/mL for HBeAg-positive and <2,000 IU/mL for HBeAg-negative).
In those who do not fall into these categories, ongoing monitoring is recommended
Figure 1 from AASLD Guidance Link
Guidance Statements for HCC Screening in HBsAg‐Positive Persons
All HBsAg‐positive patients and high risk adults (see page 1574) with cirrhosis should be screened with US examination with or without AFP every 6 months.
There are insufficient data to identify high‐risk groups for HCC in children. However, it is reasonable to screen HBsAg‐positive children and adolescents with advanced fibrosis (F3) or cirrhosis and those with a first‐degree family member with HCC using US examination with or without AFP every 6 months.
Treatment:
In adults: The AASLD recommends peg‐IFN, entecavir, or tenofovir (TDF) as preferred initial therapy for adults with immune‐active CHB
In children: The AASLD suggests antiviral therapy in HBeAg‐positive children (ages 2 to <18 years) with both elevated ALT and measurable HBV‐DNA levels, with the goal of achieving sustained HBeAg seroconversion.
Perinatal transmission:
The AASLD suggests antiviral therapy to reduce the risk of perinatal transmission of HBV in HBsAg‐positive pregnant women with an HBV‐DNA level >200,000 IU/mL..The only antivirals studied in pregnant women are lamivudine, telbivudine, and TDF. Of these 3 options, TDF is preferred to minimize the risk of emergence of viral resistance during treatment. Interim studies show high efficacy of TDF in preventing mother‐to‐child transmission.
The infants of all HBsAg‐positive women should receive immunoprophylaxis (HBV vaccination with or without hepatitis B immunoglobulin, per World Heath Organization and Centers for Disease Control and Prevention recommendations)
Treatment & prevention of HBV reactivation in patients receiving immunosuppressive or cytotoxic drugs (section 6 pages 1577-9)
HBsAg and anti‐HBc (total or immunoglobulin G) testing should be performed in all persons before initiation of any immunosuppressive, cytotoxic, or immunomodulatory therapy.
HBsAg‐positive, anti‐HBc–positive patients should initiate anti‐HBV prophylaxis before immunosuppressive or cytotoxic therapy.
HBsAg‐negative, anti‐HBc–positive patients could be carefully monitored with ALT, HBV DNA, and HBsAg with the intent for on‐demand therapy, except for patients receiving anti‐CD20 antibody therapy (e.g., rituximab) or undergoing stem cell transplantation, for whom anti‐HBV prophylaxis is recommended.
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Mother-to-child transmission of hepatitis B virus (HBV) accounts for the majority of cases of chronic HBV infection. HBV infection affects more than 250 million people worldwide and in many cases results in cirrhosis or hepatocellular carcinoma. As such, there has been interest in preventing perinatal transmission.
The most recent study (C Jourdain et al. NEJM 2018; 378: 911-23) again showed that tenofovir administration to pregnant women with HBV can prevent transmission. This study enrolled 331 women. Key findings:
0% (0/147) infants in the tenofovir group developed HBV infection compared to 2% (3/147) in the control group. This did not reach statistical significance
The placebo group received HBV vaccination and hepatitis B immune globulin 1.2 hours and 1.3 hours after birth (median time). This rapid provision of treatment along with completion of four doses of HBV vaccine likely helped keep the placebo group HBV infection rate low
In the related editorial (G Dusheiko. pg 952-3), it is noted that “current levels of evidence supporting antiviral therapy with TDF [tenofovir] (or possbily lamivudine or telbivudine) to reduce levels of maternal HBV DNA during pregnancy have been accepted by the” AASLD.
Recently the AASLD Postgraduate Course discussed emerging treatments for nonalcoholic fatty liver disease/nonalchoholic steatohepatitis. From AASLD News: Emerging Treatments for NASH
Key point:
Quentin Anstee: “It is important to remember that our patients with fatty liver disease will most likely die of cardiovascular disease, not liver disease.”
Four principles in treating nonalcoholic fatty liver disease (NAFLD) to address both cardiovascular and liver risks.
Target obesity with lifestyle changes and, possibly, bariatric surgery.
Target metabolic syndrome to reduce cardiovascular disease risk using medications with additional liver-directed benefits.
Target liver disease to prevent progression of steatohepatitis to fibrosis and cirrhosis.
Minimize downstream complications such as hepatocellular carcinoma.
More than 60 phase 3 trials are underway –Primary Therapeutic Targets:
PPAR signaling (insulin signaling, glucose and lipid metabolism, energy homeostasis, inflammation)
As part of the Hepatitis B Research Network (HBRN), 343 children were enrolled in 7 U.S. and Canadian centers. A recent study (KB Schwarz et al. J Pediatr 2015; 167: 1287-94) provides data on HBV epidemiology and a related commentary by Brian McMahon (1186-7) provides some useful advice on what is needed to further reduce HBV infection.
88 children were not enrolled. More than half of these patients refused to participate, the other reasons included language barriers or inability to comply with follow-up.
Key findings:
78% of the subjects in this study were Asian
55% were adopted. This high adoption rate likely skews some of the data because (according to the associated editorial) “children with HBV in the US..most are likely to be children of parents who immigrated to the US from endemic countries and not adoptees.”
97% had international origins with either the child or a parent born abroad
HBV genotype B was most common (43%) followed by genotype C (32%), D (16%), A (5%), E (4%) or multiple (<1%).
In the editorial, Dr. McMahon notes that ascertaining the rate of a birth dose of HBV vaccine would be of interest. In many countries, vaccination is started at ≥2 months and this is unlikely to prevent HBV transmission. Two important public health issues for North America:
“First, all pregnant women, especially those foreign-born, need to be screened for HBsAg and if positive, their infants should receive HBV vaccine and hepatitis B immune globulin immediately after birth.”
“Second, all foreign-born children and adults who immigrate to the US or Canada should be tested for HBsAg.”
My take: This study provides an up-to-date snapshot of tertiary care for children with HBV in North America. There are many opportunities to curtail (or hopefully eliminate) the impact of HBV in our communities and around the world.