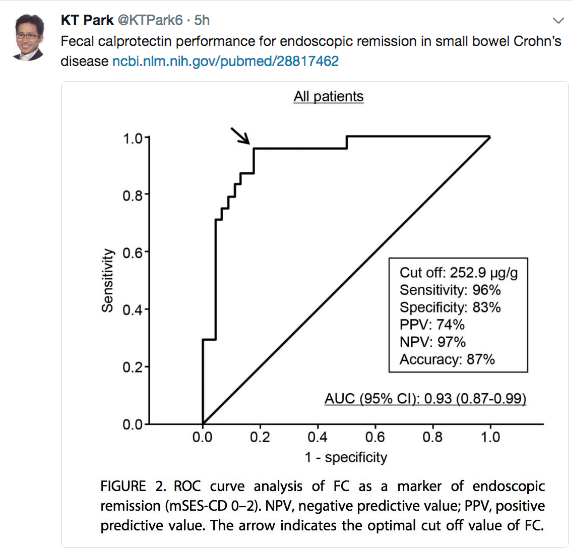
Thanks to KT Park’s Twitter feed for this reference: GA Holtman et al.
An excerpt from abstract:
Results Of the 16 eligible studies, authors of 8 studies (n = 1120 patients) provided their data sets. All blood markers and fecal calprotectin individually significantly improved the discrimination between pediatric patients with and those without IBD, when added to evaluation of symptoms. The best marker—fecal calprotectin—improved the area under the curve of symptoms by 0.26 (95% CI, 0.21-0.31). The second best marker—erythrocyte sedimentation rate—improved the area under the curve of symptoms by 0.16 (95% CI, 0.11-0.21). When fecal calprotectin was added to the model, the proportion of patients without IBD correctly classified as low risk of IBD increased from 33% to 91%. The proportion of patients with IBD incorrectly classified as low risk of IBD decreased from 16% to 9%. The proportion of the total number of patients assigned to the intermediate-risk category decreased from 55% to 6%.
Conclusions and Relevance In a hospital setting, fecal calprotectin added the most diagnostic value to symptoms compared with blood markers. Adding fecal calprotectin to the diagnostic workup of pediatric patients with symptoms suggestive of IBD considerably decreased the number of patients in the group in whom challenges in clinical decision making are most prevalent.
From: Inflamm Bowel Dis. 2017 Aug 16. doi: 10.1097/MIB.0000000000001202. [Epub ahead of print]