One of the major leaps forward in gut science began with an accidental shooting at a trading post on June 6, 1822. A fur trader named Alexis St. Martin took a bullet in the abdomen, leaving him with a hole ripped through his muscle, bone and internal organs…
His doctor, William Beaumont, could literally tie a bit of food on a string, shove it into St. Martin’s stomach through the hole, and pull it back out again. Using this one weird trick, Beaumont extracted samples of the man’s gastric juices. Over eight years and more than 200 awkwardly invasive experiments, St. Martin and Beaumont gave humanity its first real understanding of how digestion works.
Last year, the ACCURE Trial (see blog post link below), showed that laparoscopic appendicectomy, in addition to standard medical therapy, significantly reduced the relapse rates for ulcerative colitis (UC) within 1 year. Most patients were treated with mesalamine.
The COSTA study examined adult patients (n=125) who were not responding to advanced therapy. Patients were offered one of three treatments: laparoscopic appendicectomy while continuing their existing advanced therapy at a stable dose; switching their advanced therapy to a JAK inhibitor; or colectomy. 116 patients were included in the modified intention-to-treat-analysis (67 received appendicectomy and 49 received JAK inhibitor (primarily tofacitinib).
Key findings:
22 (32.8%) of 67 patients in the appendicectomy group were in clinical remission without therapy failure at 12 months compared with six (12.2%) of 49 patients in the JAK inhibitor group (p=0.016)
At 12 months, corticosteroid-free clinical remission without therapy failure was attained in 22 (32.8%) of 67 patients in the appendicectomy group compared with six (12.2%) of 49 patients in the JAK inhibitor group (p=0.010). Clinical response in 49 (73.1%) of 67 patients compared with 26 (53.1%) of 49 patients (p=0·025), and endoscopic response in 31 (48.4%) of 64 patients compared with 11 (25.6%) of 43 patients (p=0·018)
My take (borrowed in part from the authors): “Appendicectomy as an adjunct to advanced therapy in biologic-exposed patients with active ulcerative colitis was associated with higher clinical remission rates at 12 months compared with switching to a JAK inhibitor.” We don’t know how appendectomy would influence disease course in pediatric patients. We also don’t know how this information will be incorporated into adult guidelines.
Interestingly, there have been studies (two cited below) indicating that appendectomy lowers the risk of developing inflammatory bowel disease:
RE Andersson et al. NEJM 2001;344:808-814.Appendectomy and Protection against Ulcerative Colitis. Conclusion: “Appendectomy for an inflammatory condition (appendicitis or lymphadenitis) but not for nonspecific abdominal pain is associated with a low risk of subsequent ulcerative colitis. This inverse relation is limited to patients who undergo surgery before the age of 20 years.”
There is a well-described “evidence-practice gap” which has been cited to describe the lag between initial discovery and widespread, evidence-based clinical implementation (M Beauchemin et al. ANS Adv Nurs Sci. 2019 Oct-Dec;42(4):307–324); it has been suggested that this gap is typically about 17 years.
I was looking this up after reading a “practice tips” article on H pylori and was surprised at how infrequentlly practitioners follow guidelines for optimal treatment.
Background: “The American College of Gastroenterology (ACG) recently published H pylori management guidelines6 with significant updates to the prior recommendations published in 2017.7 Importantly, the 2017 management guidelines relied heavily upon extrapolation from studies performed outside of North America. Since then, new data from US patients have become available that highlights the rising rates of resistance of commonly used antibiotics for treatment of H pylori.”
Key points:
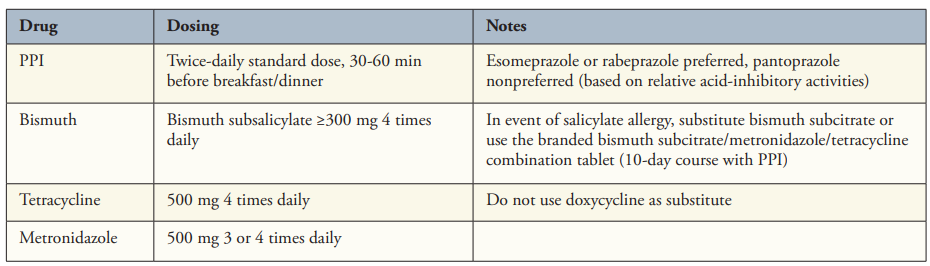
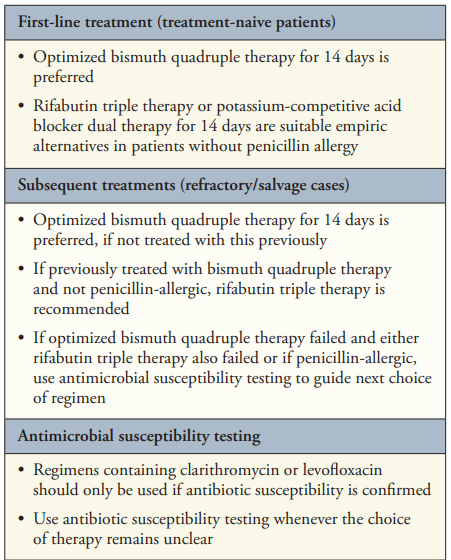
“Bismuth Quadruple Therapy Is First Line and Should Be Optimized” (see below). A 14-day course is recommended (except when using Pylera which is a 10 day treatment).
“3 new regimens have received US Food and Drug Administration (FDA) approval for H pylori therapy, each based on high levels of gastric acid inhibition. “
“The first is a combination tablet of rifabutin with amoxicillin and omeprazole (Talicia, RedHill Biopharma), given in daily doses of 150 mg, 3 g, and 120 mg, respectively. If the combination tablet is not available, generic equivalents can be substituted at similar doses (omeprazole 40 mg and amoxicillin 1 g each 3 times daily). Because the lowest available dose of generic rifabutin is only 150 mg, the best option is likely 150 mg twice daily”
“The second regimen is based on vonoprazan (Voquezna, Phathom Pharmaceuticals), the first potassium-competitive acid blocker (P-CAB) approved in the United States. substituting the P-CAB vonoprazan for lansoprazole in clarithromycin triple therapy produced higher eradication rates (81% compared with 69%). Similar statistically high rates (77%) were achieved with a dual vonoprazan-amoxicillin combination in the same trial, leading to FDA approval of both the triple and dual regimens14“
For “both rifabutin- and vonoprazan-containing regimens use amoxicillin and cannot be used in the confirmed penicillin-allergic patient. For patients with unproven penicillin allergy (approximately 10% of the US population), allergy testing is recommended”
“Use Clarithromycin or Levofloxacin Only If Antimicrobial Susceptibility Is Confirmed“
“The majority of practitioners continue to use clarithromycin-based triple therapy and have not followed the 2017 ACG H pylori guidelines …It is striking that clarithromycin-PPI triple therapy still dominates the US market, comprising greater than 80% of all treatments in 2016 to 2019.11 Notably, in approximately half of the cases where clarithromycin-PPI triple therapy failed, exactly the same prescription was given a second time.11 Thus, a massive implementation gap exists.”
My take:
While this article focuses on adult guidelines, there are similar issues in pediatrics. There is an even greater need for research involving children with H pylori. As vonoprazan appears to improve eradication rates, more guidance is needed regarding drug regimens with vonoprazan in kids.
I frequently see patients who have received empiric clarithromycin-based therapy. Based on this article, I should be less surprised that this is so commonplace.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
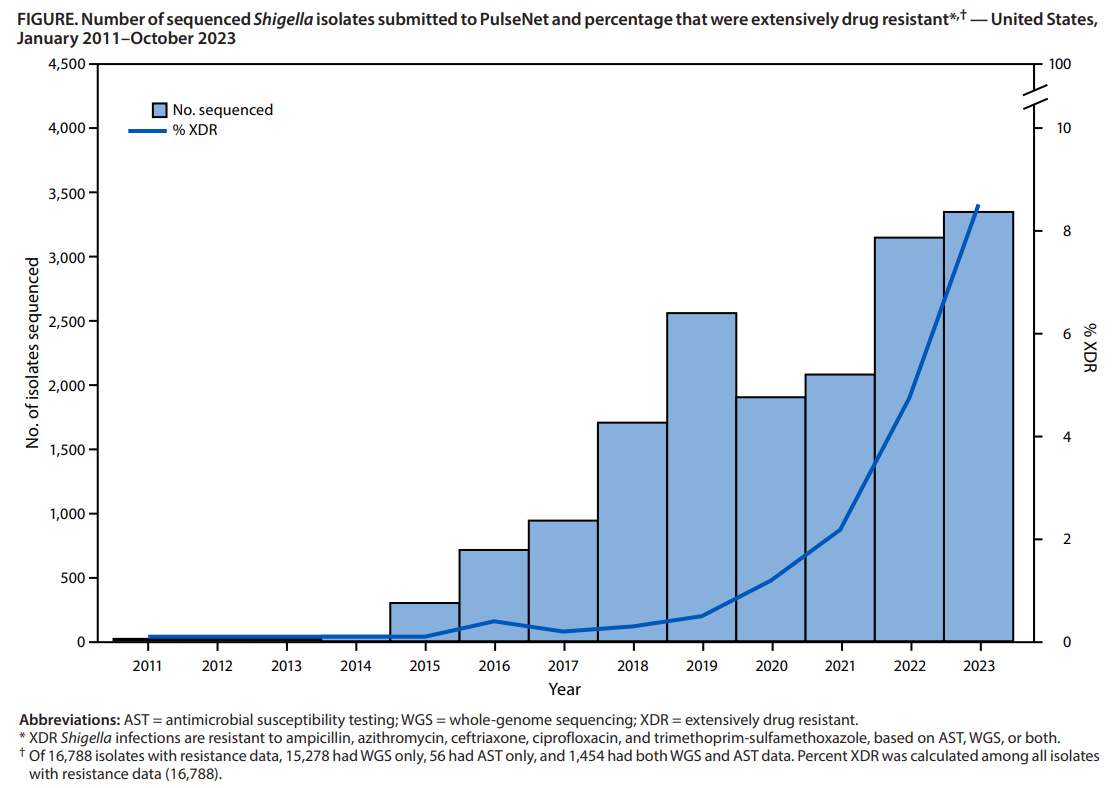
Logan N, Birhane MG, McDonald SL, et al. MMWR Morb Mortal Wkly Rep 2026;75:173–178. Open Access! Emergence of Extensively Drug-Resistant Shigellosis — United States, 2011–2023. DOI: http://dx.doi.org/10.15585/mmwr.mm7513a1
Background: “Shigellosis is a nationally notifiable diarrheal illness caused by gram-negative bacteria. Shigella infection is spread through fecal-oral transmission (infection can occur with as few as 10 organisms) and sexual contact. Although most infections are self-limited, antibiotics are indicated for severe illness or to reduce transmission in settings with high risk for spread. Since 2015, a growing proportion of cases has been caused by extensively drug-resistant (XDR) Shigella species, defined as being resistant to ampicillin, azithromycin, ceftriaxone, ciprofloxacin, and trimethoprim-sulfamethoxazole. No Food and Drug Administration–approved oral antimicrobial agents are available to treat these XDR infections.”
Key finding:
The percentage of Shigella isolates with resistance data that were XDR increased from 0% during 2011–2015 to 8.5% in 2023
Limitations included the following:
“Surveillance likely underestimated XDR Shigella isolate incidence: not all isolates were sequenced or had AST, many specimens that were positive by culture-independent diagnostic tests were not cultured, underdiagnosis and incomplete reporting occurred>”
My take (borrowed from authors): “It is concerning that resistance is increasing.”XDR Shigella infection is an emerging concern in the United States. Because no oral antimicrobial agents are FDA approved, prevention, early detection, AST-guided therapy, and timely reporting are important to protect populations at higher risk for XDR Shigella infection”
This genome-wide association study (GWAS) confirms the idiopathic achalasia (IA) “association of variants in HLA-DQB1 and HLA-DQA1, but also points to a more complex genetic risk architecture at this locus that involves an IA risk variant in HLA-DRB1. Moreover, the GWAS resulted in the identification of three novel disease variants outside HLA. One leads to an amino acid substitution with functional effect in PTPN22. One further novel IA risk variant leads to a downregulated expression of TNFSF8, TNFSF15 and TNC in immune-relevant cells. The remaining disease variant is located near ZNF365, but the cellular pathogenic mechanism remains unknown.”
“On the polygenic level, this study provides the first IA heritability estimate and shows that immune-mediated mechanisms that are shared with Crohn’s disease (CD) contribute to IA aetiopathology.”
My take: This study “highlights that immune-mediated mechanisms influenced by genetic risk are of major relevance for disease development.”
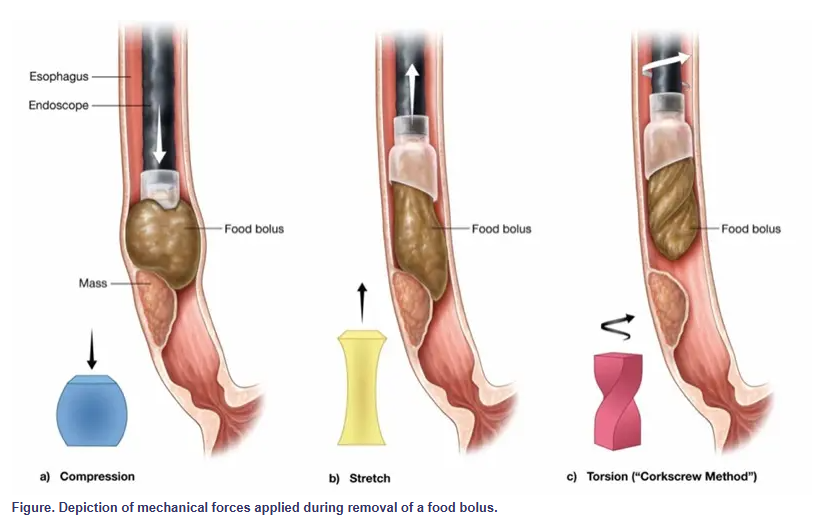
Yet, just as one wouldn’t simply yank a cork from a bottle, it may be time to rethink how we approach food bolus removal. Torsional stress—twisting rather than pulling—may provide a more efficient and atraumatic method for managing these impactions, a technique we refer to as the “corkscrew method.”
Less force is required because rotation gradually disengages the bolus, decreasing the need for strong pulling or pushing. This method also poses a lower risk for mucosal injury. Shear forces are distributed rather than focused, reducing trauma.
My take: This is probably worth a try for the next food impaction requiring endoscopic removal.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
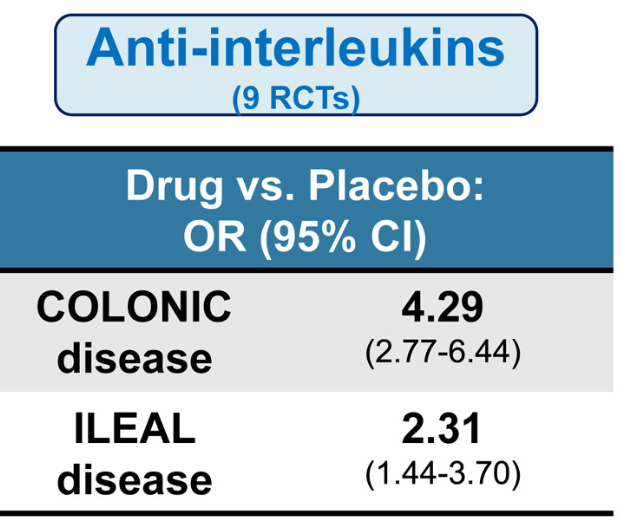
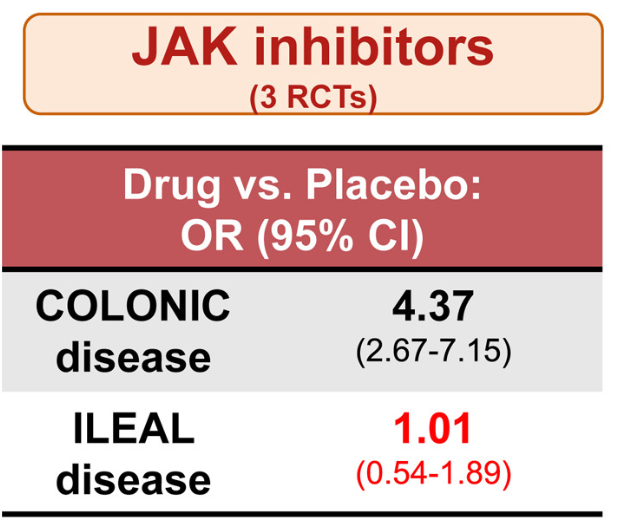
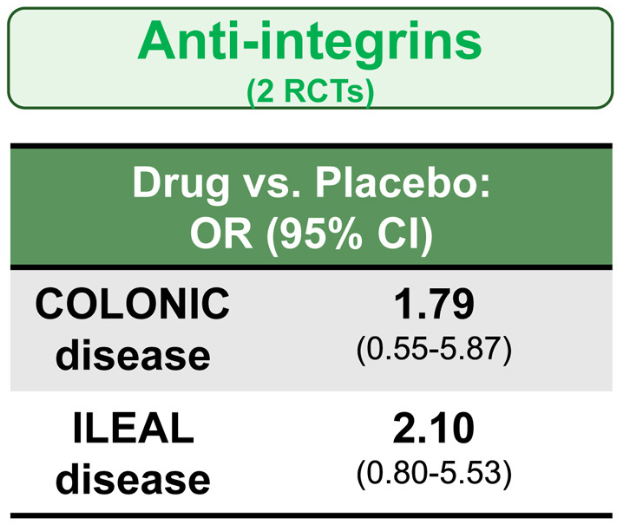
Methods: In the study by Lee et al, the authors identified 14 randomized controlled trials in 3139 patients with moderate-to-severe CD who were treated with different advanced therapies vs placebo, and reported efficacy in inducing clinical remission, stratified by disease location (isolated colonic vs ileal disease, excluding ileocolonic disease). The authors did not identify any RCT of TNF antagonists that reported induction of remission by disease location.
Key findings:
All advanced therapies had better success with colonic disease rather than ileal disease
Anti-interleukins (eg. IL23 o rIL12/IL23 agents) worked best for ileal disease among these advanced therapies
JAK inhibitors did not work well for ileal disease, but performed well for colonic disease
Anti-integrins, like vedolizumab, had some efficacy for ileal disease but generally a lower clinical remission rate than other agents
Lmitations included the use of clinical remission as the primary outcome
While this study did not provide data on anti-TNF therapy, in the discussion the authors note that “TNF antagonists may have advantages in small bowel CD…infliximab demonstrated the highest rate of improvement in large ileal ulcers (>0.5 cm).” [ref#45] “Additionally, infliximab has been reported to reduce fibrostenosis-associated inflammation, [Ref#46] making it currently the most suitable therapeuctic option for small bowel CD.”
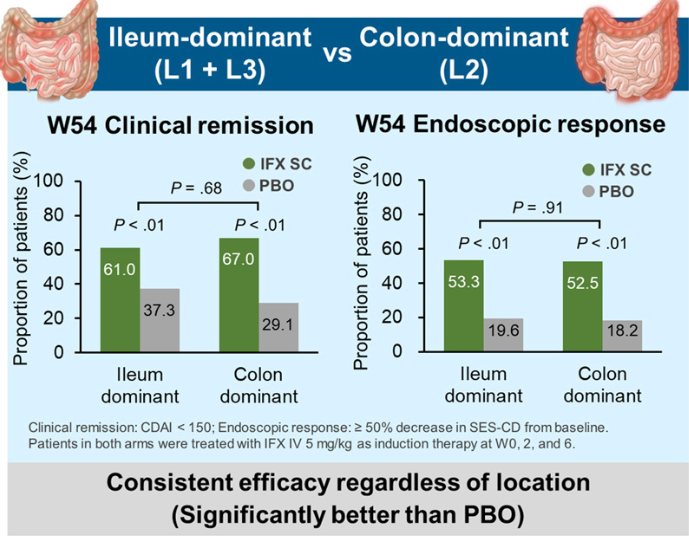
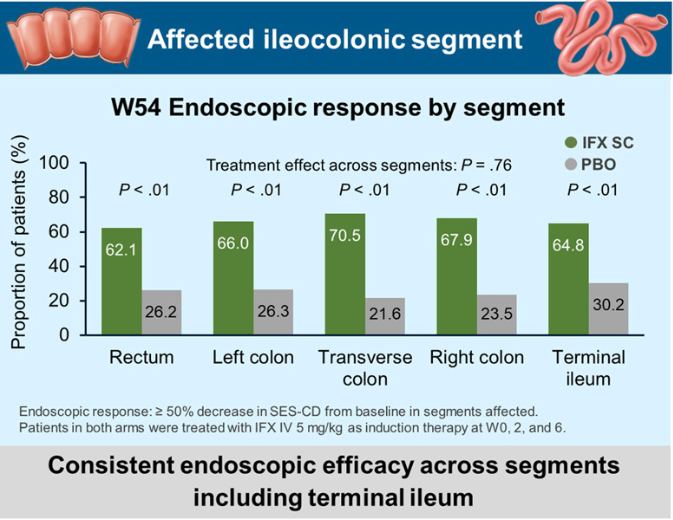
In the study by Sands et al, this post-hoc analysis included week 10 responders (n=329) to intravenous IFX induction therapy who were randomized to receive IFX SC 120 mg every 2 weeks or placebo (PBO) during maintenance therapy.
Key findings:
My take: These two studies indicate that anti-TNF agents (particularly infliximab) and IL-23 type agents are most effective for Crohn’s disease affecting the ileum. JAK inhibitors are best for colonic disease.
In the first article by Jaafari et al, the authors identified four predominant food cluster patterns from 54,127 participants from 26 countries who completed online questionnaires. The highest prevalence of IBS was associated with cluster A (including Egypt, Brazil, and Colombia) and the lowest with cluster D from several Asian countries. Cluster A dietary pattern was “rich in FODMAPs.” Cluster D participants reported the highest frequencies of fish, rice and tofu consumption and lowest milk consumption (which could be due to higher rates of lactose intolerance). The limitations from this study include the reliance on a questionnaire, the small number of foods surveyed (10), and cultural differences in reporting symptoms.
The study by Mikhael-Moussa et al examined carbohydrate malabsorption, based on breath testing, in patients diagnosed with disorders of gut-brain interaction (DGBI). Patients completed questionnaires as well.
Key findings:
Among the 301 patients with DGBI included in our analysis, 178 (59.1%) had carbohydrate intolerance
Carbohydrate-intolerant patients were significantly more likely to be female (P value < 0.001), to have 2 or more DGBI (P value = 0.001) to have lactose maldigestion (P value< 0.001) and fructose malabsorption (P value = 0.023), higher irritable bowel syndrome and somatic symptom severity, and lower quality of life (P value < 0.001) compared with patients without carbohydrate intolerance
Discussion:
There are multiple potential reasons why certain foods can contribute to GI symptoms including malabsorption, gastrointestinal mobility, alterations in intestinal microbiota, intestinal distention, fluid accumulation, and localized IgE-dependent reactions (noted with confocal laser endomicroscopy).
“Carbohydrate-reduced diets have been found effective in reducing symptoms in patients, regardless of the presence of maldigestion/malabsorption”
My take: Dietary triggers are important for the majority of patients with IBS. In this study, patients with documented carbohydrate malabsorption had increased severity of their symptoms.
Methods: This retrospective cohort study used an administrative claims database and identified patients with IBD who were new users of either JAK inhibitors (n=856) or TNF antagonists (n=9422) between 2016 and 2023. Mean age was 45 years.
Key findings:
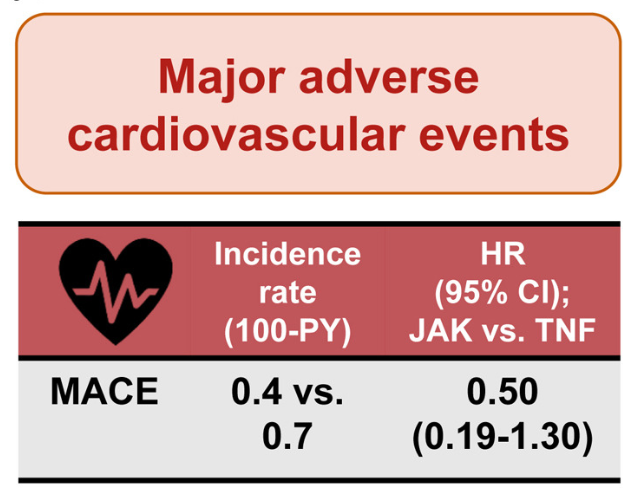
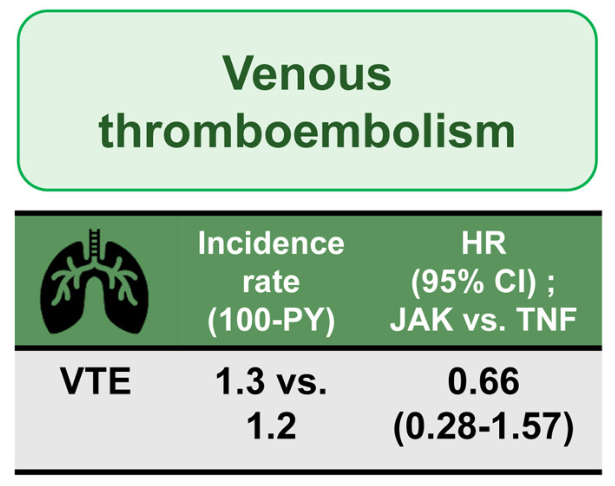
There was no difference in the risk of VTE (1.3 vs 1.2; HR, 0.66; 95% CI, 0.28–1.57) and MACE (0.4 vs 0.7; HR, 0.50; 95% CI, 0.19–1.30)
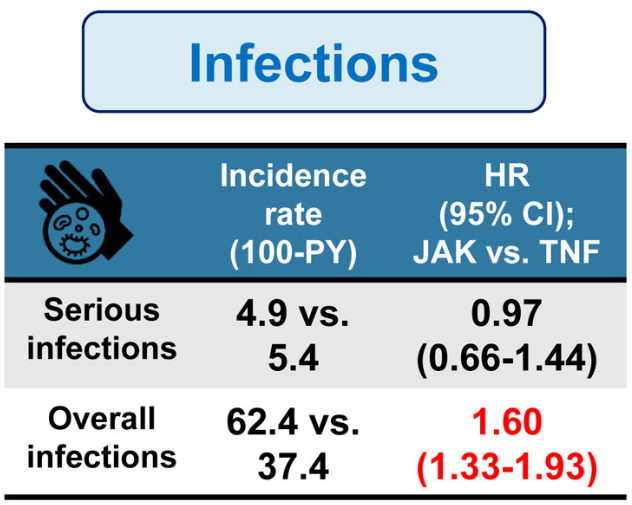
There was no difference in the risk of serious infections (4.9 vs 5.4; HR, 0.97); however, JAK inhibitors were associated with an increase risk of overall infections (incidence rate, 62.4 per 100 person-years [PY] vs 37.4 per 100 PY; hazard ratio [HR], 1.60)
The authors note that their findings differ from the ORAL study (Ytterberg et al. NEJM 2022; 386: 316-326.) which showed higher risk of MACE in patients receiving tofacitinib. In the current study, even in patients deemed to be at higher risk for MACE (age >50 years with at least 1 cardiovascular risk factor), JAK inhibitors were associated with lower incidence and risk of MACE compared with TNF antagonists (IR per 1000 PY, 0.4 vs 2.1, HR 0.10).
My take (borrowed from the authors) “It is unlikely that JAK inhibitors are associated with higher risk of VTE and MACE compared with TNF antagonists in most patients with IBD.”
Methods: This was a prospective cohort study of patients (n=181 — 79 CD, 83 UC, 6 -IBD-U, 13 with IPAA) treated with UPA between April 2022 and November 2023. Included patients responded to UPA induction, had loss of response (LOR) after dose reduction, and subsequently received reinduction therapy with 45 mg QD. They were followed for a median duration 93 weeks.
Key findings:
Dose escalation to 45 mg QD for a median of 13 weeks (IQR, 8–36 weeks) recaptured clinical response in 80.4%
Among patients who recaptured response, 19 again reduced dose
93.8% of patients on 45 mg QD maintained remission vs 21.1% who again dropped to 30 mg QD (P < .001)
Acne/rosacea was the most common adverse event (39%); there were no serious adverse events
In their discussion, the authors note that dose escalation with another JAK inhibitor, tofacitinib, also has been shown to reverse LOR (in about 50%). In addition, they note that “in our experience, prolonged exposure to 45 mg QDD UPA is safe.” Though, “a longer follow-up period…is required to address long-term safety of UPA in IBD, especially at a higher dose.”
My take: Many patients taking UPA have not responded to multiple other advanced therapy. As such, the potential to recapture response with a higher dose of UPA is an important finding. Dose intensification is an effective strategy for most of the advanced therapies.
Briefly noted: S Honap et al.Clin Gastroenterol Hepatol 2026; 24: 784-793. Open Access! Comparative Effectiveness of Tofacitinib vs Upadacitinib for the Treatment of Acute Severe Ulcerative Colitis In this retrospective study of 111 adults with ASUC, Between days 3 and 7 after treatment initiation, upadacitinib was associated with greater response rates (84% vs 54%), but response/remission was comparable at day 98 (45%/36% vs 55%/48%) and day 182 (29/29% vs 39/34%).