Recently Dr. DiLorenzo gave our group a brilliant lecture. I have taken some notes and shared some slides. There may be inadvertent omissions and mistakes in my notes. This is part 2 of my summary.
Key points (intermixed with slides):
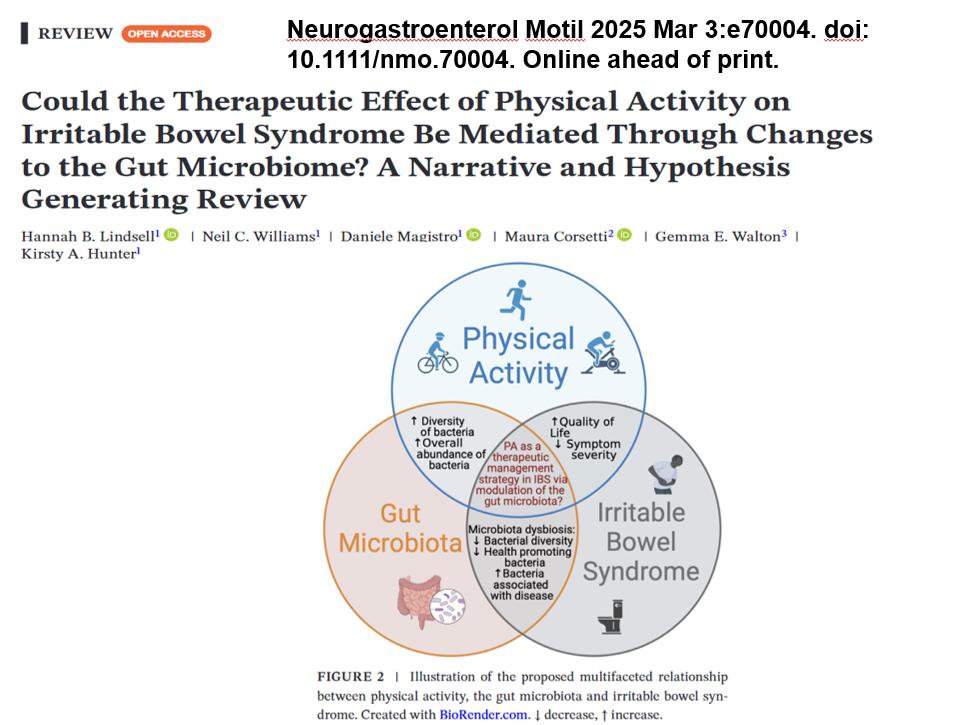
- Improving Physical activity, Diet and Sleep Often Helps DGBI symptoms
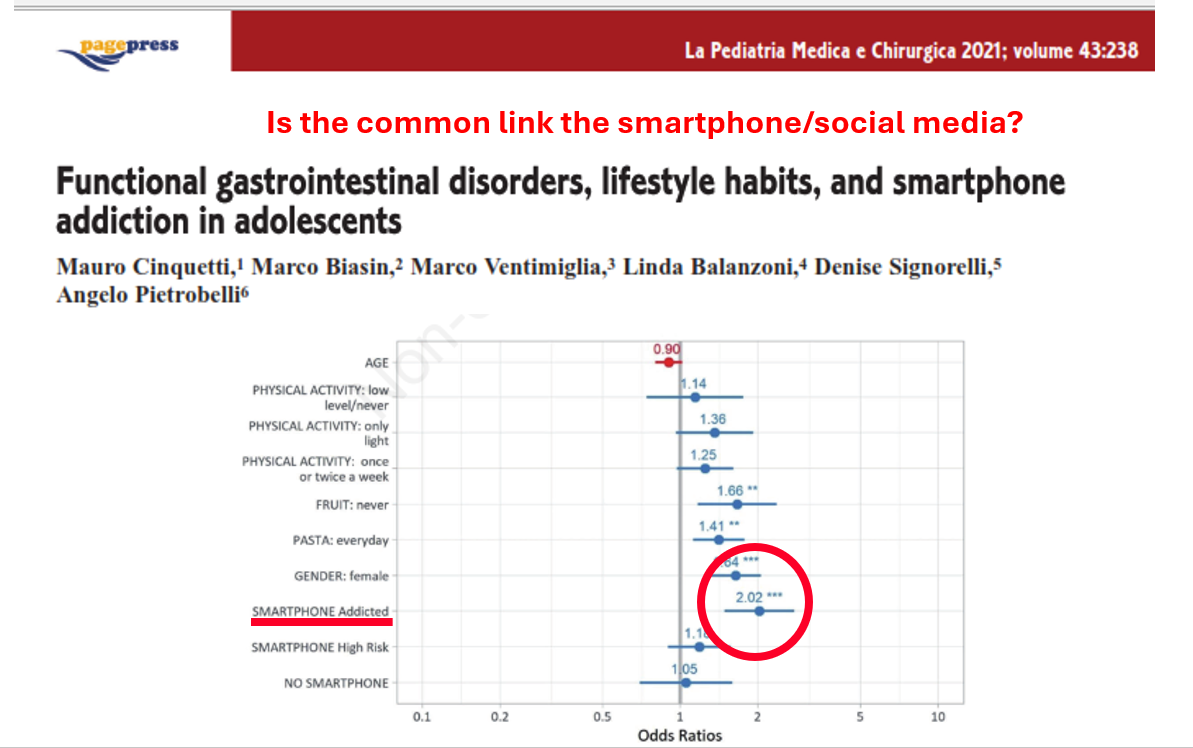
- Excess use of smartphones can be detrimental. There are issues with FOMO (fear of missing out), cyberbullying, effects on sleep, and effects on interpersonal skills
- Displacement, or replacing important activities (including physical activity) with time spent on social media, is a significant concern

- Working with pain psychologists is an important part of treatment for many children and adolescents
- Lots of celebrities have been open about their mental health challenges: Lady Gaga, Ariana Grande, Kristen Bell, Selena Gomez, Ryan Reynolds, and Dwayne “The Rock” Johnson
- For more serious mental health concerns, referral to psychiatry is more appropriate
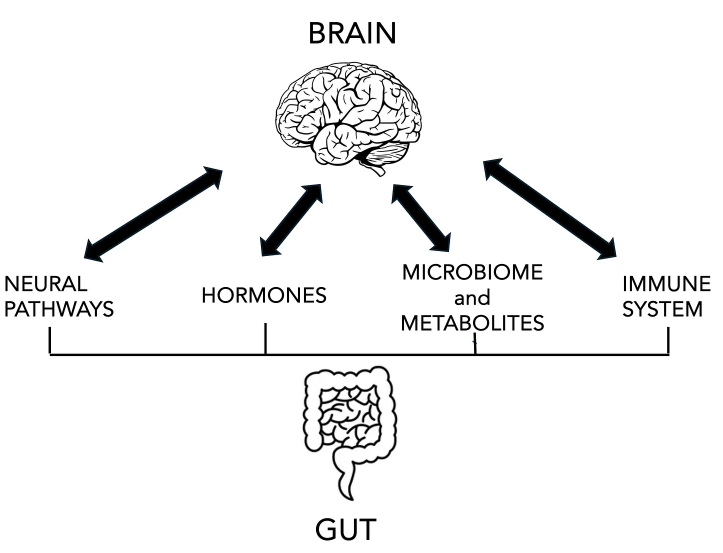
- Gut-Brain neuromodulators can be effective.
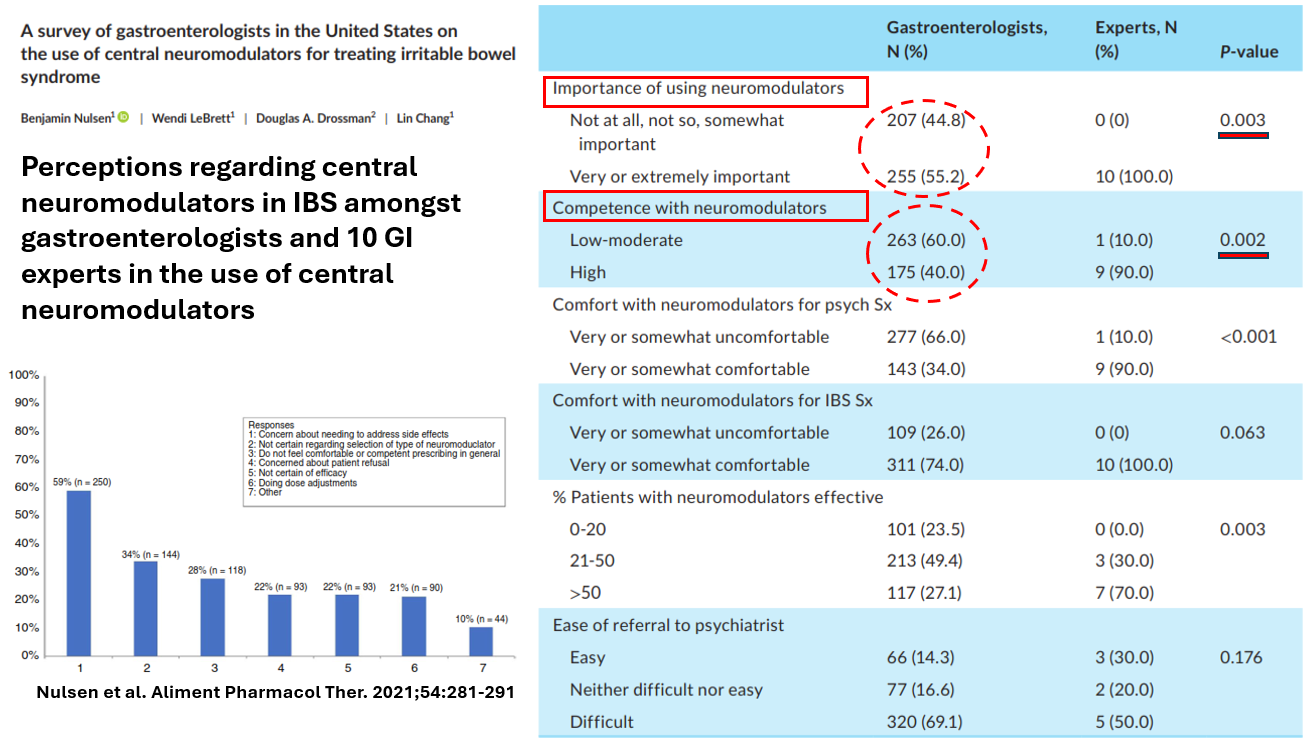
- Despite their good safety profile, they are underutilized
- Dr. DiLorenzo uses more citalopram than omeprazole
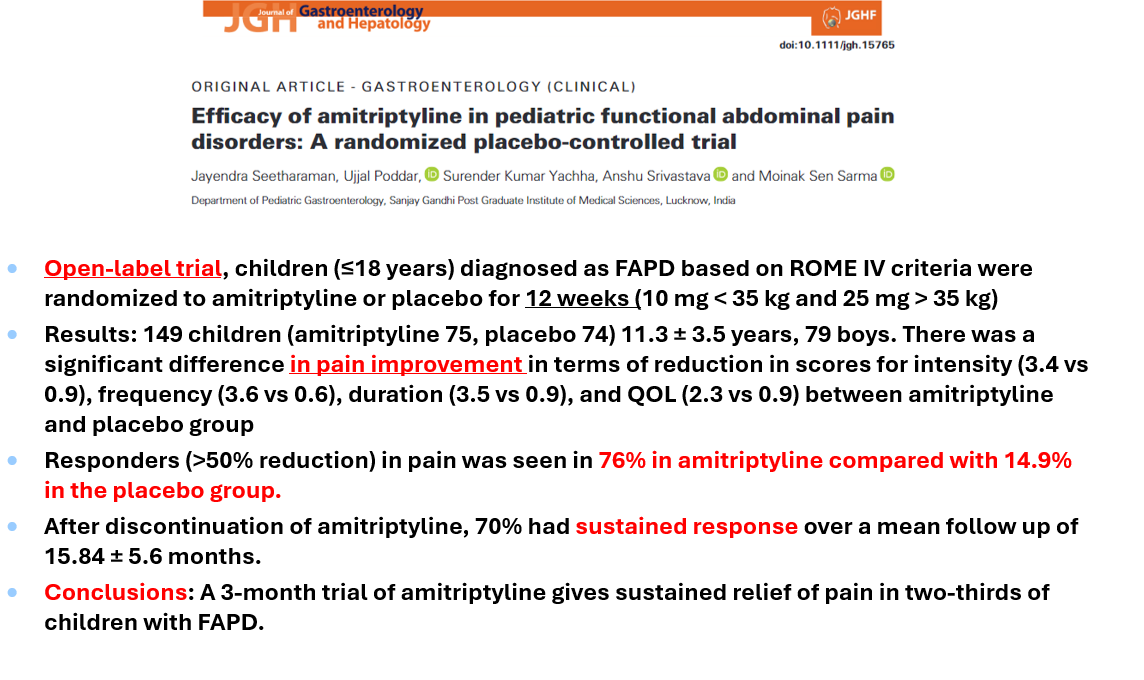
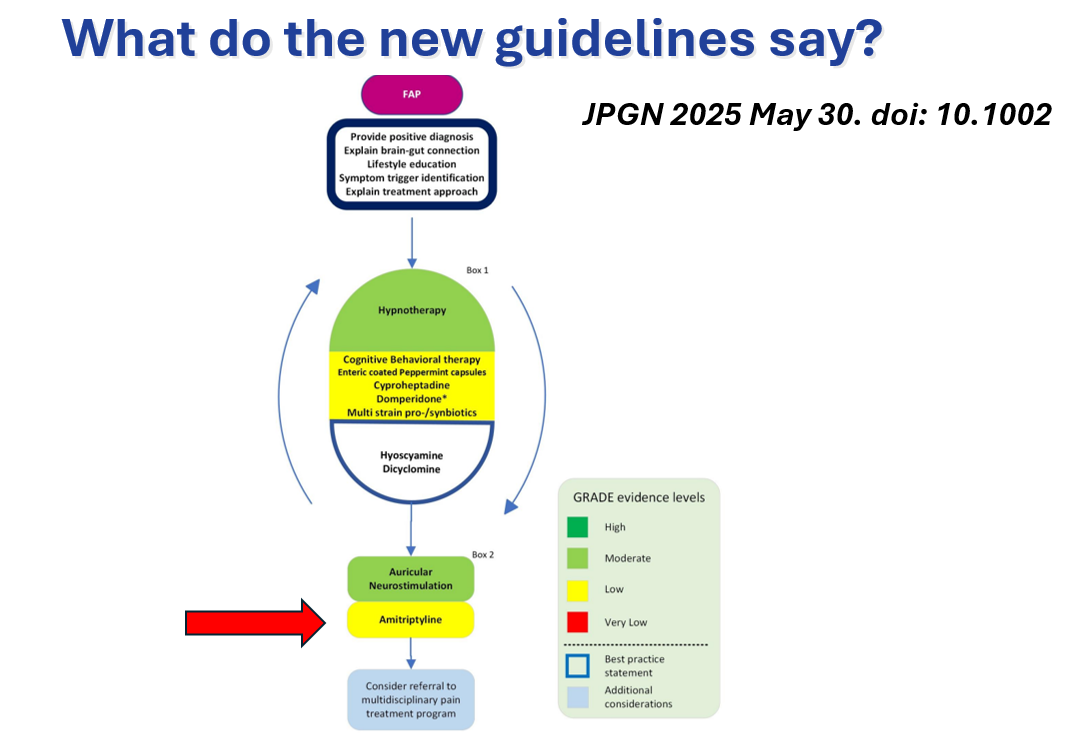
- Amitriptyline is often used for abdominal pain in the absence of anxiety. Variable results have been published
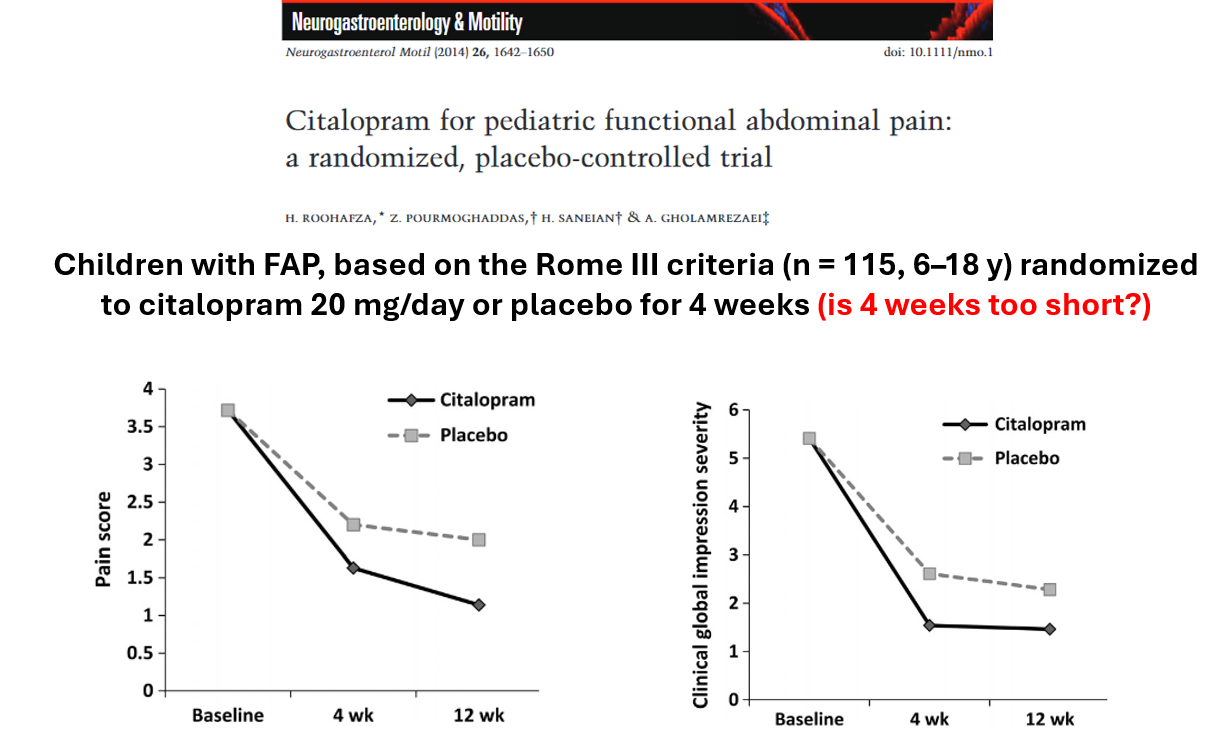
- Psychotropic medications: Amitriptyline is useful for pain predominant IBS, Citalopram often is effective for FAP/IBS with anxiety, Buspirone is helpful in dyspepsia with anxiety, and Mirtazapine is a good choice in the setting of dyspepsia with with weight loss. Generally, start with a low dose and slowly titrate with each medication
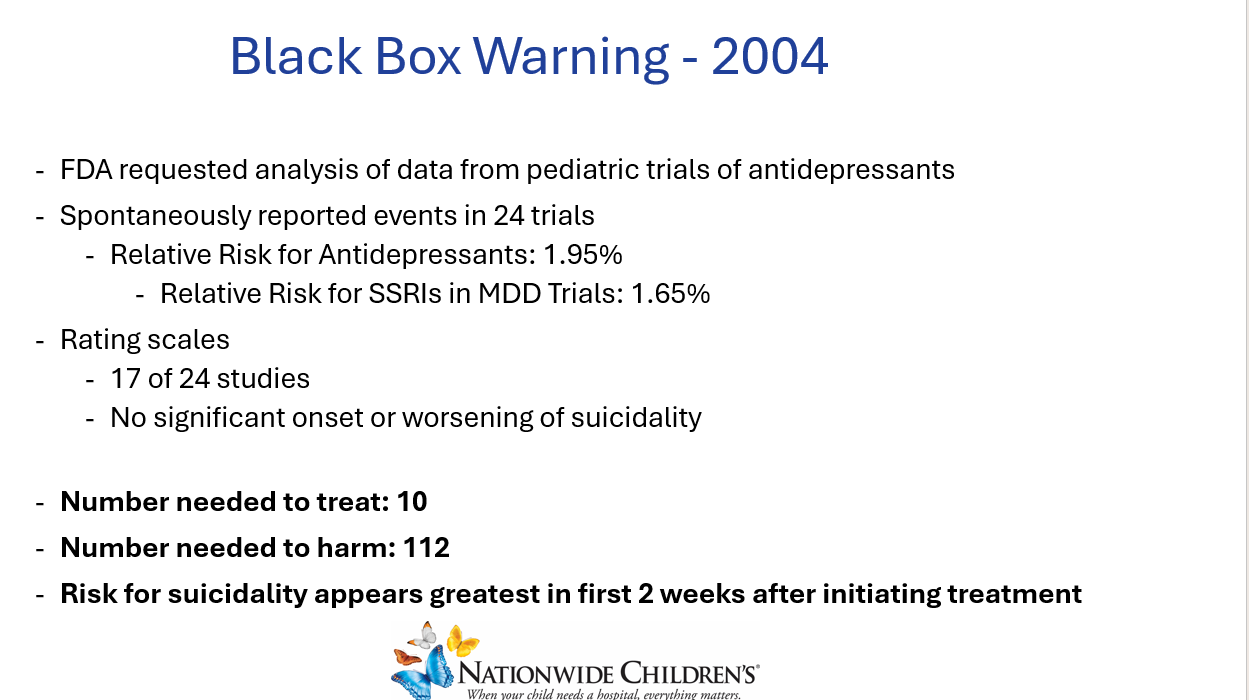
- Safety: Despite black box warning, recent studies have suggested SSRIs may lower the risk of suicidality overall

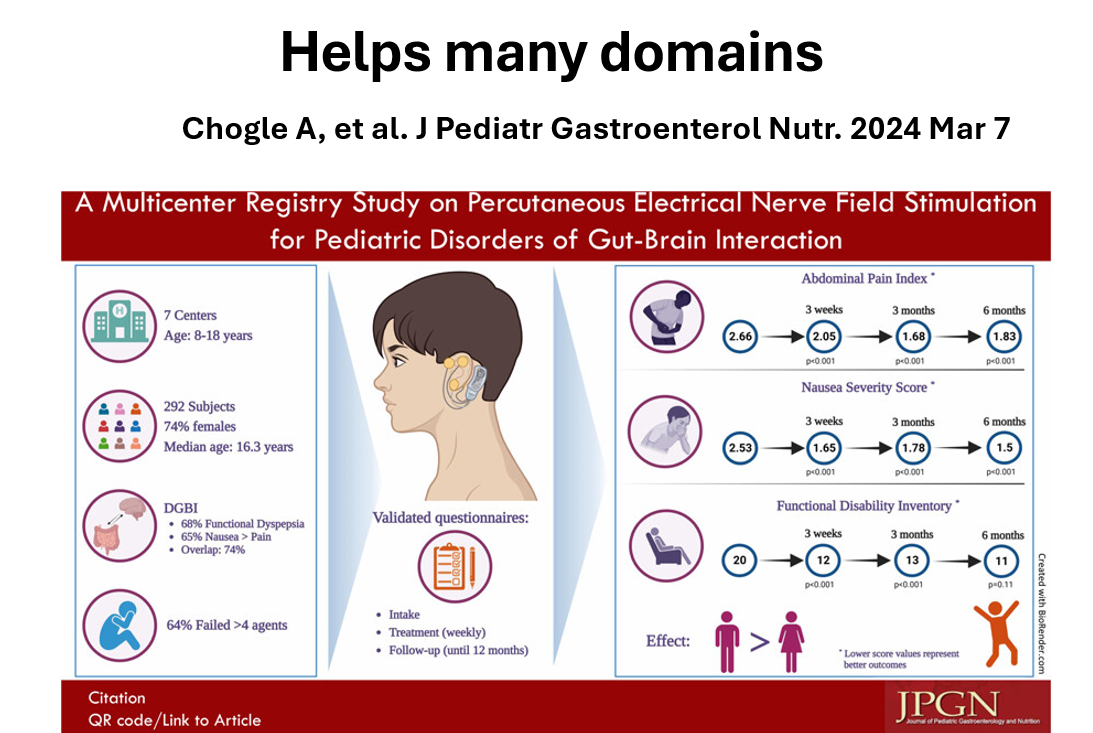
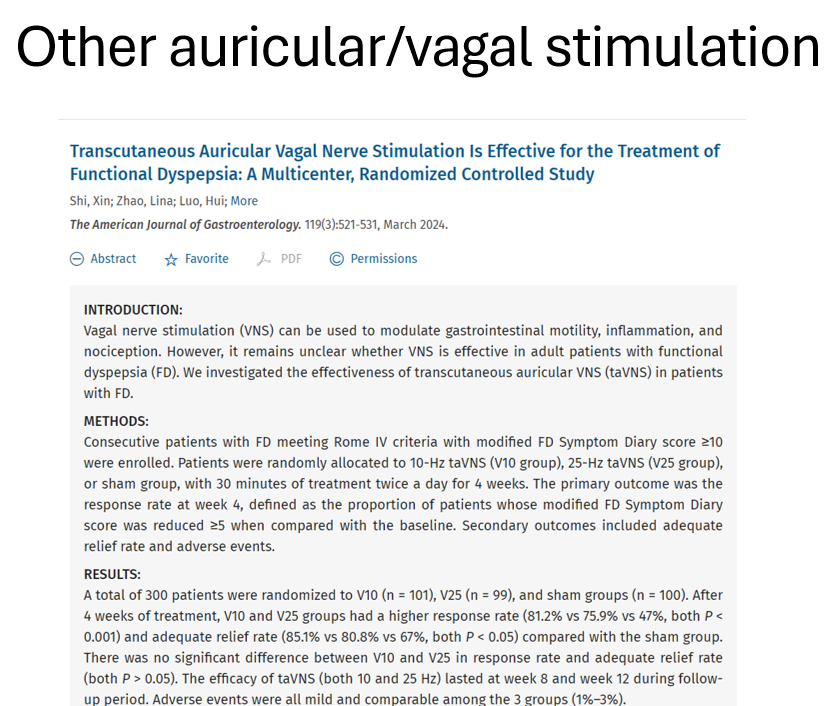
- Other treatments: PENFS (see also: Auricular Stimulation Associated with Less Pain, Less Disability, and Better Sleep)
- Don’t be the doctor who only tells patients things they want to hear. (Don’t be afraid of online rating)
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition