A Le-Nguyen. N Engl J Med 2025;392:1215. Meconium Ileus
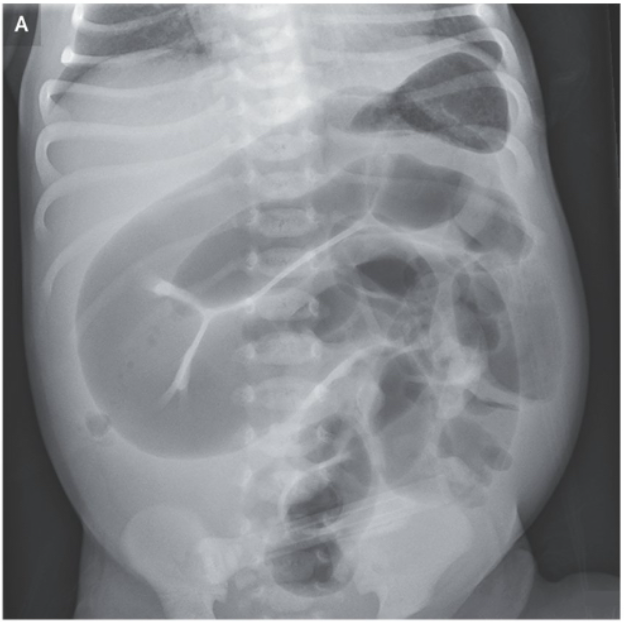
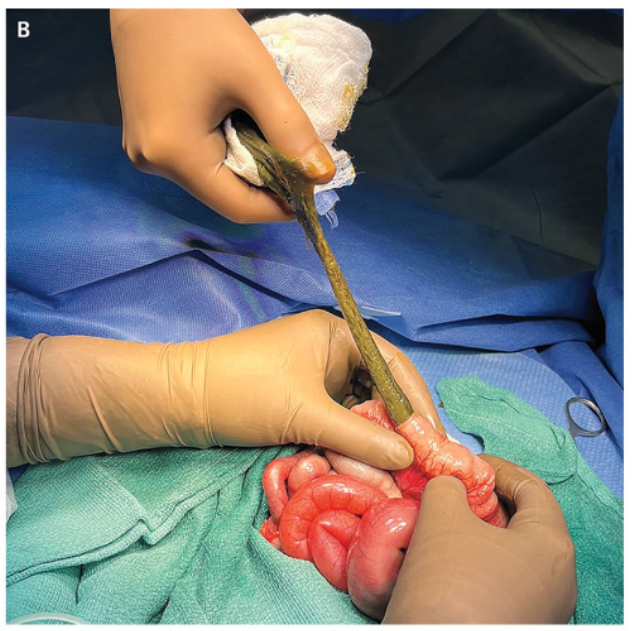
An abdominal radiograph had shown dilated loops of small intestine (Panel A). Owing to concern for intestinal malrotation with midgut volvulus, an urgent laparotomy was performed. Considerable distention of the small bowel by thick meconium — rather than midgut volvulus — was identified. An enterotomy for evacuation of meconium was performed (Panel B). On postoperative genetic testing, the baby was found to be homozygous for a mutation in CFTR, the gene encoding cystic fibrosis transmembrane conductance regulator… The condition is associated with a very high risk of cystic fibrosis, so genetic testing is warranted in all cases. Uncomplicated cases are typically managed with serial enemas.
Related blog posts:
- Impact of CFTR Modulators on the Need for Liver and Lung Transplantation in Patients with Cystic Fibrosis
- AAP GI Review Articles: GI Bleeding in the Neonate, Cystic Fibrosis in Neonates, and Intestinal Transplantation in Children
- Aspen Webinar 2021 Part 7 -Cystic Fibrosis Liver Disease
- Liver Briefs: Hereditary Angioedema/Liver Transplantation, Bulevirtide/PEG for HDV, and AASLD Cystic Fibrosis Guidance
- Delayed Diagnosis of Cystic Fibrosis and Long-Term Impact
- CHOA Nutrition Support Lecture: Cystic Fibrosis Nutrition -Changing in the Age of ‘Miracle Drug’