There have been studies suggesting that antibiotics at a young age promote obesity and other studies that have NOT found an association. A recent study (could not find an effect of chronic prophylactic antibiotics.
Link: Weight Gain and Obesity in Infants and Young Children Exposed to Prolonged Antibiotic Prophylaxis
From Abstract:
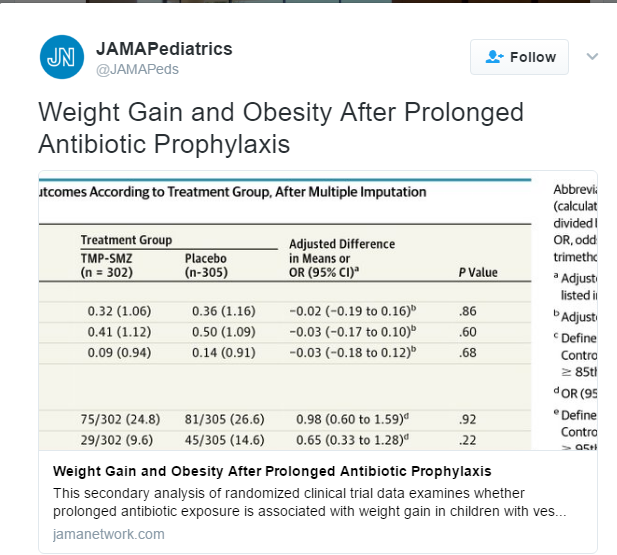
Design, Setting, and Participants Secondary analysis of data from the Randomized Intervention for Children With Vesicoureteral Reflux Study, a 2-year randomized clinical trial that enrolled participants from 2007 to 2011. All 607 children who were randomized to receive antibiotic (n = 302) or placebo (n = 305) were included. Children with urinary tract anomalies, premature birth, or major comorbidities were excluded from participation.
Interventions Trimethoprim-sulfamethoxazole or placebo taken orally, once daily, for 2 years.
Results Participants had a median age of 12 months (range, 2-71 months) and 558 of 607 (91.9%) were female. Anthropometric data were complete at the 24-month visit for 428 children (214 in the trimethoprim-sulfamethoxazole group and 214 in the placebo group). Weight gain in the trimethoprim-sulfamethoxazole group and the placebo group was similar (mean [SD] change in weight-for-age z score: +0.14 [0.83] and +0.18 [0.85], respectively; difference, −0.04 [95% CI, −0.19 to 0.12]; P = .65). There was no significant difference in weight gain at 6, 12, or 18 months or in the prevalence of overweight or obesity at 24 months (24.8% vs 25.7%; P = .82). Subgroup analyses showed no significant interaction between weight gain effect and age, sex, history of breastfeeding, prior antibiotic use, adherence to study medication, or development of urinary tract infection during the study.
My take: Whether antibiotics could contribute to obesity is not entirely clear –even the possibility could encourage better stewardship of antimicrobials.
Related blog posts:
- NY Times: Frequent Antibiotics May Make Children Fatter
- Could antibiotics make you fat? | gutsandgrowth
- Could Obesity Be Cured/Created at Birth with Manipulation of …
- Missing Bacteria in Refractory Malnutrition | gutsandgrowth
- Preterm Neonatal Microbiota and Effect of Perinatal …
- Early Antibiotics and Obesity | gutsandgrowth