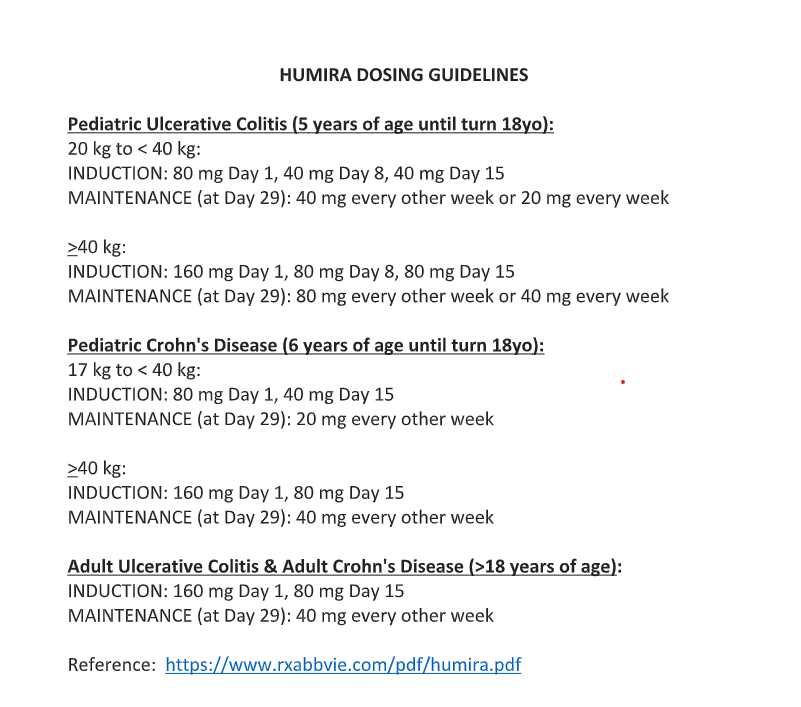
Correction made on blog post on 5/12/21 Humira Dosing Guidelines. For Crohn’s induction >/= 40kg, there is not an 80mg dose on day 8, just 160mg day 1 and 80mg day 15. Blog post: Ustekinumab for Refractory Pediatric Ulcerative Colitis and Updated Adalimumab Dosing
————————————————————————
NY Times: Can We Learn to Live With Germs Again? (4/23/21)
An excerpt:
Almost everything we know about the microbiome is uncertain, including how our activities and environments influence its makeup...
Despite the now consensus recognition that air transmission, …we continue to annihilate every microbe in our midst, even though most are harmless…
Excessive hygiene practices, inappropriate antibiotic use and lifestyle changes such as distancing may weaken those [microbial] communities going forward in ways that promote sickness and imperil our immune systems. By sterilizing our bodies and spaces, they argue, we may be doing more harm than good…
Dr. Graham Rook, an emeritus professor of medical microbiology at University College London, likens the immune system to a computer. He says that the microbes we encounter in daily life — on other people and in our spaces — are the data that the immune system relies on to program and regulate its operations.
Deprived of these exposures, especially at the start of life, the immune system is prone to malfunction. The result can be allergies, asthma, autoimmune disorders, obesity, Type 2 diabetes and other chronic medical conditions...
“Even before the pandemic, we know that half of antibiotic use was inappropriate.”…
For those who aren’t yet able to mix and mingle — and right now, that’s most of us — there are other ways to support microbial health. “If you want to do something proactive right now, I would put eating a healthy diet high on your list,” says Dr. Emeran Mayer… plant foods (legumes, greens, whole fruits, a variety of vegetables), as well as fermented foods, support the richness and diversity of the gut microbiome. So, too, does limiting one’s intake of processed and fast foods, especially those that contain added sugar…
Before the pandemic, only one of the top 10 causes of death in America — influenza — was attributable to an infectious disease that someone could “catch.” Nearly all the rest, such as heart disease and stroke, cancer, brain disease and diabetes, are associated with poor microbiome health or dysfunction.
Related blog posts:
- Origins of the Hygiene Hypothesis
- Why Asthma Study is Important: Hygiene Theory
- NYT: Educate Your Immune System | gutsandgrowth).
- Emigration -One Way to Acquire Inflammatory Bowel Disease | gutsandgrowth
- Why are we seeing so many more cases?