I am a pediatric gastroenterologist at GI Care for Kids (previously called CCDHC) in Atlanta, Georgia. The goal of my blog is to share some of my reading in my field more broadly. In addition, I wanted to provide my voice to a wide range of topics that often have inaccurate or incomplete information.
Before starting this blog in 2011, I would tear out articles from journals and/or keep notes in a palm pilot. This blog helps provide an updated source of information that is easy to access and search, along with links to useful multimedia sources.
I was born and raised in Chattanooga. After graduating from the University of Virginia, I attended Baylor College of Medicine. I completed residency and fellowship training at the University of Cincinnati at the Children’s Hospital Medical Center. I received funding from the National Institutes of Health for molecular biology research of the gastrointestinal tract.
During my fellowship, I had the opportunity to work with some of the most amazing pediatric gastroenterologists and mentors. Some of these individuals included Mitchell Cohen, William Balistreri, James Heubi, Jorge Bezerra, Colin Rudolph, John Bucuvalas, and Michael Farrell. I am grateful for their teaching and their friendship. During my training with their help, I received a nationwide award for the best research by a GI fellow.
I have authored numerous publications/presentations including original research, case reports, review articles, and textbook chapters on various pediatric gastrointestinal problems. In addition, I have been recognized by Atlanta Magazine as a "Top Doctor" in my field multiple times.
Currently, I am the vice chair of the section of nutrition for the Georgia Chapter of the American Academy of Pediatrics. In addition, I am an adjunct Associate Clinical Professor of Pediatrics at Emory University School of Medicine. Other society memberships have included the North American Society for Pediatric Gastroenterology Hepatology and Nutrition (NASPGHAN), American Academy of Pediatrics, the Food Allergy Network, the American Gastroenterology Association, the American Association for the Study of Liver Diseases, and the Crohn’s and Colitis Foundation.
As part of a national pediatric GI organization called NASPGHAN (and its affiliated website GIKids), I have helped develop educational materials on a wide-range of gastrointestinal and liver diseases which are used across the country. Also, I have been an invited speaker for national campaigns to improve the evaluation and treatment of gastroesophageal reflux disease, celiac disease, eosinophilic esophagitis, hepatitis C, and inflammatory bowel disease (IBD). Some information on these topics has been posted at my work website, www.gicareforkids.com, which has links to multiple other useful resources.
I am fortunate to work at GI Care For Kids. Our group has 17 terrific physicians with a wide range of subspecialization, including liver diseases, feeding disorders, eosinophilic diseases, inflammatory bowel disease, cystic fibrosis, DiGeorge/22q, celiac disease, and motility disorders. Many of our physicians are recognized nationally for their achievements. Our group of physicians have worked closely together for many years. None of the physicians in our group have ever left to join other groups. I have also worked with the same nurse (Bernadette) since I moved to Atlanta in 1997.
For many families, more practical matters about our office include the following:
– 14 office/satellite locations
– physicians who speak Spanish
– cutting edge research
– on-site nutritionists
– on-site psychology support for abdominal pain and feeding disorders
– participation in ImproveCareNow to better the outcomes for children with inflammatory bowel disease
– office endoscopy suite (lower costs and easier scheduling)
– office infusion center (lower costs and easier for families)
– easy access to nursing advice (each physician has at least one nurse)
I am married and have two sons (both adults). I like to read, walk/hike, bike, swim, and play tennis with my free time.
I do not have any financial relationships with pharmaceutical companies or other financial relationships to disclose. I have helped enroll patients in industry-sponsored research studies.
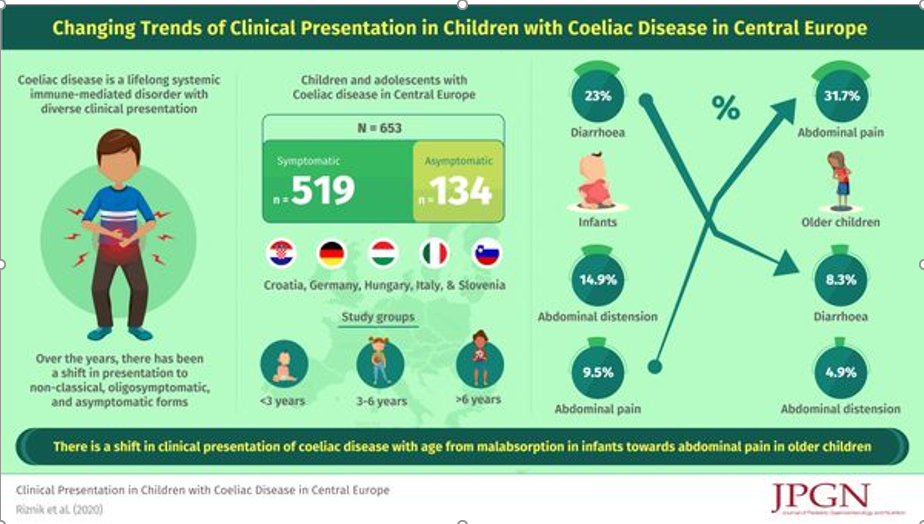
Two recent JPGN articles from the same researchers highlight changes in presentation and deficits of knowledge with celiac disease (CD). Interestingly, the authors chose to spell celiac disease differently in the two articles.
This retrospective study included data from 653 children and adolescents (median age 7 years 2 months; 63.9% girls) from Croatia, Germany, Hungary, Italy, and Slovenia were available for the analysis. Key findings:
One fifth (N = 134) of all children were asymptomatic.
In symptomatic children, the most common leading symptom was abdominal pain (33.3%), followed by growth retardation (13.7%) and diarrhoea (13.3%). Many children (47.6%; N = 247) were polysymptomatic.
Symptoms and signs of malabsorption (eg. diarrhea and distention) were significantly more common in younger (P < 0.001)
Methods: This was a a 72-week, double-blind phase 2 trial involving patients with biopsy-confirmed NASH and liver fibrosis of stage F1, F2, or F3. Patients were randomly assigned, in a 3:3:3:1:1:1 ratio, to receive once-daily subcutaneous semaglutide at a dose of 0.1, 0.2, or 0.4 mg or corresponding placebo.
Key findings:
The percentage of patients in whom NASH resolution was achieved with no worsening of fibrosis was 40% in the 0.1-mg group, 36% in the 0.2-mg group, 59% in the 0.4-mg group, and 17% in the placebo group (P<0.001 for semaglutide 0.4 mg vs. placebo).
An improvement in fibrosis stage occurred in 43% of the patients in the 0.4-mg group and in 33% of the patients in the placebo group (P=0.48).
The mean percent weight loss was 13% in the 0.4-mg group and 1% in the placebo group.
Safety: Malignant neoplasms were reported in 3 patients who received semaglutide (1%) and in no patients who received placebo. Overall, neoplasms (benign, malignant, or unspecified) were reported in 15% of the patients in the semaglutide groups and in 8% in the placebo group
Clearly this study indicates that there may be safety concerns with semaglutide. In addition to the malignant neoplasms, there were 8 individuals with colonic polyps in the treatment groups and 7 with renal cysts in the treatment group. However, the authors note that in a recent meta-analysis with 55,921 patients, GLP-1 agonists were not associated with an increased risk of malignant neoplasms (Diabetes Obes Metab 2020; 22: 699-704).
Related article: JPH Wilding et al. NEJM 2021; 384: 989-1002. Once-Weekly Semaglutide in Adults with Overweight or ObesityKey finding: The mean change in body weight from baseline to week 68 was −14.9% in the semaglutide group as compared with −2.4% with placebo. This study indicates potential for GLP-1 Agonist class for pharmacologic treatment of obesity.
My take: The improvement in NASH with semaglutide is encouraging and perhaps improvement in fibrosis will occur with more time. Yet, more time is also needed to determine if this agent is truly safe in this population. In patients receiving other GLP analogues, vigilance for adverse events is needed as well.
This study derived data from a longitudinal cohort; the sample for this study followed women with and without endometriosis who completed extensive surveys (n=323) and excluded women with celiac disease or inflammatory bowel disease. Cases of IBS were based on patient reports of Rome IV criteria, though 81% were confirmed via medical record review.
Key findings:
“More adolescents with endometriosis (54 of 224; 24%) had comorbid IBS compared with adolescents without endometriosis (7 of 99; 7.1%). The odds of IBS was 5.26-fold higher among participants with endometriosis than without (95% CI, 2.13–13.0).”
“For participants with endometriosis, each 1-point increase in acyclic pain severity increased the odds of IBS by 31% (adjusted odds ratio, 1.31; 95% CI, 1.18–1.47).”
The association of endometriosis with IBS was based on Rome IV criteria, as such, the authors assert that this is “not merely a diagnostic bias” However, some of the increase may be related to referral patterns.
Useful points:
“In the adult literature, pain in the pelvis, menstrual-related symptoms, symptoms related to sexual intercourse, ovarian cysts, and subfertility seem to distinguish women with endometriosis from other GI conditions.”
“Chronic pain syndromes were more prevalent in girls with endometriosis and IBS. Rates of migraine headaches, sleep disturbance, and urinary symptoms were higher…[and] had higher prevalence rates of mood disturbance.”
Why is there overlap between these disorders?
The authors speculate that “the inflammatory process likely plays a role…and central pain sensitization may play a crucial role in the two diseases”
My take: Adolescents with endometriosis have a higher likelihood of IBS. Acyclic pain is a strong predictor of IBS.
1st Advance: In 1796, Edward Jenner “found that an animal virus (cowpox) could protect against disease caused by a human virus (smallpox)… Jenner’s work ultimately led to the eradication of a disease that is estimated to have killed more than 300 million people in the 20th century”
2nd Advance: In 1885, Louis Pasteur developed an inactivated virus vaccine for rabies. This has led to the development of many other inactivated vaccines, including the influenza vaccine.
3rd Advance: In 1937, Max Theiler attenuated yellow fever virus by means of serial passage in mouse and chicken embryos. This has led to the development of numerous attenuated vaccines to prevent polio (Sabin, 1960s), measles (1963), mumps (1967), rubella (1969), varicella (1995), and rotavirus (2008).
4th Advance: In 1980, Stanford biochemists Richard Mulligan and Paul Berg developed recombinant DNA technology which led to vaccines containing purified surface proteins. This led to the hepatitis B virus (1986), human papillomavirus (2006), and influenza virus (2013) vaccines.
Some of the notable improvements related to vaccines:
In U.S., the incidence of polio dropped from 29,000 cases in 1955 to elimination
In U.S., during the “2019–2020 influenza season, the influenza vaccine prevented an estimated 7.52 million infections, 3.69 million medical visits, 105,000 hospitalizations, and 6300 deaths”
In U.S., the measles vaccine has nearly eliminated a virus that previously caused 2 million to 3 million infections, 50,000 hospitalizations, and 500 deaths every year
In U.S., “since the hepatitis B virus vaccine started being routinely recommended for newborns in the early 1990s, rates of hepatitis B virus infection among children younger than 10 years have fallen from about 18,000 per year to nearly zero”
Globally, “between 2000 and 2018, roughly 23 million measles deaths were prevented by vaccination…Live attenuated rotavirus vaccines are countering a virus that once killed more than 500,000 infants and young children each year”
5th Advance: In 2020 “with the recent authorization of mRNA vaccines, we have entered the fifth era of vaccinology. This class of vaccines doesn’t contain viral proteins; rather, these vaccines use mRNA, DNA, or viral vectors that provide instructions to cells on how to make such proteins. The SARS-CoV-2 pandemic will be an important test of whether these new platforms can fulfill their promise of creating safe, effective, and scalable vaccines more quickly than traditional methods.”
As noted in yesterday’s post, in addition to private equity, hospitals have been consolidating medical practices. One incentive has been that hospitals can often charge a “facility fee.”
An excerpt: The increasingly controversial charge — basically a room rental fee — comes without warning, as hospitals are not required to inform patients of it ahead of time…
Hospitals say they charge the fee to cover their overhead for providing 24/7 care, when needed. Stamatis also noted the cost of additional regulatory requirements and services “that help drive quality improvement and assurance, but do increase costs.“
But facility fees are one reason hospital prices are rising faster than physician prices, according to a 2019 research article in Health Affairs….The Centers for Medicare & Medicaid Services has attempted to curtail facility fees by introducing a site-neutral payment policy. The American Hospital Association sued over the move and plans to take the case to the Supreme Court.
My take: When hospitals own physician practices, there are often hidden costs. NPR recommends: “Ask outright if there will be a facility fee — and how much — even if there has not been one before. If it’s an elective procedure, you can search for a cheaper provider.”
A recent commentary (JM Zhu et al. NEJM 2021; 384: 11: 981-983. Private Equity and Physician Medical Practices — Navigating a Changing Ecosystem) describes the restructuring of medical practices with a major decline in independent practices due to the growth of hospital-affiliated employees and private-equity investment in medical specialties.
Key points:
Between July 2016-January 2018, “hospitals and health systems acquired more than 8000 practices…Roughly 14,000 physicians left private practice”
Private-equity investment in medical practices has emerged as an alternative source of investment “that allows physicians to continue to hold equity and benefit financially from future transactions.”
Potential consequences of private-equity investment in medical practice:
Reduction in competition
Leverage market power with insurers & possible higher costs
Possible additional pressures on physicians to improve profits and reduction of physician autonomy
Possible improvements in value with operational improvements including sharing industry knowledge with smaller practices, adopting technology infrastructure, and helping practices assume risk with value-based payments
Possible prioritization of patients with better payer mix and lower complexity
My take: Mergers and acquisitions whether through hospitals or private equity make me worried that physicians will be squeezed between delivering profits and providing the best service for our patients.
This was a retrospective cohort study which included 169 patients who never smoked actively, 91 patients (54%) were exposed to passive smoking.
Key finding:
Exposed patients were more likely to undergo intestinal surgery than nonexposed patients (67% vs 30%; P < 0.001). Multivariate Cox regression analysis revealed that passive smoking was an independent risk factor for intestinal surgeries (hazard ratio, 1.7; 95% CI, 1.04–2.9; P = 0.034)
Smoking has long been identified as one of the strongest environmental risk factors for both the development of Crohn disease (CD) and the worsening of the disease course.
Studies in smokers with CD have reported that the risk of flares and complications matches that of nonsmokers with CD after 1 year of abstinence.
It would be reasonable to expect that a similar risk reduction exists for patients who can become passive-smoke-free. In addition, their likelihood of remaining smoke-free themselves is increased if they live in a smoke-free household.
My take (from editorial): “Clinicians should consider widening the scope of smoking cessation counseling to include not just patients but also their cohabitants.”
Using the Inform Diagnostics database, which is a national electronic repository of histopathologic records from patients distributed throughout the entire United States, the authors performed a case-control study among 302,061 patients undergoing bidirectional endoscopy on the same day.
The database contained 3860 ulcerative colitis (UC) patients, 3330 Crohn’s disease (CD) patients, 1476 patients with indeterminate colitis with respect to UC or CD, and 5296 MC (microscopic colitis) patients.
Key findings:
EoE was less common in the overall IBD, CD, and MC case populations than the control population. Adjusted odds ratios (compared to control) :
EoE and IBD aOR 0.64
EoE and Crohn’s aOR 0.41
EoE and UC aOR 0.97
EoE and Indeterminate Colitis aOR 0.29
EoE and MC aOR 0.68
My take: (partly from authors) “Unexpectedly, the present analysis revealed statistically significant inverse relationships between EoE and CD or MC, but not UC.” Because endoscopy is often undertaken in those with a suspicion of IBD, EoE can be identified in the IBD population surreptiously; however, its frequency is likely less than in the general population.
This was a population-based prospective study from Canterbury, New Zealand
Key findings:
Overall incidence rates were 1.93 per 100,000 for AIH (95% CI, 1.58–2.34), 0.51 per 100,000 for PBC (95% CI, 0.33–0.73), and 0.92 per 100,000 for PSC (95% CI, 0.68–1.21).
The incidence rateof AIH was significantly higher during the period of 2014–2016 (2.39 per 100,000; 95% CI, 1.76–3.23) than during the period of 2008–2010 (1.37 per 100,000; 95% CI, 0.91– 2.06) (P < .05). Incidences of PBC and PSC did not change significantly.
In 2016, prevalence values were 27.4 per 100,000 for AIH (95% CI, 23.58–32.0), 9.33 per 100,000 for PBC (95% CI, 7.13–12.05), and 13.17 per 100,000 for PSC (95% CI, 10.56–16.42).
My take: This study indicates that autoimmune hepatitis has been increasing in incidence.
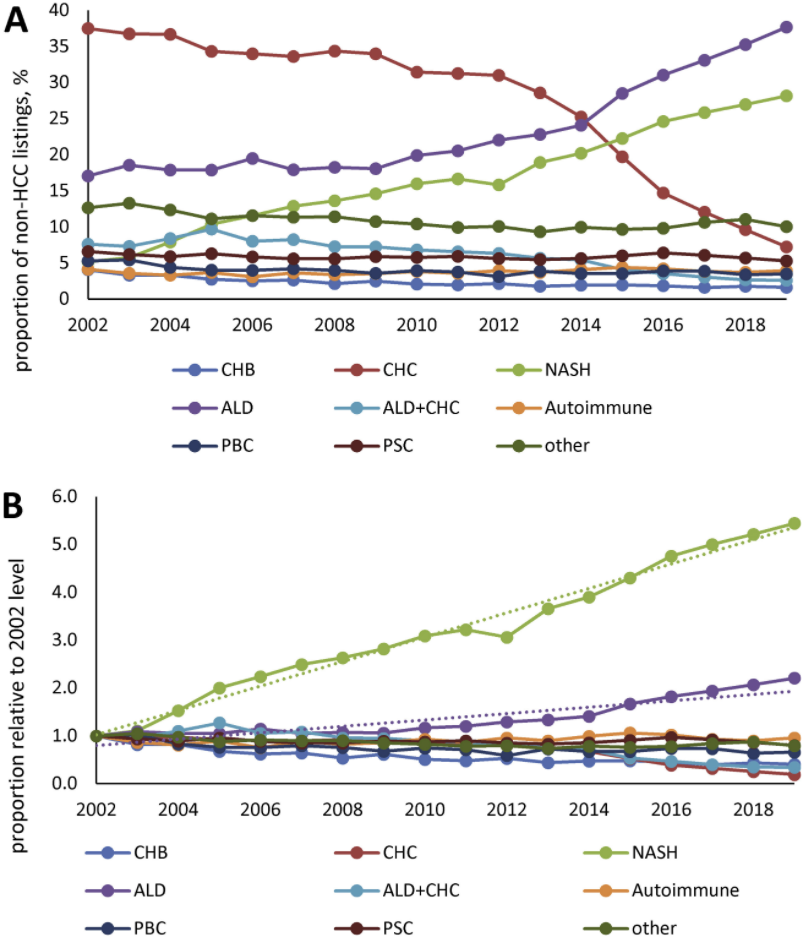
This study was an analysis of data from the Scientific Registry of Transplant Recipients (2002 through 2019).
Key findings:
In 2002, the most common etiologies of non-acute liver failure on the liver transplant waitlist (in patients without HCC)
In 2019, among patients without HCC, NASH was the second leading indication for liver transplantation (28% of patients), after ALD (38% of patients). were chronic HCV infection (37%) and ALD (16%), whereas only 5% had NASH
HCC accounted for 27,799 patients (16.5%) and was commonly due to chronic HCV throughout study period
My take: Demand for liver transplantation has NOT improved despite curative therapy for chronic hepatitis C. This is due to increased liver failure related to fatty liver disease and alcoholic liver disease.
Figure 1 Prevalence of the most common CLD etiologies in waitlisted liver transplant candidates without HCC. (A) Proportion of all non-HCC listings with known etiology; (B) the proportion relative to that seen in 2002.