M Gibson et al. JPGN 2023; 77: 207-213. Safety and Durability of Accelerated Infliximab Dosing Strategies in Pediatric IBD: A Single Center, Retrospective Study
This pediatric retrospective study (n=291, 2010-2020) showed a high response to infliximab in patients with inflammatory bowel disease (n=234 Crohn’s disease (CD), n=53 ulcerative colitis (UC)) over a 10-period. Mean duration of treatment among study participants was 2.9 years. Key findings:
- 53% (n=135) started with doses of 10 mg/kg and 64% (n=87) of those who started on 5 mg/kg were dose-escalated; thus, approximately 76% of patients in their cohort needed doses of 10 mg/kg.
- Only 12% of patients discontinued treatment over the observed timeframe.
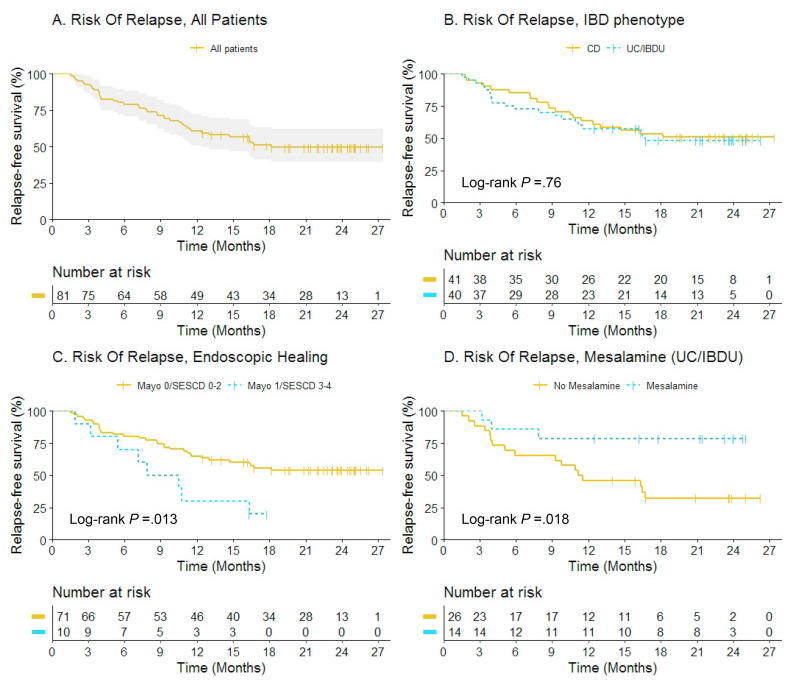
- Patients with UC (P ≤ 0.01) and patients with extensive disease (P = 0.01) had lower durability, despite a higher starting dose of IFX (P = 0.03). Figure 2 indicated that durability in CD was ~93% compared to ~60% for UC with HR of 5.12. The HR for extensive disease (n=77) was 3.74 compared to those with limited disease (n=108). Still, ~75% of those with extensive disease continued on treatment
- Common adverse events included 18 with skin findings (14 with psoriasis, 3 nonspecific rash, 1 with lupus), 23 with infusion reactions, 7 with AST/ALT >3 times ULN (or >120 IU/L), and 3 with serious infections.
Like the theme song from the 1996 Olympics (Reach, Gloria Estefan) reaching higher (dosing) resulted in being stronger (i.e.. better outcomes).
My take: This study showed really good outcomes associated with “accelerated” infliximab dosing.
Related blog posts:
- Another Study Justifying Higher Infliximab Dosing in Pediatrics
- Disease extent and need for higher infliximab dosing
- ARCH Study: Higher Doses of Infliximab in Acute Severe Ulcerative Colitis
- How Much Infliximab Can You Give to Young Children?
- “Denials, Dilly-dallying and Despair”
- Kids Are Different: Therapeutic Drug Monitoring
- Can Therapeutic Drug Monitoring with Monotherapy Achieve Similar Results as Combination Therapy?



Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.