CC Thompson et al. Gastointestinal Endoscopy (EPUB), in a letter to the editor, respond to two recent studies on SARS-CoV-2 virus/COVID-19 and provide recommendations for PPE use in this era of COVID-19.
Here’s a link to manuscript: COVID-19 in Endoscopy: Time to do more?
Key points:
- Reduce non-urgent cases. “We have cut our daily endoscopy volume by over 80% and closed our ambulatory endoscopy practice.”
- Increase the use of telemedicine. “At present, telemedicine or virtual visits make up 91% of our upcoming clinic appointments.”
- Physical distancing as advocated recently by WHO throughout a patient’s time in the endoscopy unit is stressed in the papers, with a 6-foot minimum between individuals.
- Suggests “the need for a separate toilet as part of the isolation to minimize spread of infection due to bioaerosols from the toilet plume”
- Our hospital system has recently changed policy to mandate that all employees wear surgical masks at all times while in the hospital and attest to their wellness online before reporting to work.
- We suggest labeling each computer so the same provider uses that computer and chair for the entire day, and separating by at least 6 feet.
- All endoscopic procedures (upper endoscopy, colonoscopy, EUS, ERCP) are aerosol-generating, referencing studies that show contamination of the endoscopist’s face during routine procedures. This makes all endoscopic procedures high risk from an infectious standpoint, and appropriate PPE is
recommended… It makes little sense for healthcare providers to perform
aerosolizing procedures, with patients coughing or passing gas on them, while not wearing an N95 mask or better - “It is important to use full PPE for all endoscopic procedures while in a pandemic such as this especially in areas with community spread, because no one is truly low risk given our ongoing difficulties with testing.”
- “The mask can be reused as long as it is functional, not soiled, and not used in a suspected or COVIDpositive patient. It is important to cover the N95 to prevent soiling.”
- “A study from China showed that no medical staff working in high-risk departments who wore N95s and practiced strict hand hygiene regardless of patient’s infection status became infected.”
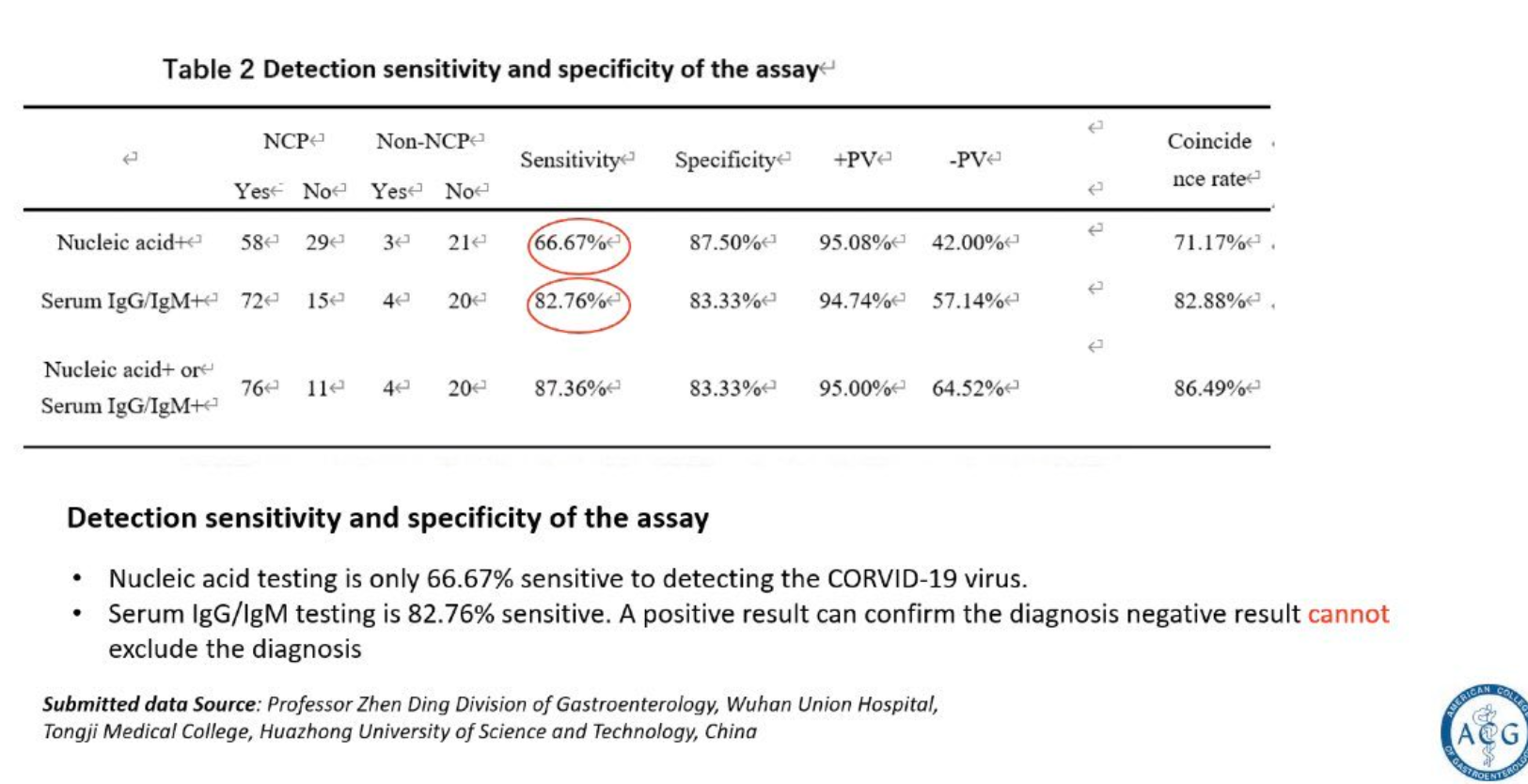
- “Testing all patients before high-risk procedures such as endoscopy is likely the best approach; however, this will depend on significant expansion of testing capabilities. Hopefully, the development of point-of-care testing with rapid results and increasing testing availability will make this a reality soon”
My take (in part from authors): “We are living through an unprecedented time and are all trying our best to protect our patients and ourselves under suboptimal conditions of limited PPE, limited testing, and limited data. ” The recommendations in this article are based mainly on expert opinion and may need modifications based on new data and circumstances.
—————————-
IOIBD (International Organization for the Study of Iinflammatory Bowel Disease) Recommendations (#76) for IBD Patients with Regard to COVID-19:
Full link: IOIBD Update on COVID19 for Patients with Crohn’s Disease and Ulcerative Colitis (3/26/20)