JD Feuerstein et al. Clin Gastroenterol Hepatol 2025; 23: 2068-2082. Open Access! Appropriate Use and Complications of Corticosteroids in Inflammatory Bowel Disease: A Comprehensive Review
Steroids are commonly used and misused for inflammatory bowel disease. This article reviews best practices, steroid formulations/dosing, and potential complications.
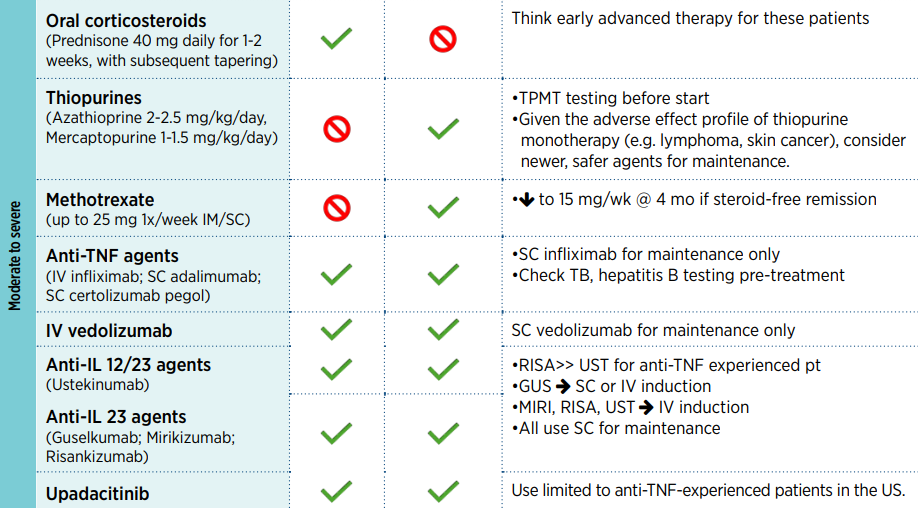
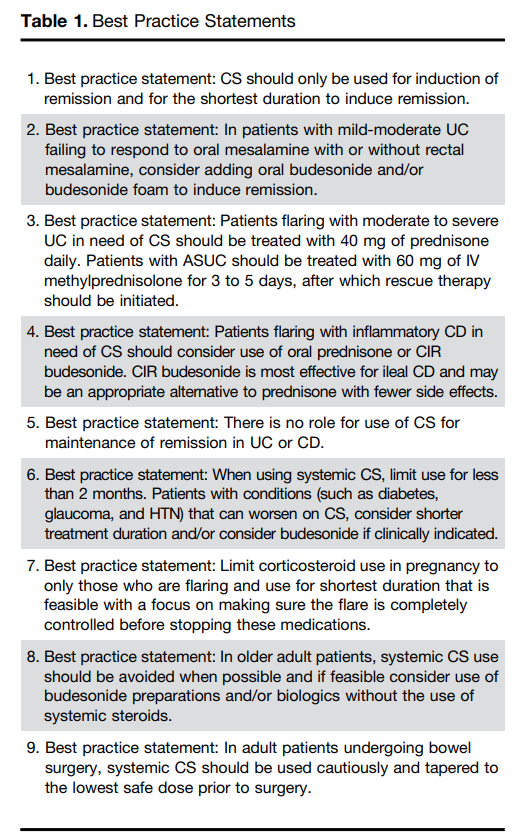
- For moderate to severe ulcerative colitis (in adults), the authors recommend treatment with 40 mg of prednisone daily. Patients with ASUC (acute severe ulcerative colitis) should be treated with 60 mg of IV methylprednisolone for 3 to 5 days, after which rescue therapy should be initiated
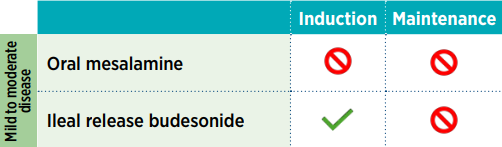
- Use of budesonide is recommended as an option for many clinical situations to minimize steroid adverse effects. These situations include mild-moderate UC failing to respond to mesalamine, ileal CD and older patients
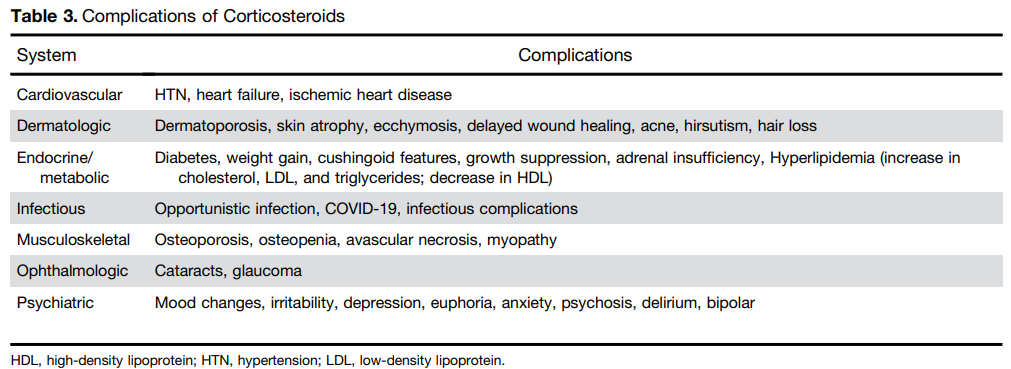
- Postoperative complications: “In the postoperative period, patients treated with CS had a higher risk of both infectious complications (aOR, 3.69; 95% CI, 1.24–10.97) and major infectious complications (aOR, 5.54; 95% CI, 1.12–27.26) [Abrerra et al].135 Subramanian pooled data from 7 studies showing that preoperative CS use is associated with increased postoperative complications (OR, 1.41; 95% CI, 1.07–1.87) as well as infectious complications.
The authors note that corticosteroids “remain widely available and are an effective short-term option for induction of remission in patients with active UC or inflammatory CD. However, their well-described and significant safety profile warrants proactive strategies to limit their use through non-systemic formulations, short-term exposures, steroid-sparing maintenance options, and most recently, complete steroid avoidance strategies.”
My take: Continuing steroids when they are not effective prior to potential surgery (eg. ASUC) remains a frequent problem. Sometimes, it is difficult to know it they are helping some.