Followup on previous blog post (Mary Suhr: Coding Update 2025) -there is a new CPT code for the PENFS procedure in 2026: 64567. This procedure has FDA approval for children/adolescents (8-21 years) with functional abdominal pain associated with irritable bowel syndrome; in addition, it has an indication for functional dyspepsia.
While it may seem like a disease from the past, this airborne illness kills more people than any other infectious disease worldwide, roughly 1.2 million a year. That number could increase dramatically because of the Trump administration’s cuts to foreign assistance, according to a new study…
As many as 10 million additional people could get TB, and 2.2 million could die by 2030 in high-burden countries under the worst-case funding scenario over the next five years, researchers report in the journal PLOS Global Public Health.
My take: I recently finished, Everything is Tuberculosis by John Green, which is a good read. So this article caught my attention. Even before the funding cuts, more effort was needed to stop the scourge of TB. Currently TB kills more than a million people per year; in some historic periods, it has killed as many as one in seven people.
Thanks to Anna Kelly for recommending the book to me.
This article recommends that physicians consider a proactive role in explaining the prior authorization process. Here is his suggested handout:
We want to make sure you understand something called “prior authorization.”
Often, insurance companies require us to ask their permission for coverage before prescribing a drug or doing a test or procedure. They say they do this to make sure that we are suggesting medically appropriate, cost-effective care — on behalf of you or your employer. In fact, this is always our goal, but they don’t always think we’re accomplishing it.
To try to get this authorization ahead of time, we document our logic in the format they require, and they may reject it. Often we find out about rejections well before any surgery, but sometimes we don’t.
The doctors here often don’t understand why insurers reject our requests for permission.
The prior authorization process can be as baffling to us as it may be to you, and we find it intensely frustrating. Please keep in mind that we are at the mercy of dozens of insurance companies, and their rules and requirements can change constantly. Your doctor may not be able to predict the odds of a prior authorization rejection, and musing over the possibility before it happens probably isn’t a productive use of our time together in the exam room.
We do have billing specialists who handle prior authorization requests for our doctors.
If you have any concerns once you know what we’re recommending, reach out to our billing specialist or the department that helps with this. They too may not be able to tell you much ahead of time, but they will play a role in helping us with any appeal that is necessary if our request for prior authorization fails in full or in part.
Watch for all communications — from us but especially from your insurance company.
Insurance companies like paper mail. Check yours every day, in case they issue denials that way. Download your insurance company’s app and sign up for push notifications for any changes, especially if they offer alerts specifically for changes in prior authorization. Opt in to email notifications, and check your spam.
You might hear from the insurance company before we do.
We are partners here, and you have a role.
We think we are pretty good at navigating this deeplysuboptimal system, but we can’t do it without you. Please, become intimately familiar with your insurance plan and what it covers — whether prior authorization is required or not.
Engage a human resources specialist at your employer, if you have one, to help communicate with the insurance company during the prior authorization process if you think you might need help. Call the insurer on your own to ask whether your medicine or procedures require permission and whether the insurance company is missing information it needs.
Patients can sometimes get better information faster than we can, if only because we may be trying to help hundreds of patients at once.
What happens if our prior authorization request is rejected?
There is an appeal process, which may differ by insurer. Contact a billing specialist with whatever information you have from your insurance company, though we may hear about it before you do and start the process on our own.
Sometimes, the problem is a relatively simple one, resulting from confusion over the byzantine process of submitting medical codes, or some similar snafu. But often, a doctor will have to do what’s known as a peer review with someone from the insurance company. We find this burdensome, since the “peer” on the line with us may not have the same level of expertise as we do. That prolongs the call, adds to our overall operating expenses and keeps us from spending more time with you, the patient.
We’ll give any appeal our best shot, but it may take time to schedule any peer review.
Please don’t worry.
We dislike having to give you a document like this that might produce anxiety. Still, it’s better that you be aware of how things might go than be desperately trying to reach us or learn about the prior authorization process after getting a mysterious and indecipherable rejection letter in the mail.
If things don’t go our way at first, we will have your back and argue fiercely to get you coverage for the care you need.
Still, there is only so much we can do to make this easier.
Our industry has a structural problem. We can provide you information and over-communicate, but the incentive systems are what they are.
Insurance companies may sometimes deny permission for care in order to make more money. Employers (and individuals) don’t want premiums to rise. Some patients demand that we throw everything we doctors have at every health condition. Regulators are in the middle of all of it, ordering up paperwork. And doctors are not infallible.
We wish we could fix all of that. But for now, we can be plain-spoken with you about how prior authorization works and try to make the system that we have just a bit more tolerable.
I am not an expert on autism. However, I am concerned about the administration’s recent recommendations regarding acetaminophen and autism. Even scientists who have suggested a possible link have NOT recommended stopping the use of acetaminophen during pregnancy.
It is well-recognized that autism is related to multiple factors, both genetic and potential environmental factors. The use of acetaminophen, even if linked to autism, could represent an epiphenomenon in which a primary disorder (like a fever or infection) is responsible for subsequent neurodevelopmental problems rather than the medicine itself. While there has been growing concern about the increasing frequency of autism, much of this relates to changes in the definition of autism over various periods.
I recommend the following recent sources of information on this topic:
Editorial Board Wall Street Journal, 9/23/25: Trump, Tylenol and the Plaintiffs Bar “The acetaminophen link to autism is based on weak evidence pushed by RFK Jr. and his legal allies.”
“Today’s announcement by HHS is not backed by the full body of scientific evidence and dangerously simplifies the many and complex causes of neurologic challenges in children. It is highly unsettling that our federal health agencies are willing to make an announcement that will affect the health and well-being of millions of people without the backing of reliable data.
“In more than two decades of research on the use of acetaminophen in pregnancy, not a single reputable study has successfully concluded that the use of acetaminophen in any trimester of pregnancy causes neurodevelopmental disorders in children. In fact, the two highest-quality studies on this subject—one of which was published in JAMA last year—found no significant associations between use of acetaminophen during pregnancy and children’s risk of autism, ADHD, or intellectual disability.
“Acetaminophen is one of the few options available to pregnant patients to treat pain and fever, which can be harmful to pregnant people when left untreated. Maternal fever, headaches as an early sign of preeclampsia, and pain are all managed with the therapeutic use of acetaminophen, making acetaminophen essential to the people who need it. The conditions people use acetaminophen to treat during pregnancy are far more dangerous than any theoretical risks and can create severe morbidity and mortality for the pregnant person and the fetus.”
From KFF News:
In August, Bauer and her colleagues published an analysis of 46 previous studies on Tylenol, autism, and attention-deficit/hyperactivity disorder. Many found no link between the drug and the conditions, while some suggested Tylenol might occasionally exacerbate other potential causes of autism, such as genetics.
Bauer, an epidemiologist at the University of Massachusetts-Lowell, and her team called for more judicious use of the drug until the science is settled.
Autism experts at the Centers for Disease Control and Prevention were neither consulted for the White House’s long-awaited autism announcement nor asked to review a draft of the findings and recommendations…
If prenatal Tylenol has any association, which it may not, it would help account for only a fraction of cases, she said. Further, research has not deeply examined Tylenol risks in young children, and manyrigorous studies refute a link between vaccines and autism.
Bauer worries such statements will cut both ways: People may put themselves at risk to avoid vaccines and Tylenol, the only safe painkiller for use during pregnancy. And she frets that scientists might outright reject her team’s measured concerns about Tylenol in a backlash against misleading remarks from Trump and other members of his “Make America Healthy Again” movement….
Helen Tager-Flusberg, director of the Center for Autism Research Excellence at Boston University, called Trump’s comments dangerous. Fevers can harm the mother and the developing fetus, she said, adding that fevers are more strongly associated with autism than Tylenol…
Several medical and scientificassociations have called for Kennedy’s removal or resignation. Many scientists are skeptical of what he says because much of it has been misleading or wrong. For example, he’s said HIV isn’t the only cause of AIDS (it is), that antidepressant drugs cause mass shootings (they don’t), that older adults don’t have severe autism (some do), that the measles vaccine causes brain swelling (it doesn’t), that covid vaccines were the deadliest vaccines ever made (they aren’t), that vaccines aren’t safety-tested (they are), and that vaccines contribute to autism (they don’t).
From the Wall Street Journal:
Washington Post Editorial:
From TIME article: “Despite what we are now hearing from the most powerful health offices in the nation, the science on acetaminophen and autism remains unsettled. What is not unsettled is the damage done when politics masquerades as medicine. Every false certainty erodes the trust that holds the fragile bridge between patients and their doctors. Break that trust, and no study, no drug, no vaccine will be enough to save lives when the next real crisis comes. When politicians play doctor, it’s families who will pay the price.”
My take: Thinking about the damage from this press conference, I was reminded of a scene from the movie “Doubt.” In the movie Doubt, Father Flynn (played by Philip Seymour Hoffman) tells a parable about an old priest instructing a woman who has been gossiping to take a pillow, cut it open on her roof, and then return to gather up all the feathers. When she tells him it can’t be done because “the wind took them all over,” the priest responds: “And that… is gossip!”
The spreading of damaging rumors and lies, which is being done by leaders of this country, is impossible to contain or undo once released, and its impact is far-reaching and destructive.
This commentary was published on 7/30/25 and was written by the 17 voting members of the ACIP who were dismissed.
Key points:
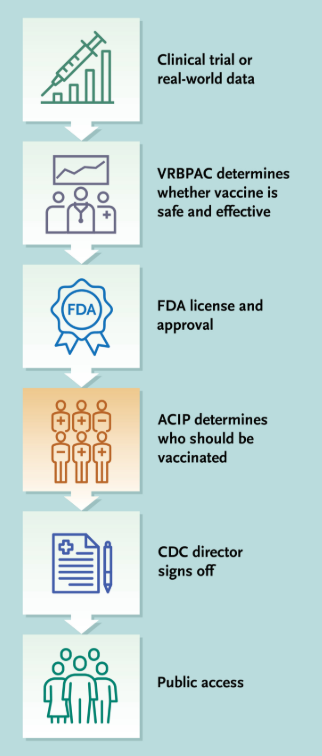
For over 60 years, the Advisory Committee on Immunization Practices (ACIP), which comprised a diverse group of nonpartisan specialists, has advised the Centers for Disease Control and Prevention (CDC) on vaccine recommendations based on science and intensive review of evidence. The abrupt dismantling of the rigorously vetted process and the replacement of the Committee with an inexperienced and biased panel has engendered fundamental distrust in the Committee’s vital work…The government has abruptly changed vaccine policy through social media postings and publications in news media.
**VRBPAC denotes FDA’s Vaccines and Related Biological Products Advisory Committee
The ACIP has been an independent committee of vaccine scientists and clinicians that has relied on a process called the Evidence to Recommendations framework. This deliberative framework calls for a review of the strength of evidence around a variety of factors, including the magnitude of the public health problem, potential benefits and harms, values, acceptability, resource use, equity, and feasibility.
Previously, the ACIP had well-defined and stringent conflict of interest standards. Voting members had to disclose and actively manage any actual or apparent conflicts of interest before and throughout their tenure… ACIP members disclosed any potential conflicts during each vote and could not vote on issues where they had an ongoing conflict.
ACIP recommendations have many implications. For example, government-run medical systems such as the Veterans Health Administration may be able to provide only vaccines consistent with ACIP recommendations…For children who are uninsured, underinsured, Medicaid-eligible, American Indian, or Alaska Native, the Vaccines for Children program pays only for ACIP-recommended vaccines; about half of children in the United States get their vaccines through this program.
The nation now faces a scenario in which the rigor and discipline of these vaccine recommendation processes are rapidly eroding…Three major issues are of particular concern: the quality and availability of data; straightforward guidance for providers and the public; and insurance coverage and vaccine access, uptake, and equity.
The absence of a cohesive federal policy produced by means of an evidence-based, expert-informed process creates the very real potential for conflicting messaging from within the Department of Health and Human Services (DHHS) or in relation to messages from nongovernmental agencies, such as professional organizations. This lack of coordination is likely to cause confusion for providers and the public, vaccine-administration errors, decreased uptake of vaccines, and further erosion of an already damaged public trust. It is also likely that in this milieu, misinformation will flourish.
The ACIP cannot be replaced, but it may be possible to limit the damage. In this vacuum, it is urgent that other organizations step forward to reassert an evidence-based, expert approach to vaccine recommendations to bring the nation back from the precipice of uncontrolled spread of infectious diseases and needless deaths.
My take: The advice from governmental agencies has been compromised. With regard to vaccines, instead of a transparent process with expertise, we are left with partisan recommendations with questionable credibility.
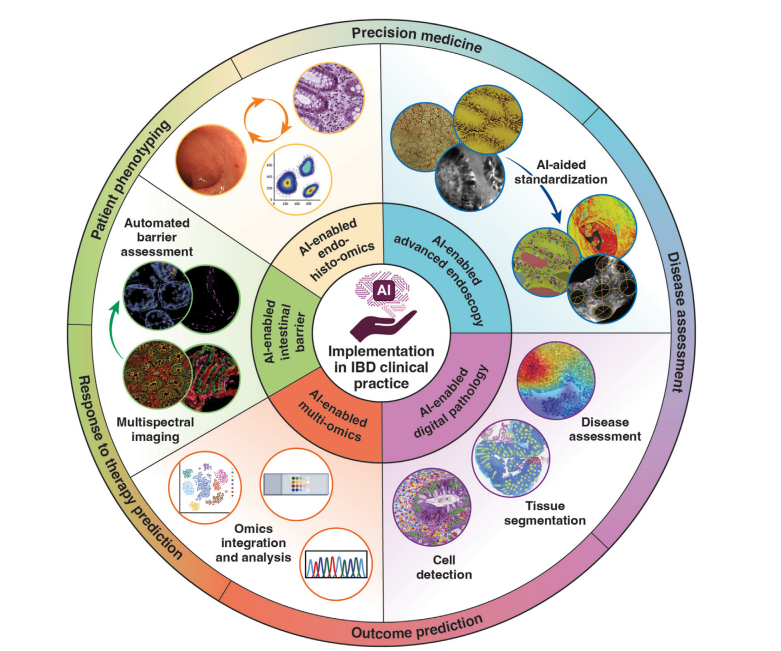
This month’s Gastroenterology issue is devoted solely to the use/expected uses as well as risks of artificial intelligence (AI) for gastroenterology and hepatology.
“AI is reshaping the landscape of gastroenterology and hepatology with the promise of better, faster, more objective, and standardized care of delivery. However, behind the algorithms lies a more insidious risk: the erosion of trust in human providers…Information risk …include both error commission (ie, when the models generate false statements, introduce nonsensical concepts, or fabricate sources) and error omission (ie, summaries that omit critical information)…
When AI becomes the center of care, patients may perceive their doctors as intermediaries…diminishing the therapeutic effect of the patient-physician relationship…This arrangement can dilute clinical training, increase physician burnout, and lead to medicolegal implications…Other risks include perpetuating bias from nonrepresentative training data and amplifying uncertainty of AI due to lack of real-world validation…
We hope that AI systems will allow us to spend more, not less, time with patients and empower us to provide personalized care by leveraging high-quality multimodal data.”
Most of the articles are behind a paywall in this issue. There are five that are open access articles:
My take: These articles provide a good deal of information about the applications and risks of AI. In my view, physicians will be needed more than ever to help interpret/manage the huge amount of information available.
Despite the enormous benefits of hepatitis B vaccination, it appears that this administration has its sights on changing the policy of administration at birth.
Committee members, some of whom are vaccine skeptics, are likely to recommend restricting the use of the shots at birth or delaying them until later in childhood…
“Unless the mother is hepatitis-B-positive, an argument could be made to delay the vaccine for this infection,” Martin Kulldorff, the committee’s chair, said at its previous meeting in June.
Vaccine experts at the C.D.C., who normally would be deeply involved in preparing for this week’s meeting, have been sidelined and given no more information than the public about the meeting’s agenda or possible outcomes…
Before 1991, when newborns were not all vaccinated for hepatitis B, about 20,000 babies became infected each year. Routine immunization at birth cut the number of newborn infections … There are now fewer than 20 children per year who acquire the disease from their mothers.
Only about half of the cases before 1991 were a result of transmission from an infected mother. The other half “weren’t getting it from becoming sex workers, and they weren’t getting it from being intravenous drug users,” Dr. Paul Offit, director of the Vaccine Education Center at Children’s Hospital of Philadelphia, said…
From 2015 to 2017, about 21,000 infants were born to pregnant women with hepatitis B antibodies, but fewer than half were identified through prenatal screening, according to the C.D.C.
Related news article: Jackie Fortier, NPR 9/16/25 Link to 3 minute report: RFK Jr.’s vaccine panel is expected to recommend delaying hepatitis B shot in kids “:”A vaccine advisory panel, recently reshaped by RFK Jr., is expected to vote on changing the age children should get their first hepatitis B vaccine — from right after birth to age 4”
My take: If routine immunization at birth is stopped, there will be a lot more hepatitis B infections and subsequent complications. Some infections will be acquired at birth and some later due to missed opportunities to provide protection later on.
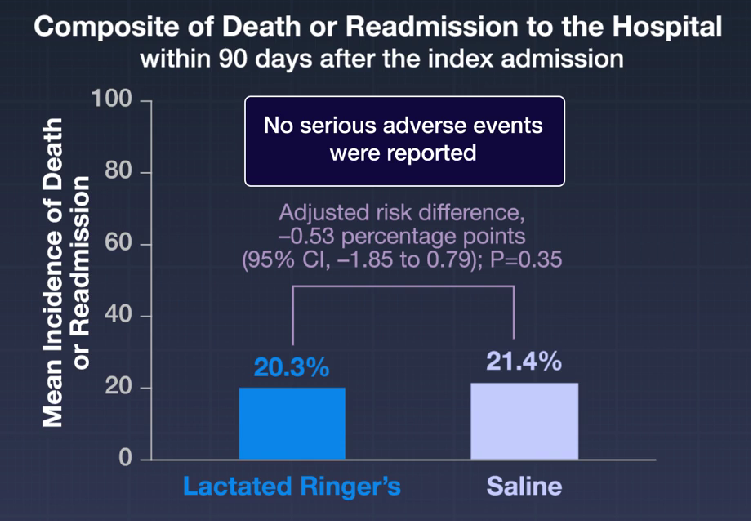
L McIntyre et al. NEJM 2025; 393: 660-670. A Crossover Trial of Hospital-Wide Lactated Ringer’s Solution versus Normal Saline
Background: “A single-center, multiple-crossover trial involving noncritically ill patients in the emergency department found that balanced crystalloid fluids were associated with a lower incidence of major adverse kidney events at 30 days than normal saline. A systematic review of 13 randomized, controlled trials comparing balanced crystalloids with normal saline in a total of 35,884 critically ill participants showed no significant difference in mortality (17.4% with balanced crystalloids and 18.2% with saline; relative risk, 0.96; 95% confidence interval [CI], 0.91 to 1.01) or in the incidence of the use of renal replacement therapy (5.6% and 6.0%, respectively; relative risk, 0.95; 95% CI, 0.81 to 1.11) in trials with a low risk of bias.4 However, the investigators in that analysis and those in another patient-level meta-analysis involving a Bayesian approach concluded that there is a high probability that balanced crystalloids are associated with lower in-hospital mortality and a lower incidence of the use of renal replacement therapy than normal saline.5“
Methods of th “FLUID” trial: 3 hospitals used lactated ringer’s (LR) and 4 hospitals used normal saline throughout hospital setting for 12 weeks. Then after a 1-2 week washout period, the hospitals switched to the other fluid for 12 weeks.
Key finding:
Discussion: “A limitation of this trial was the inability to recruit the total of 16 hospitals as originally planned owing to the Covid-19 pandemic. Hence, the trial had less power to detect differences that were small — but important to patients — at the level of the hospital or health care system…Our findings align with those of recent meta-analyses of randomized, controlled trials that suggest a small but clinically relevant reduction in mortality with balanced crystalloids as compared with normal saline.”
My take: This study did not show a significant difference in death or readmission at 90 days. Yet, lactated ringer’s is probably just a bit better fluid for most adult patients. In the pediatric population, more studies are needed.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition
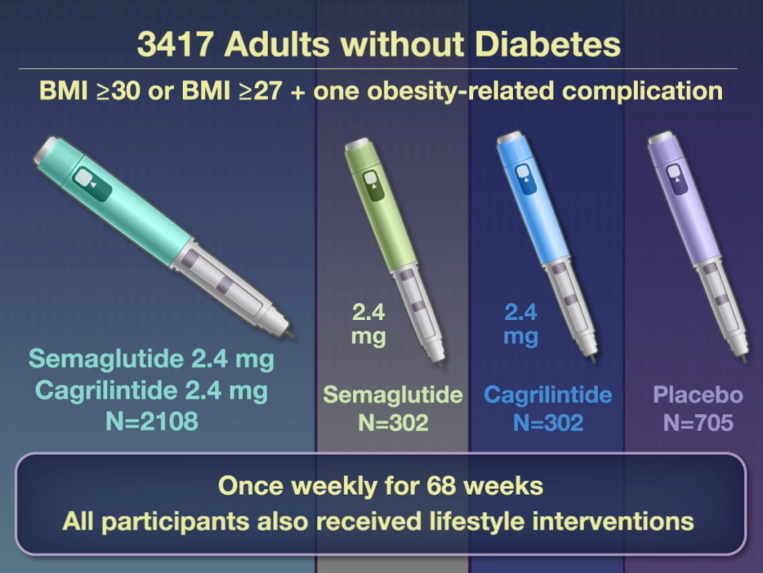
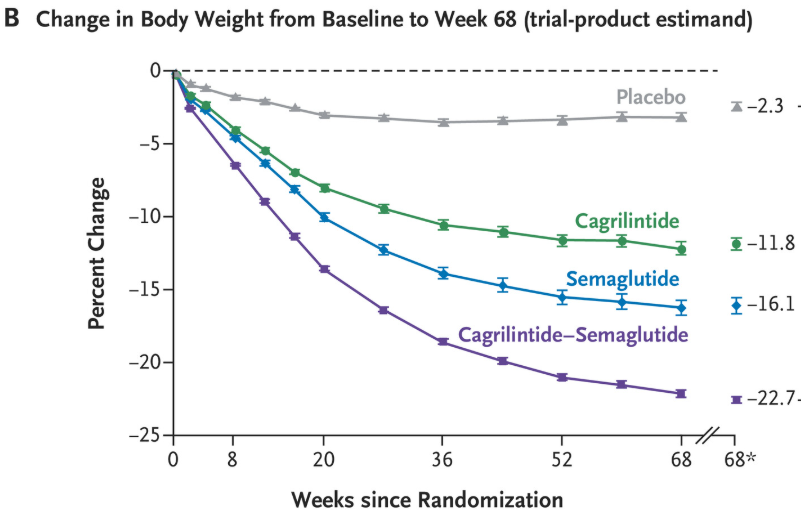
WTGarvey et al. N Engl J Med 2025;393:635-647. Coadministered Cagrilintide and Semaglutide in Adults with Overweight or Obesity
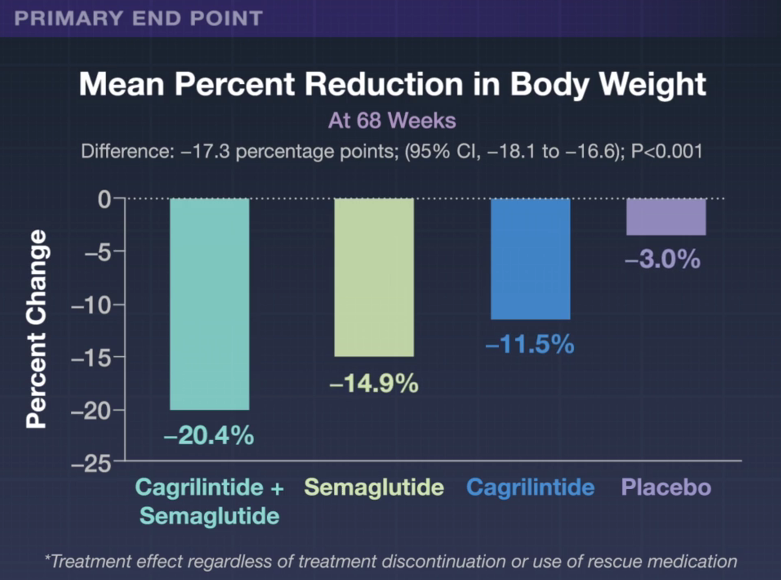
This phase 3a, 68-week, multicenter, double-blind, placebo-controlled and active-controlled trial (REDEFINE 1) examined the efficacy of the combination of Cagrilintide and Semaglutide (known as CagriSema). Patients had a body-mass index (BMI) of 30 or higher or a BMI of 27 or higher with at least one obesity-related complication. The combination druge was delivered as a fixed-dose in a single-dose, single-use pen device. 6.1% of trial participants had BMI <30.
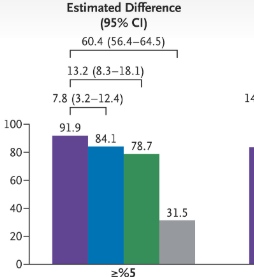
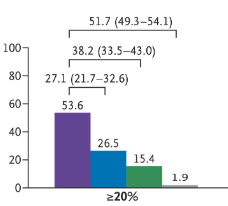
Percentage of patients with at least 5% weight loss Percentage of patients with at least 20% weight loss
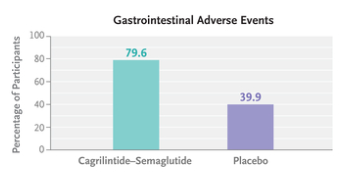
“Gastrointestinal adverse events (affecting 79.6% in the cagrilintide–semaglutide group and 39.9% in the placebo group), including nausea, vomiting, diarrhea, constipation, or abdominal pain, were mainly transient and mild-to-moderate in severity.”
“Although 57.4% of the participants assigned to cagrilintide–semaglutide were receiving the maximum dose at 68 weeks, 74.7% had received the maximum dose at some point after randomization…doses below the target might be highly effective for some patients and that dose reductions based on the clinical judgment…may be appropriate.”
This same issue also examined the use of this combination in patients with type 2 diabetes (REDEFINE 2). in this study with 1206 patients, “the estimated mean change in body weight from baseline to week 68 was −13.7% in the cagrilintide–semaglutide group and −3.4% in the placebo group.”
The editorial by CM Hales (“Expanding the Treat-to-Target Toolbox for Obesity and Diabetes Care”) notes that “six deaths occurred in the two trials combined, all in the cagrilintide–semaglutide groups, including one suicide in each trial. Previous studies of suicidality with GLP-1 receptor agonist treatment have not supported a causal link,6 but it continues to be of concern.”
My take (from the editorial): “A sustainable treat-to-target approach should extend to lifelong maintenance of health gains after initial weight loss. The intensity and composition of lifestyle interventions in the context of highly effective pharmacologic therapies also need further study. The pharmaceutical pipeline is promising, with potential improvements in safety (such as preservation of lean mass) and more convenience for patients (such as oral administration and monthly dosing). Greater effects on the health of Americans may be achieved not with antiobesity medications producing ever greater magnitudes of weight loss but with expanded access to safe and effective therapies for those who would most benefit.”
“A team of researchers found evidence of shady organizations churning out fake or low-quality studies on an industrial scale. And their output is rising fast, threatening the integrity of many fields…“If these trends are not stopped, science is going to be destroyed,” said Luís A. Nunes Amaral, a data scientist at Northwestern University and an author of the study”
““Science relies on trusting what others did, so you do not have to repeat everything,” Dr. Amaral said….By the 2010s, journal editors and watchdog organizations were warning that this trust was under threat. They flagged a growing number of papers with fabricated data and doctored images. In the years that followed, the factors driving this increase grew more intense.”
“As more graduate students were trained in labs, the competition for a limited number of research jobs sharpened. High-profile papers became essential for success, not just for landing a job, but also for getting promotions and grants. Academic publishers have responded to the demand by opening thousands of new scientific journals every year…”
“Organizations known as paper mills are now turning scientific fraud into a lucrative business. Scientists eager to pad out their resumes can pay hundreds to thousands of dollars to be named as an author of a paper that they had nothing to do with…paper mills often use artificial intelligence to alter the text they lift from other papers…”
“The papers that Dr. Amaral and his colleagues could study came to light only because of the work of independent sleuths. To estimate how many paper mill papers have yet to be exposed, Dr. Amaral’s team created a statistical model that accurately predicted the rate at which suspicious papers surfaced. They estimate that the number of paper mill products may be 100 times greater than the ones they have identified…”
“In their new study, they calculated that the number of suspicious new papers appearing each year was doubling every 1.5 years. That’s far faster than the increase of scientific papers overall, which is doubling every 15 years.”
““We need to stop making it profitable to game the system.”
My take: This problem has preceded the widespread use of AI, although Al makes it harder to detect. Unfortunately, fake scientific reporting appears to be worsening.
Related article: Jessica Steier NY Times 8/19/25: The Playbook Used to ‘Prove’ Vaccines Cause Autism This article details very specifically how David Geier (now appointed by RFK Jr to evaluate vaccines and autism) and his father have produced multiple flawed studies regarding vaccine safety. This commentary takes a particularly deep dive into one of his articles on the preservative thimerosol. She shows that the authors likely used p-hacking to identify “atypical autism” since there was not a significant association with autism, compared different time cohorts (the control group was from a period with different diagnostic criteria/lower rates of autism), did not include confounders, and supported their arguments with “personal citing.”
Some excerpts:
There have been some 70 studies since Mr. Wakefield’s looking for any link between vaccines and autism. Of these, 26 have linked vaccines to autism in some way, and 43 found no connection between vaccines and autism.
A whopping two-thirds of studies that claimed to have found a link were written by David and Mark Geier. These studies have been heavily criticized for using deceptive research techniques and flawed data.
Among the eight other studies that found a link, four were retracted for data manipulation, flawed methods or undisclosed conflicts of interest. Most of the authors have been involved in anti-vaccination campaigns and have had other papers retracted.
One such study that Mr. Kennedy referred to in his Senate confirmation hearing was published in a WordPress blog disguised as a journal and was funded by an anti-vaccine organization, among other problems.
Fortunately, independent scientists have conducted more than 40 high-quality studies since 1998 involving over 5.6 million people across seven countries. All found no connection between vaccines and autism. These studies were rigorously designed, were reviewed by independent peers and do not contain telltale signs of data manipulation, as the Geier studies do.
I was recently listening to a radio program (On Point) about the beneficial effects of sunlight.
The program notes that the potential beneficial effects of sunlight are much greater than the risks. Increased sunlight has been associated with lower rates of death, as well as lower rates of cardiovascular disease and autoimmune conditions like multiple sclerosis, type 1 diabetes, and Crohn’s disease.
When dermatologists recommend avoiding sunlight, they may be focused on the risks but not the benefits (though this varies among individuals). In addition, despite the more than 5-fold rise of melanoma diagnosis (especially in wealthy communities), there has not been a change in the rate of deaths due to melanoma. Skin cancers associated with sun exposure are mainly basal cell tumors and squamous cell tumors. These non-melanoma skin cancers have excellent survival rates.
Here is a link: The Healing Power of Sunlight (48 minutes) The most important part of this is in the middle, starting around 20 minutes.
My take: It’s a good idea to avoid sunburns but getting sunshine is good for health.
Related article:
Environ Epidemiol 2025. 9(3):e401. doi: 10.1097/EE9.0000000000000401. The association between time spent outdoors during daylight and mortality among participants of the Adventist Health Study 2 Cohort. Conclusion: “Moderate time outdoors in daylight during warmer months could be associated with lower risks of all-cause, CVD, and noncancer non-CVD mortality”