About gutsandgrowth
I am a pediatric gastroenterologist at GI Care for Kids (previously called CCDHC) in Atlanta, Georgia. The goal of my blog is to share some of my reading in my field more broadly. In addition, I wanted to provide my voice to a wide range of topics that often have inaccurate or incomplete information.
Before starting this blog in 2011, I would tear out articles from journals and/or keep notes in a palm pilot. This blog helps provide an updated source of information that is easy to access and search, along with links to useful multimedia sources.
I was born and raised in Chattanooga. After graduating from the University of Virginia, I attended Baylor College of Medicine. I completed residency and fellowship training at the University of Cincinnati at the Children’s Hospital Medical Center. I received funding from the National Institutes of Health for molecular biology research of the gastrointestinal tract.
During my fellowship, I had the opportunity to work with some of the most amazing pediatric gastroenterologists and mentors. Some of these individuals included Mitchell Cohen, William Balistreri, James Heubi, Jorge Bezerra, Colin Rudolph, John Bucuvalas, and Michael Farrell. I am grateful for their teaching and their friendship. During my training with their help, I received a nationwide award for the best research by a GI fellow.
I have authored numerous publications/presentations including original research, case reports, review articles, and textbook chapters on various pediatric gastrointestinal problems. In addition, I have been recognized by Atlanta Magazine as a "Top Doctor" in my field multiple times.
Currently, I am the vice chair of the section of nutrition for the Georgia Chapter of the American Academy of Pediatrics. In addition, I am an adjunct Associate Clinical Professor of Pediatrics at Emory University School of Medicine. Other society memberships have included the North American Society for Pediatric Gastroenterology Hepatology and Nutrition (NASPGHAN), American Academy of Pediatrics, the Food Allergy Network, the American Gastroenterology Association, the American Association for the Study of Liver Diseases, and the Crohn’s and Colitis Foundation.
As part of a national pediatric GI organization called NASPGHAN (and its affiliated website GIKids), I have helped develop educational materials on a wide-range of gastrointestinal and liver diseases which are used across the country. Also, I have been an invited speaker for national campaigns to improve the evaluation and treatment of gastroesophageal reflux disease, celiac disease, eosinophilic esophagitis, hepatitis C, and inflammatory bowel disease (IBD). Some information on these topics has been posted at my work website, www.gicareforkids.com, which has links to multiple other useful resources.
I am fortunate to work at GI Care For Kids. Our group has 17 terrific physicians with a wide range of subspecialization, including liver diseases, feeding disorders, eosinophilic diseases, inflammatory bowel disease, cystic fibrosis, DiGeorge/22q, celiac disease, and motility disorders. Many of our physicians are recognized nationally for their achievements. Our group of physicians have worked closely together for many years. None of the physicians in our group have ever left to join other groups. I have also worked with the same nurse (Bernadette) since I moved to Atlanta in 1997.
For many families, more practical matters about our office include the following:
– 14 office/satellite locations
– physicians who speak Spanish
– cutting edge research
– on-site nutritionists
– on-site psychology support for abdominal pain and feeding disorders
– participation in ImproveCareNow to better the outcomes for children with inflammatory bowel disease
– office endoscopy suite (lower costs and easier scheduling)
– office infusion center (lower costs and easier for families)
– easy access to nursing advice (each physician has at least one nurse)
I am married and have two sons (both adults). I like to read, walk/hike, bike, swim, and play tennis with my free time.
I do not have any financial relationships with pharmaceutical companies or other financial relationships to disclose. I have helped enroll patients in industry-sponsored research studies.
A recent study on a new monoclonal antibody to prevent Clostridium difficile infection is available from the NEJM. Here’s the link: Preventing Clostridium difficile Infection Recurrence

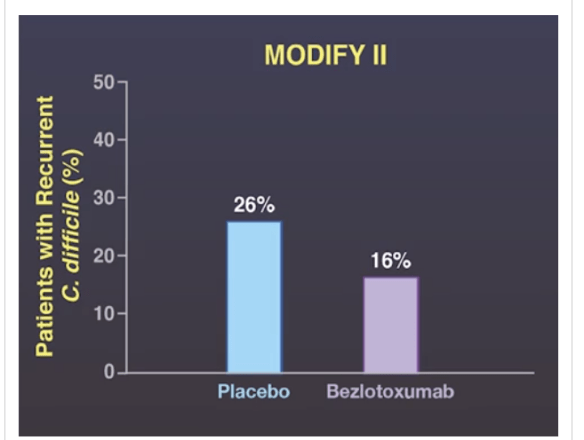
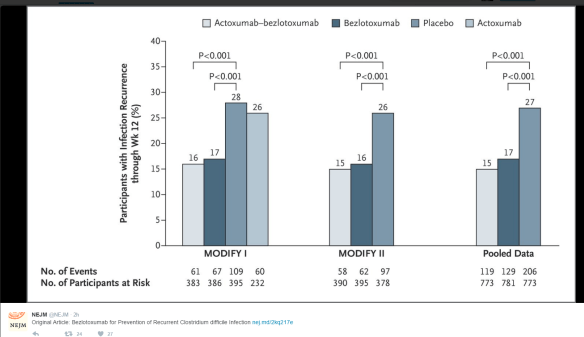
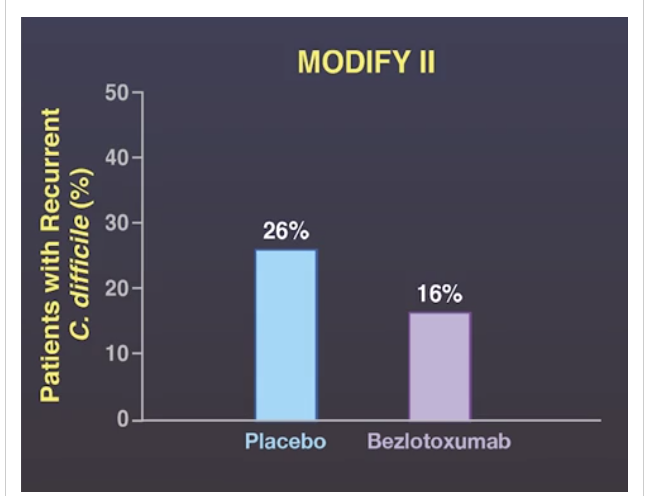
My take: In Modify I and Modify II, Bezlotoxumab reduced the rate of Clostridium difficile recurrence in elderly patients (median age 66 years). In a high risk patients, the likely hefty cost of this medication may be warranted.
These studies were likely pivotal in receiving FDA approval: FDA Approves Merck’s ZINPLAVA™ (bezlotoxumab) to Reduce Recurrence of Clostridium difficile Infection
A recent study (ALT Ma et al. J Pediatr 2016; 179: 216-8) reaches a conclusion that questions the cost-effectiveness of pretreatment TPMT activity in pediatric patients. In my opinion, this retrospective study is ridiculous. Here’s why:
The authors examined thiopurine transmethyltransferase (TPMT level) in 228 children before starting a thiopurine. They found the following:
- Only 2 patients experienced mild neutropenia
- 12% of their cohort had intermediate activity and 88% normal TPMT activity
I agree with their conclusion that routine blood tests are needed following institution of thiopurines, I think stating that “from an economic point of view –the cost for testing TPMT enzyme activity was high without major clinical benefit” cannot be made with such a small study. Deficient TPMT activity occurs in about 1 in 300. If a single patient develops bone marrow suppression due to a thiopurine medication, this can lead to a horrific and prolonged hospitalization. The cost of such a hospitalization, both economically and emotionally, is enormous.
My take: If I were taking a thiopurine, I would want to know if I metabolized this medication at a slower rate and was at increased risk for bone marrow suppression. My hunch is the authors would not forgo checking a TPMT level on themselves despite their study’s conclusion, particularly if they have ever witnessed a patient with thiopurine-induced bone marrow suppression.
Related blog posts:

Grand Prismatic Spriing, Yellowstone
U Lantto et al. J Pediatr 2016; 179: 172-7. This retrospective study showed that tonsillectomy was highly effective in children with PFAPA (periodic fever, aphthous stomatitis, pharyngitis, and adenitis) -both those with classic features and incomplete features.
“In the group that met Thomas criteria, 97% (56/58) had complete resolution of fever episodes after tonsillectomy; in the group that did not meet Thomas criteria (50/50) had complete resolution.”
Thomas criteria:
- Recurring fevers with early age of onset (<5 years) [the authors suggest a minimum of 5 episodes]
- Constitutional symptoms in the absence of over upper respiratory infection with at least one of the following: aphthae, cervical adenitis, pharyngitis
- Exclusion of cyclic neutropenia
- Completely asymptomatic interval between episodes
- Normal growth and development

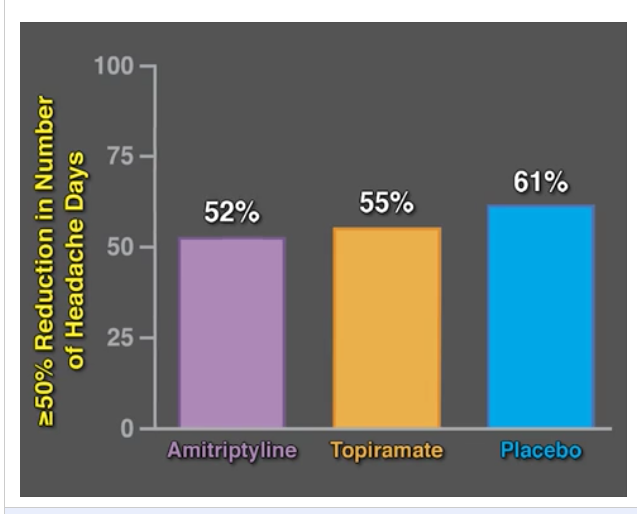
For those who missed this important pediatric study, a quick take ~2 min video link: Pediatric Migraine CHAMP Study


Related blog post: Topamax and Amitriptyline Did Not Work for Pediatric Migraines
My take: It looks like placebo did pretty well with >60% response rate. In a commentary on this subject, the authors noted that when patients are seen by the physician, the symptoms are often severe. So, some improvement is expected, in part, due to regression to the mean; that is, it is common to return to their baseline level of symptoms.
From A Riskin et al. Pediatrics Jan 2017 (Thanks to Seth Marcus for pointing out this study), Link: Rudeness and Medical Team Performance
Abstract
OBJECTIVES: Rudeness is routinely experienced by medical teams. We sought to explore the impact of rudeness on medical teams’ performance and test interventions that might mitigate its negative consequences.
METHODS: Thirty-nine NICU teams participated in a training workshop including simulations of acute care of term and preterm newborns. In each workshop, 2 teams were randomly assigned to either an exposure to rudeness (in which the comments of the patient’s mother included rude statements completely unrelated to the teams’ performance) or control (neutral comments) condition, and 2 additional teams were assigned to rudeness with either a preventative (cognitive bias modification [CBM]) or therapeutic (narrative) intervention. Simulation sessions were evaluated by 2 independent judges, blind to team exposure, who used structured questionnaires to assess team performance.
RESULTS: Rudeness had adverse consequences not only on diagnostic and intervention parameters (mean therapeutic score 3.81 ± 0.36 vs 4.31 ± 0.35 in controls, P < .01), but also on team processes (such as information and workload sharing, helping and communication) central to patient care (mean teamwork score 4.04 ± 0.34 vs 4.43 ± 0.37, P < .05). CBM mitigated most of these adverse effects of rudeness, but the postexposure narrative intervention had no significant effect.
CONCLUSIONS: Rudeness has robust, deleterious effects on the performance of medical teams. Moreover, exposure to rudeness debilitated the very collaborative mechanisms recognized as essential for patient care and safety. Interventions focusing on teaching medical professionals to implicitly avoid cognitive distraction such as CBM may offer a means to mitigate the adverse consequences of behaviors that, unfortunately, cannot be prevented.
This same group had a related study in 2015:The Impact of Rudeness on Medical Team Performance: A Randomized Trial
My take:The saying “you catch more flies with honey than you do with vinegar” is probably accurate.

Costa Maya, Mexico
A cautionary note on biosimilars has been discussed in a recent review (DT Rubin et al. Gastroenterol & Hepatol 2016; 12: 741-51)
In the recently completed NOR-SWITCH study presented at the United European Gastroenterology Week 2016 meeting, “a total of 481 patients were recruited across 40 centers: all patients had been on stable treatment with the originator infliximab for at least 6 months…When looking specifically at IBD patients, disease worsening was noted in 21.2% of originator infliximab-treated patients and 36.5% of CT-P13-treated Crohn’s disease patients (n=155).” The 15% difference did not reach statistical significance, but is concerning. The authors state that “subtle postranslational modifications unique to the biosimilars may be sufficient to lead to antidrug antibody formation with associated loss of response. Also, it is noted that this study did not include endoscopic evaluation.
The authors note that therapeutic monitoring worked with biosimilar product using available infliximab assays.
My take: We still have a lot to learn. The preliminary message, until more studies are available, indicate that switching stable patients could increase risk of losing response.
Related blog posts:

Puerto Rico
A recent study (ML Basiaga et al. J Pediatr 2016; 179: 226-32) highlights the large variation in care for 701 children receiving steroids (for at least 15 days) at a leading children’s hospital (CHOP). I think, given the fact that this is a retrospective study and the huge variation in steroid exposure, the message regarding variation should not be taken that seriously. But, the article does suggest that in children with chronic glucocorticoid therapy, several measures should be considered:
- Bone health -particularly Vitamin D (25-OH) levels
- Immunity -particularly assuring pneumococcal and influenza vaccines
- Lipid screening
- Stress steroid plan. The authors indicate that the endocrinology society recommendations have included instructing parents in intramuscular hydrocortisone in case of vomiting or severe stress.
My take: Having a standard approach to an at-risk group makes sense, however, “whether implementation of preventive care guidelines improves outcomes in children” is not known.

A recent study (JM Garbutt et al. J Pediatr 2016; 179: 166-71 and related editorial by MD Dowd, pg 15-17) provide relevant information on the issue of firearm injury prevention.
The study describes the results of a survey provided to 1246 parents at a diverse group of practices around St Louis.
Key findings:
- 36% reported being owners of firearms
- Of the owners, 25% reported ≥1 firearm was stored loaded and 17.9% carried a firearm when leaving the house.
- 75% of all parents thought pediatricians should provide advise on safe storage of firearms (71% of owners); however, only 12.8% of all parents reported a discussion about firearms with the pediatrician
The discussion and commentary on this study are more interesting than the actual results. Key points:
- The AAP has recommended that pediatricians screen for the presence of household firearms and has stated that a “home without guns is the safest option…Advising safe storage is also encouraged.” Prior surveys have echoed this study that few pediatricians counsel families about firearm safety.
- Despite AAP recommendations, over “60% of Americans believe that a ‘gun in the house makes it safer’ which is a more common attitude than in 2004 when 42% of Americans held that view.
- Providing a child with firearm avoidance educational programs (eg. NRA’s “Eddie Eagle”) “is unlikely to lead to safe behaviors…[and] may give parents a false sense of security.”
- “Children cannot distinguish real guns from toy guns and are strong enough to pull a trigger as early as 3 years of age.”
- Approaching the topic of safe storage “as an expert in child development” and children’s unpredictable behavior rather than in firearm safety “may be acceptable to both pediatricians and parents.”
- The authors advocate keeping firearm storage on a checklist of hazards (eg. medication storage, avoiding household poisons) –though this has not been well-studied.
- From editorial: “When compared with other developed nations, US children under 15 years of age are 12 times more likely to be killed by a gun…We know that nearly 1 in 10 families with guns admit to keeping at least 1 gun loaded and unlocked, and nearly one-half keep at least 1 gun unlocked.”
So, in fact, having a gun in the home does not make a home safer, just the opposite. But delving into this topic is probably not productive due to strong feelings tangential to gun ownership. There have been unsuccessful legislative efforts in over 10 states to prevent physicians from discussing the topic as well as a protracted legal battle in Florida.
My take (borrowed from editorial): “Although the difference between “gun safety” and “child safety” may seem subtle, such a shift allows a consistent approach to home injury prevention across mechanisms of injury with the focus on the child, not the gun.” “Little children are curious and big children (teens) are impulsive, so exposure to unsecured guns can lead to tragic outcomes that cannot be prevented by child education. Who better to deliver this message than pediatricians?”
Related blog posts:

A soon-to-be-published study (available online Hepatology) from WF Balistreri et al shows that the combination of Ledipasvir-Sofosbuvir is highly effective in pediatric patients aged 12-17 years.
Here is the abstract:
ABSTRACT
No all-oral, direct-acting antiviral regimens have been approved for children with chronic hepatitis C virus (HCV) infection. We conducted a Phase 2, multi-center, open-label study to evaluate the efficacy and safety of ledipasvir–sofosbuvir in adolescents with chronic HCV genotype 1 infection. One hundred patients ages 12 to 17 years received a combination tablet of 90 mg ledipasvir and 400 mg sofosbuvir once daily for 12 weeks. On the 10th day following initiation of dosing, 10 patients underwent an intensive pharmacokinetic evaluation of the concentrations of sofosbuvir, ledipasvir, and the sofosbuvir metabolite GS-331007. The primary efficacy endpoint was the percentage of patients with a sustained virologic response 12 weeks posttreatment (SVR12). Median age of patients was 15 years (range, 12-17 years). A majority (80%) were HCV treatment naïve, and 84% were infected through perinatal transmission. One patient had cirrhosis and 42 did not; in 57 patients the degree of fibrosis was unknown. Overall, 98% (98/100; 95% CI, 93% to 100%) of patients reached SVR12. No patient had virologic failure. The 2 patients who did not achieve SVR12 were lost to follow-up either during or after treatment. The 3 most commonly reported adverse events were headache (27% of patients), diarrhea (14%), and fatigue (13%). No serious adverse events were reported. AUCtau and Cmax values for sofosbuvir, ledipasvir, and GS-331007 were within the predefined pharmacokinetic equivalence boundaries of 50% to 200% when compared with adults from Phase 2 and 3 studies of ledipasvir and sofosbuvir. Conclusion: Ledipasvir−sofosbuvir was highly effective in treating adolescents with chronic HCV genotype 1 infection. The dose of ledipasvir−sofosbuvir currently used in adults was well tolerated in adolescents and had an appropriate pharmacokinetic profile.
My take: This is great news for pediatric patients. This study indicates that this breakthrough therapy (and likely others) for adults will become more widely available for pediatric patients soon.

TV sports analysts have tremendous insight! Virginia needs to score enough points to win.