I had the privilege recently of introducing William Balistreri as the keynote speaker for the Georgia AAP Nutrition Symposium. Dr. Balistreri is a personal hero for me; someone I admire greatly. Hopefully, if he reads this, he will forgive me for forgetting to mention in my introduction that he also is a Lacrosse coach for one of his grandchildren’s team.
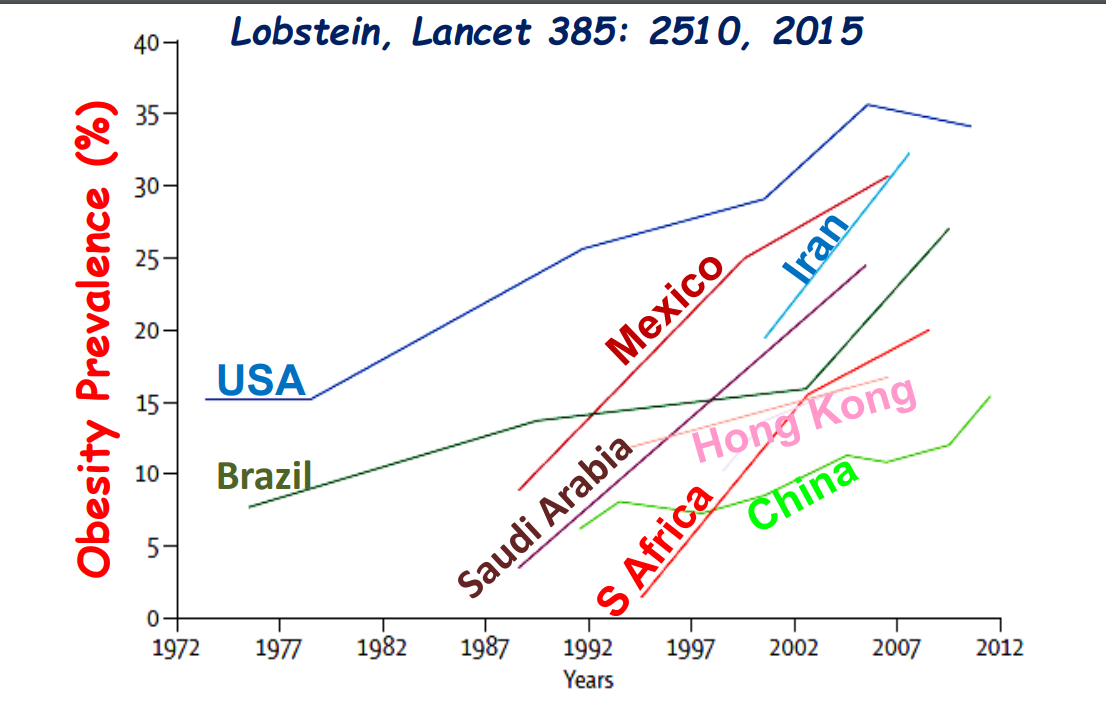
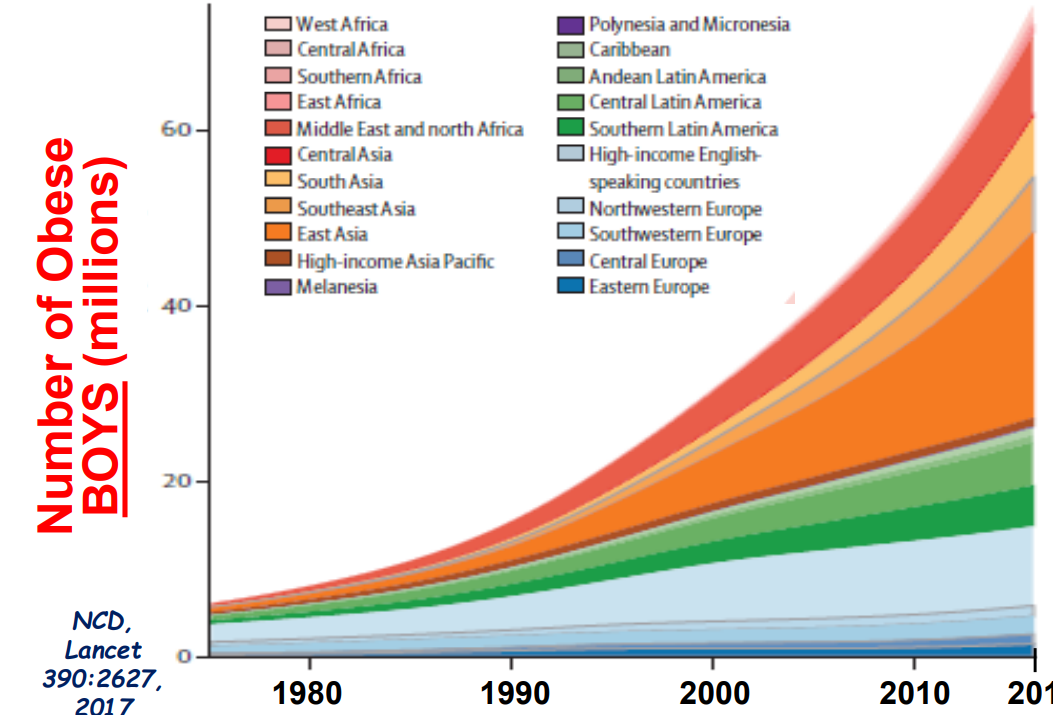
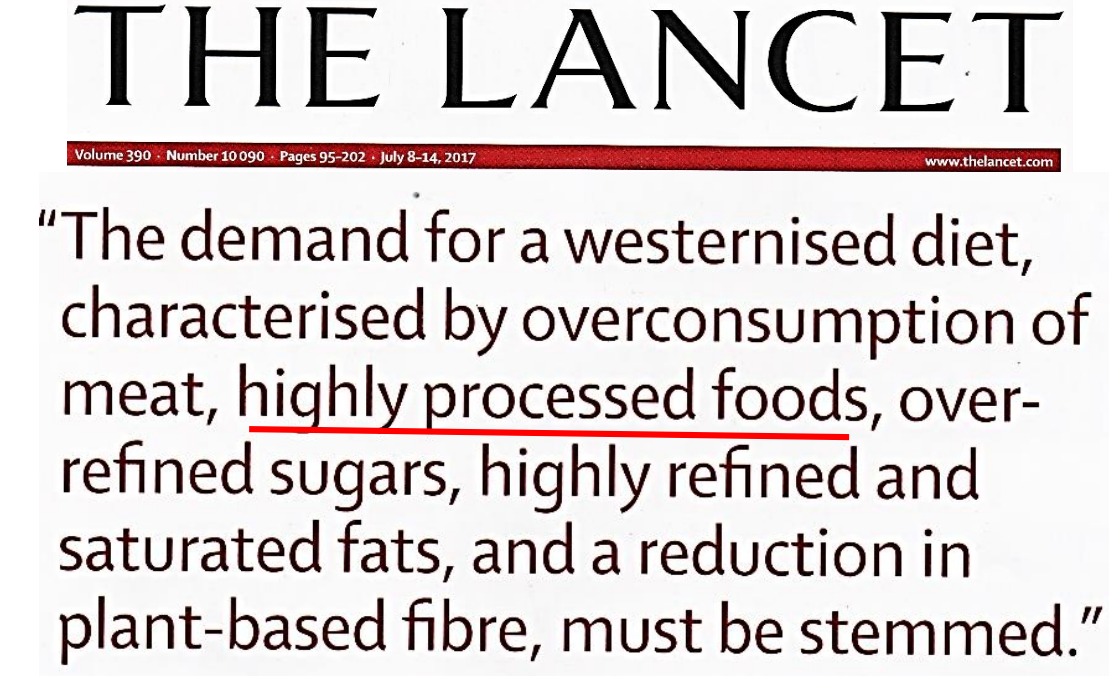
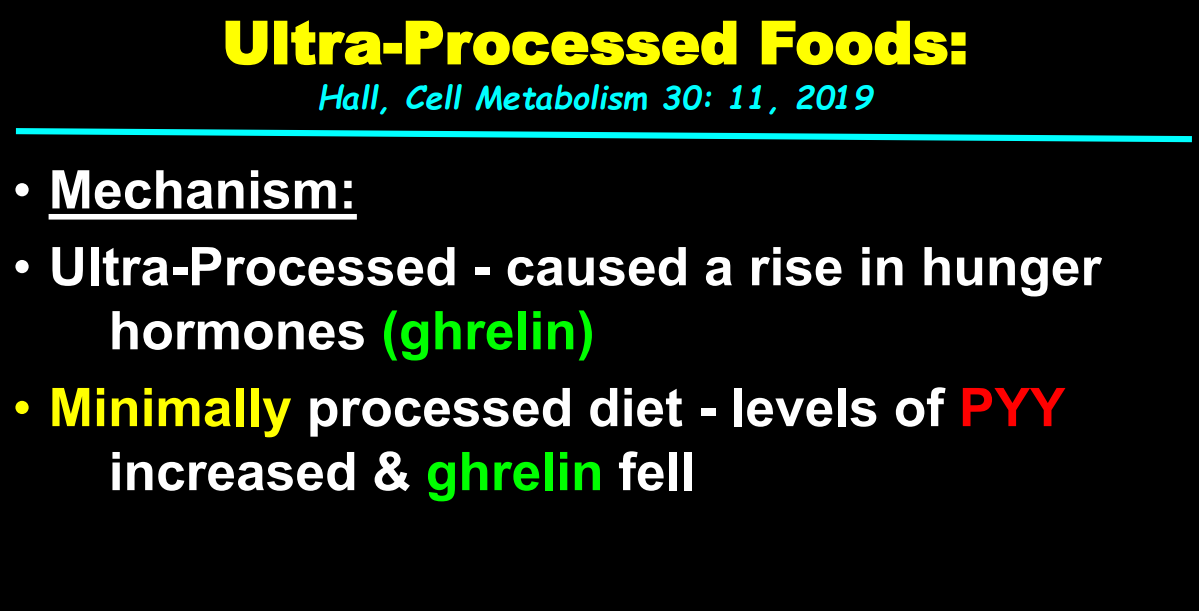
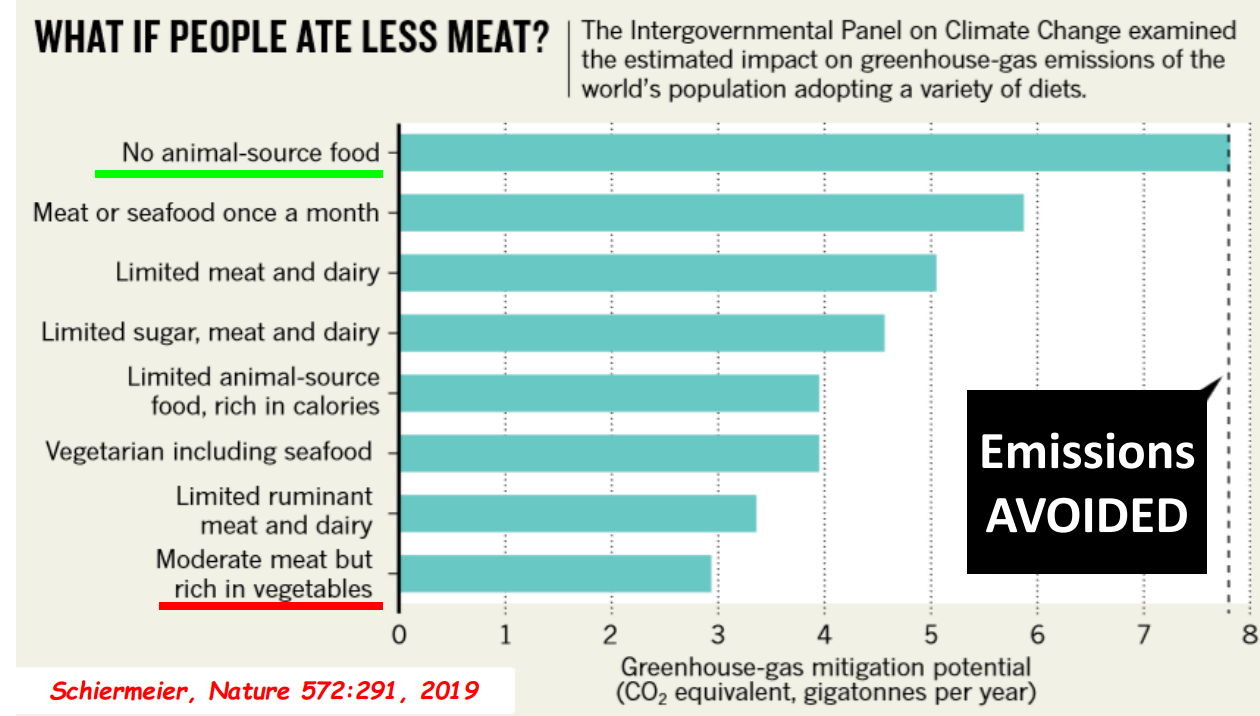
He gave a tour de force presentation on the global challenge of obesity. In addition, he discussed undernutrition, endobariatrics, gastroenteritis, climate change and even food waste; 40% of U.S. food is thrown away. In Finland, there is a ‘Grocery Store Happy Hour‘ for distribution of reduced cost/free groceries which may help reduce food waste. In general, I try to condense what I read or hear –that was pretty much impossible with this lecture which was packed with information based on the latest research as well as information dating back to the 5th Century BC/Plato. What follows are some of my favorite slides.
Here is a link to the full talk: WHAT’S HOT in Pediatric Gastroenterology? Global Nutrition Lecture (10-10-19)
Two Articles received the most attention:
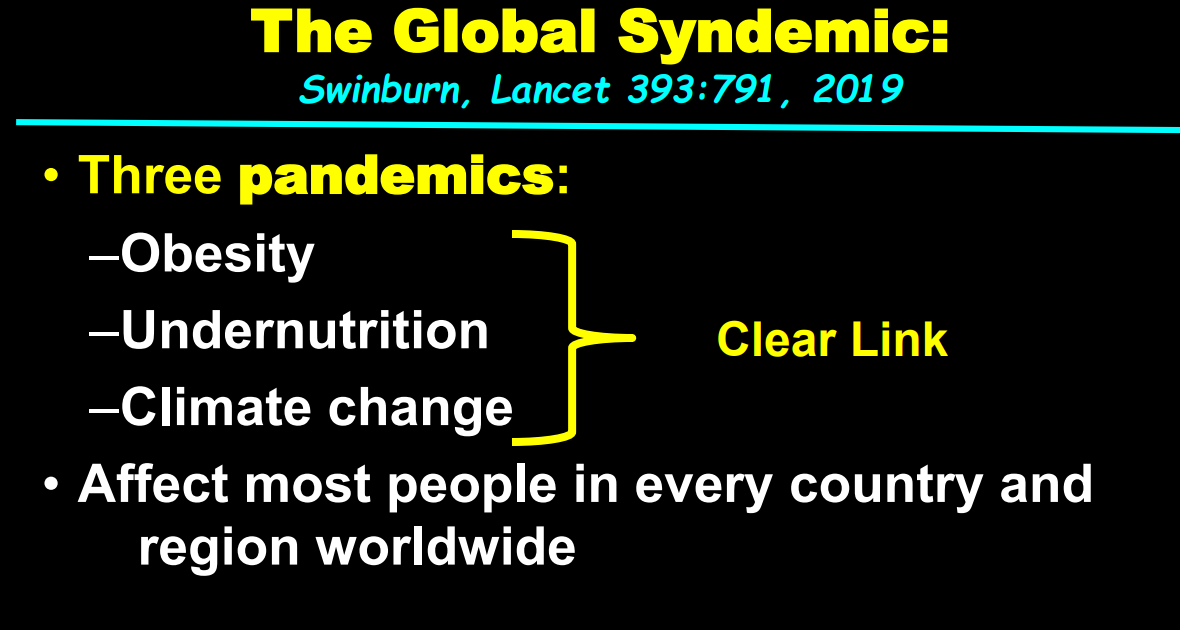
- LANCET Commission on Global Syndemic (Obesity, Undernuturition, and Climate Change)
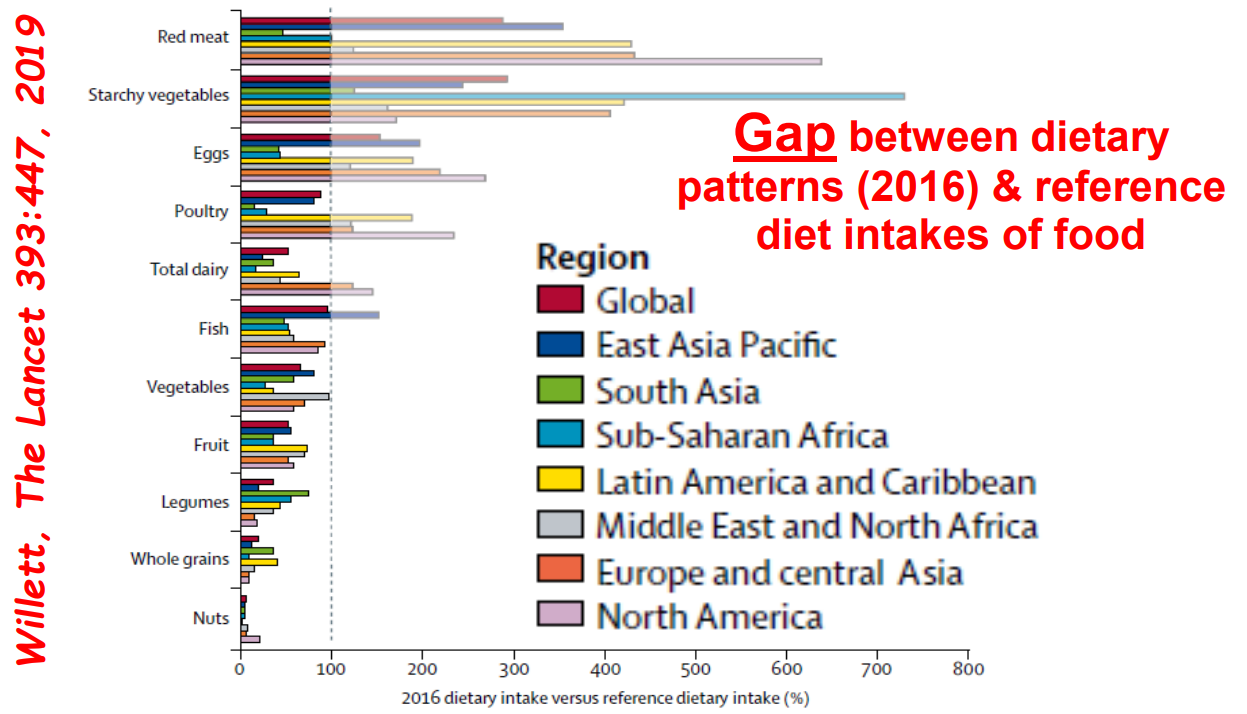
- EAT- LANCET Commission on Healthy Diets

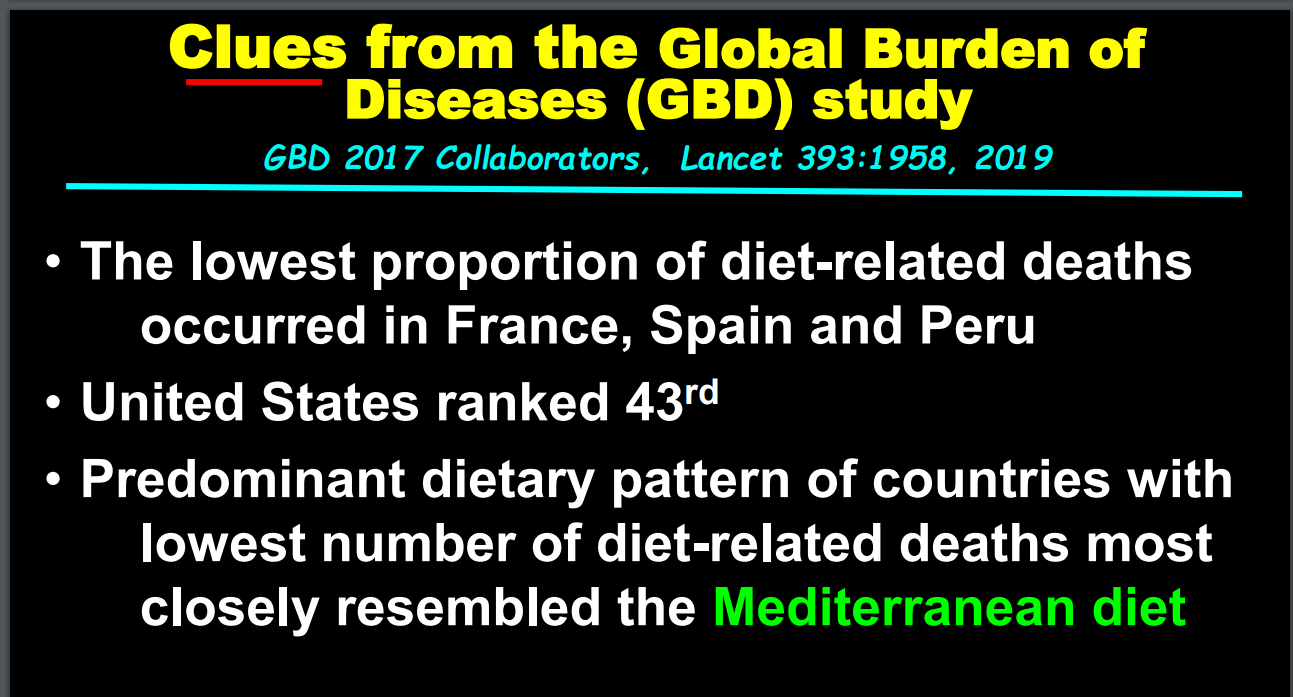
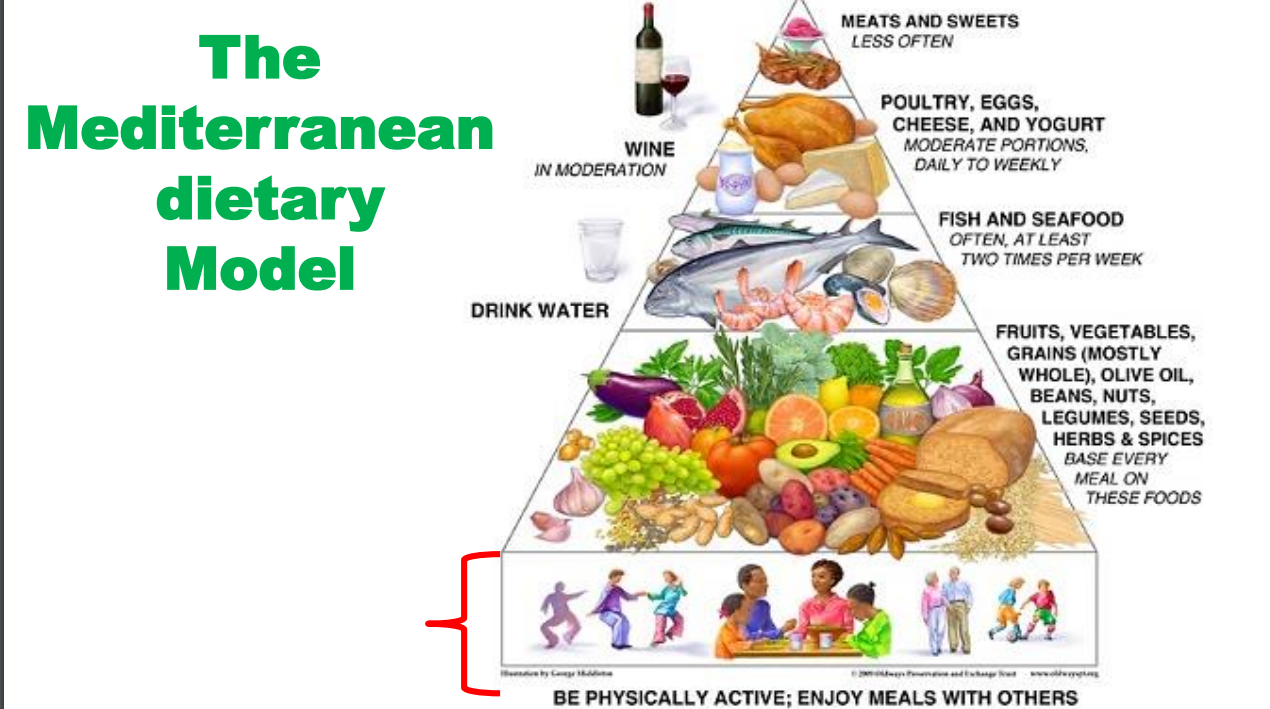
What Can Be Done?
Additional References:
A recent book (not discussed in lecture) provides related information. “We Are The Weather” by Jonathan Foer, was reviewed this past weekend in the NY Times: Meat is Murder: “[This book] has a point, and that is to persuade us to eat fewer animal products. Foer makes the case that, for Americans and citizens of other voracious meat-eating countries, this is the most important individual change we can make to reduce our carbon footprints.” However, the reviewer, Mark Bittman, states that “we’re not good at making positive decisions about our future. And we’re really not good at denying ourselves cheap pleasures like cheeseburgers.” He advocates for stronger laws, government leadership, and pricing the products to account for their true costs in terms of their contributions to climate change, public health, and environmental degradation.
Related blog posts:
- NY Times: “Our Food is Killing Too Many of Us”
- Bad diets –>High Mortality
- Better Diet, Lower Mortality
- Big Data for Personalized Diets
- Why Fiber Matters?
- Nutrition Week (Day 7) Connecting Epidemiology and Diet in Inflammatory Bowel Disease
- Life Cut Short by Obesity