Listed below are the 10 ‘Best Practice Advice’ recommendations. I think the acknowledgement that “hemostatic powder should be preferentially used as a rescue therapy and not for primary hemostasis, except in cases of malignant bleeding or massive bleeding with inability to perform thermal therapy or hemoclip placement” (#7) is very useful.
“Best Practice Advice:”
Endoscopic therapy should achieve hemostasis in the majority of patients with NVUGIB.
This may include clips, thermal (heater probes, bipolar/multipolar catheters, hemostatic forceps), diluted epinephrine injection, and hemostatic spray
Initial management of the patient with NVUGIB should focus on resuscitation, triage, and preparation for upper endoscopy. After stabilization, patients with NVUGIB should undergo endoscopy with endoscopic treatment of sites with active bleeding or high-risk stigmata for rebleeding.
Endoscopists should be familiar with the indications, efficacy, and limitations of currently available tools and techniques for endoscopic hemostasis, and be comfortable applying conventional thermal therapy and placing hemoclips.
Monopolar hemostatic forceps with low-voltage coagulation can be an effective alternative to other mechanical and thermal treatments for NVUGIB, particularly for ulcers in difficult locations or those with a rigid and fibrotic base.
Hemostasis using an over-the-scope clip should be considered in select patients with NVUGIB, in whom conventional electrosurgical coagulation and hemostatic clips are unsuccessful or predicted to be ineffective.
Hemostatic powders are a noncontact endoscopic option that may be considered in cases of massive bleeding with poor visualization, for salvage therapy, and for diffuse bleeding from malignancy.
Hemostatic powder should be preferentially used as a rescue therapy and not for primary hemostasis, except in cases of malignant bleeding or massive bleeding with inability to perform thermal therapy or hemoclip placement.
Endoscopists should understand the risk of bleeding from therapeutic endoscopic interventions (eg, endoluminal resection and endoscopic sphincterotomy) and be familiar with the endoscopic tools and techniques to treat intraprocedural bleeding and minimize the risk of delayed bleeding.
In patients with endoscopically refractory NVUGIB, the etiology of bleeding (peptic ulcer disease, unknown source, post surgical); patient factors (hemodynamic instability, coagulopathy, multi-organ failure, surgical history); risk of rebleeding; and potential adverse events should be taken into consideration when deciding on a case-by-case basis between transcatheter arterial embolization and surgery.
Prophylactic transcatheter arterial embolization of high-risk ulcers after successful endoscopic therapy is not encouraged.
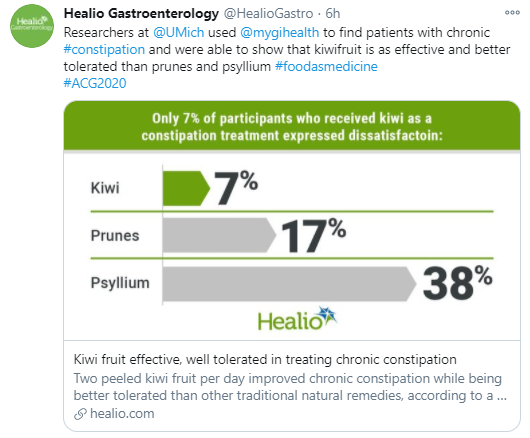
From a randomized (Virtual) ACG 2020 study from Samuel W. Chey and colleagues (University of Michigan), n=79 adults:
“All three treatments improved complete spontaneous bowel movement (P .003). Prunes demonstrated the largest magnitude of response at 67% vs. 64% for psyllium vs. 45% for Kiwi fruit”
“The highest proportion of participants – 68% – reported treatment satisfaction with kiwifruit while similar proportions of those receiving prunes and psyllium – 48% – reported satisfaction”
“The kiwi group had the lowest proportion of participants reporting treatment dissatisfaction at 7%….Participants receiving prunes and psyllium were more likely to report abdominal pain and bloating than those receiving kiwi”
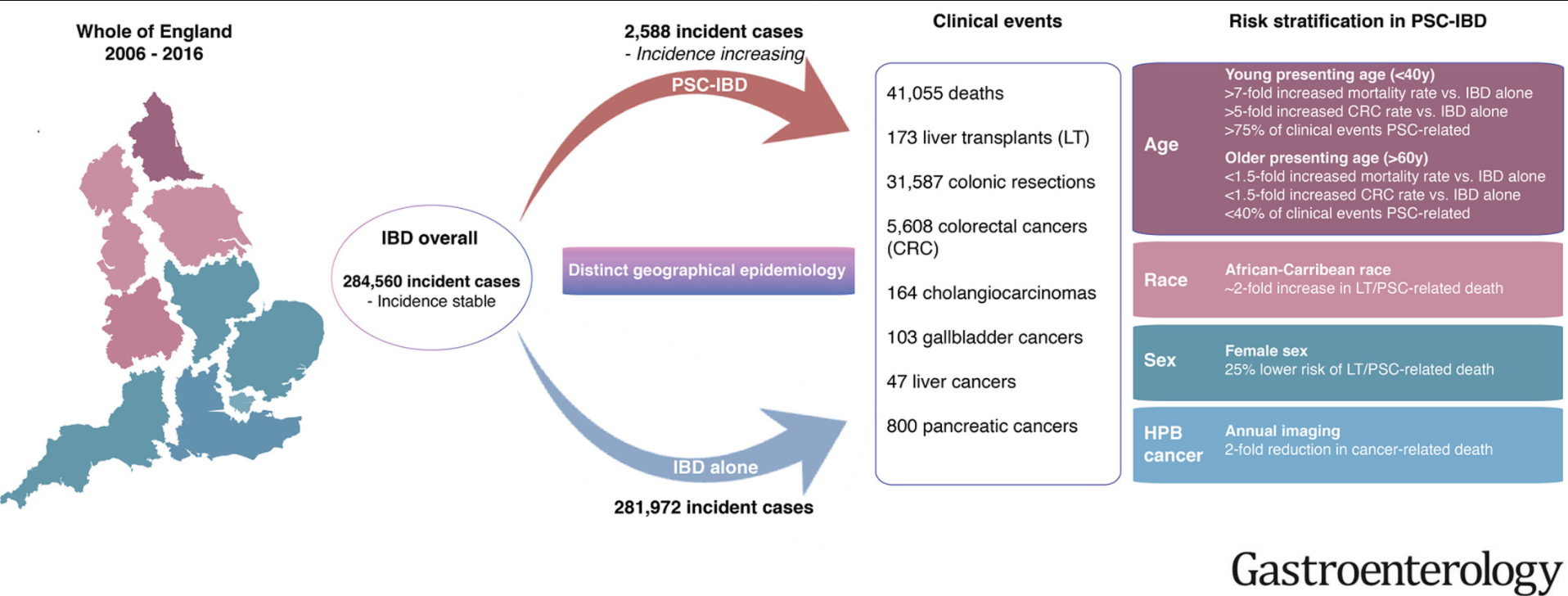
Methods: The authors linked prospectively collected data from national health care registries maintained for all adults in England on hospital attendances, imaging and endoscopic evaluations, surgical procedures, cancer, and deaths.
Key findings:
Over 10 years, we identified 284,560 incident cases of IBD nationwide; of these, 2588 patients developed PSC. This study excluded patients <18 years of age.
Development of PSC was associated with increased risk of death and CRC (hazard ratios [HRs], 3.20 and 2.43, respectively; P < .001) and a lower median age at CRC diagnosis (59 y vs 69 y without PSC; P < .001)
Compared to patients with IBD alone, patients with PSC-IBD had a 4-fold higher risk of CRC if they received a diagnosis of IBD at an age younger than 40 years
Development of PSC also increased risks of cholangiocarcinoma (HR, 28.46), hepatocellular carcinoma (HR, 21.00), pancreatic cancer (HR, 5.26), and gallbladder cancer (HR, 9.19) ( P < .001 for all)
The greatest difference in mortality between the PSC-IBD alone group vs the IBD alone group was for patients younger than 40 years
Patients with PSC-UC had >40% risk of colonic resection compared to patients with IBD alone (aHR 1.65)
My take: This study shows the impact the added diagnosis of PSC has for patients with IBD. One of the limitations in assessing outcomes is determining whether someone with IBD has PSC as there are a lot of patients with IBD who have asymptomatic changes in their biliary tree.
In an analysis (n= 279 adults, 70% female, average age 47 years) of patients with chronic constipation at a tertiary center who were referred for anorectal manometry, 19% had symptoms consistent with an eating disorder; this assessment was based on the Eating Attitudes Test (EAT-26).
“Gastrointestinal-specific anxiety fully mediated the relationship between the severity of ED pathology and constipation (standardized β, 0.11–0.16; P = .026–.024).”
The authors note that screening for eating disorders “is of particular importance before prescribing dietary interventions.”
My take: While this was a study with adults, it is likely that chronic constipation may be a presenting feature of an eating disorder in teenagers as well.
This prospective study combined 3-dimensional high-resolution manometry (3D-HRM) with detailed analysis of computed tomography images to study the EGJ (esophagogastric junction) in patients with achalasia (n=12) and healthy controls (n=10). Key finding: Besides LES, the 3D pressure profile of the EGJ can indicate anatomic and functional abnormalities of the crural diaphragm muscle in patients with achalasia esophagus
“In this edition of Gastroenterology, researchers led by Ravi Mittal …demonstrated an asymmetric, extrinsic CD (crural diaphragm) component to EGJ pressure superimposed on the intrinsic LES.”
Methods: “This case-time-control study used data from the French national health insurance database, covering 66 million individuals, on all patients exposed to ustekinumab between April 1, 2010, and December 31, 2016, classified according to their cardiovascular risk level (high- and low-risk strata). The risk period was the 6 months before the SCE, defined as acute coronary syndrome or stroke, and the reference period was the 6 months before the risk period. Statistical analysis was performed from September 20, 2017, to July 6, 2018.”
Key findings:
Of the 9290 patients exposed to ustekinumab (4847 men [52%]; mean [SD] age, 43 [14] years), 179 experienced SCEs (65 cases of acute coronary syndrome, 68 cases of unstable angina, and 46 cases of stroke).
Among patients with a high cardiovascular risk, a statisically significant association between initiaton of ustekinumab treatment and SCE occurrence was identified (odds ratio, 4.17; 95% CI, 1.19-14.59).
Conversely, no statistically significant association was found among patients with a low cardiovascular risk (odds ratio, 0.30; 95% CI, 0.03-3.13).
My take: This study suggests that the initiation of ustekinumab treatment may trigger SCEs among patients at high cardiovascular risk; however, the study conclusions are limited as this was an observational study (not a randomized trial).
This is a useful article in evaluation of elevated ferritin levels in adults. This approach is NOT applicable in young children but may have some use in adolescents. In young children, other considerations include HLH and macrophage activation. In newborns, elevation of ferritin (along with liver dysfunction) may be indicative of GALD (gestational alloimmune liver disease).
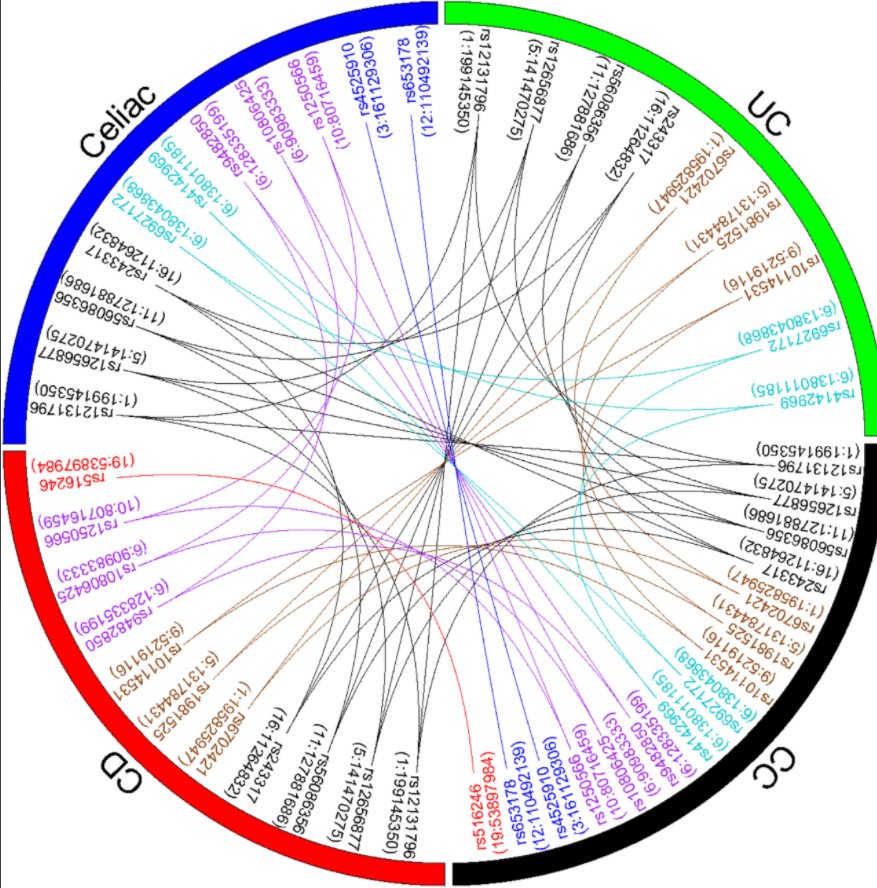
“In this largest genetic study of CC to date with histologically confirmed diagnosis, we strongly implicated the HLA locus and proposed potential non-HLA mechanisms in disease pathogenesis. We also detected a shared genetic risk between CC, celiac disease, CD, and UC.”
Selecting Patients for Surgery: Current guidelines fall short in determining appropriate patients who would benefit most from surgery. For instance, the recommendation that a desire to discontinue PPI therapy is a suitable indication for antireflux surgery fails to recognize that 62% of patients end up back on PPIs within 9 years.Furthermore, indicating that those patients who failed medical management would benefit from surgery neglects the fact that the patients who respond best to antireflux surgery are those who have responded well to PPI therapy in the first place
Complications: Late postoperative complaints are more common and often are referred back to the referring gastroenterologist for diagnosis and management. These include late-onset dysphagia (3%–24%), recurrent heartburn (up to 62%), gas-bloat syndrome (up to 85%), and diarrhea (18%–33%). Anatomic failure of the fundoplication (Figure Below) can present a unique challenge to the clinician because the symptoms and patient presentation (postoperative dysphagia, regurgitation, and heartburn) can be clinically indistinct from the issues seen commonly after this surgery even in the best of circumstances. Therefore, the gastroenterologist should assess symptoms carefully in a stepwise approach with upper endoscopy, barium swallow, esophageal manometry, and/or ambulatory pH monitoring when appropriate and plan any interventions based on objective findings from focused testing.
Other points:
Antireflux Surgery Has No Significant Impact on the Progression of Barrett’s Esophagus to Esophageal Adenocarcinoma: Endoscopic Ablation of Dysplastic Barrett’s Esophagus Still Is Recommended
Medical Therapy Is More Cost Effective Than Surgical Treatment if the Cost of the Drug Is Low
Several New, Less-Invasive Surgical and Endoscopic Antireflux Procedures Are Now Food and Drug Administration Approved, Available, and Appear Promising