CDC Study: “From late August 2024 to early September 2025, the vaccines reduced the risk of Covid-related emergency room and urgent care visits by 76% among children ages 9 months to 4 years, and by 56% among children ages 5-17, according to the study”
Citation: Irving SA, Rowley EA, Chickery S, et al. Effectiveness of 2024–2025 COVID-19 Vaccines in Children in the United States — VISION, August 29, 2024–September 2, 2025. MMWR Morb Mortal Wkly Rep 2025;74:607–614. DOI: http://dx.doi.org/10.15585/mmwr.mm7440a1
Between the end of February and mid-August, funding ceased for 383 studies that were testing treatments for conditions including cancer, heart disease and brain disease. The cuts disproportionately impacted efforts to tackle infectious diseases like the flu, pneumonia and COVID-19, researchers found…
More broadly, the lost research harms patients who could have benefited from a possible new treatment, researchers said in the report published Monday in the journal JAMA Internal Medicine…
“The whole purpose of these clinical trials is to generate evidence on what works and doesn’t work in medicine,” said study co-author Anupam B. Jena with Harvard Medical School. Researchers counted 11,008 NIH-funded studies during the study period. Of those, 1 in 30 lost funding.
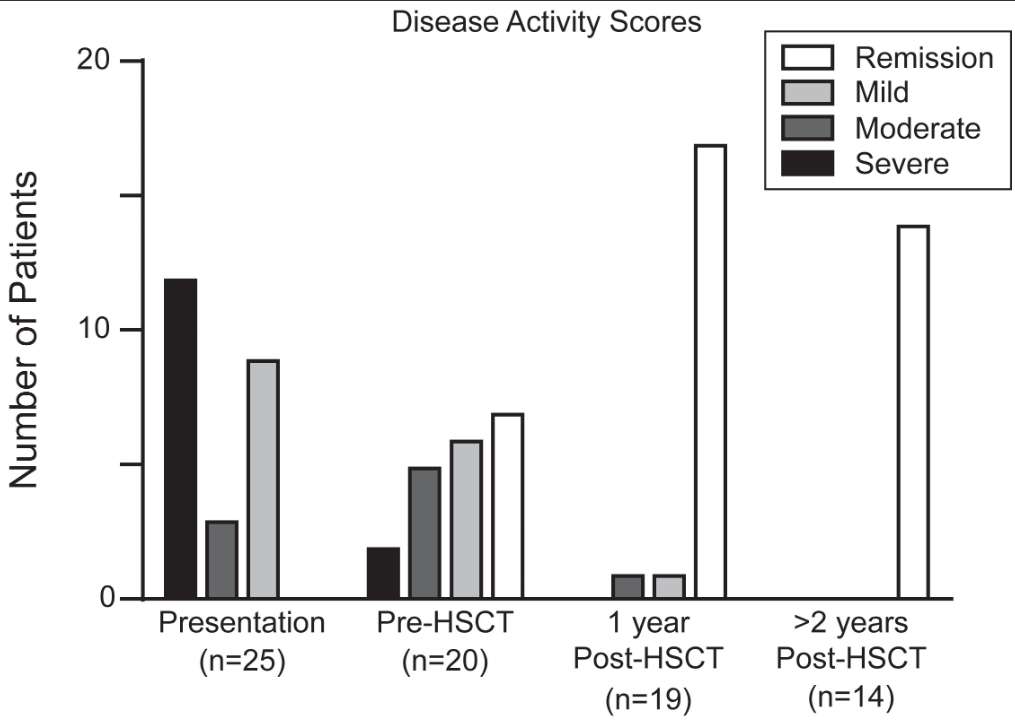
This was a retrospective single-center (CHOP) study of 25 children with monogenic IBD who underwent Hematopoietic Stem Cell Transplant (HSCT) (2012-2022).
Key findings:
Seventy-two percent of patients had Crohn’s Disease, and 28% were classified as IBD-unspecified. Ninety-two percent of patients had VEO-IBD, 56% presenting under age 1
At most recent follow-up, 92% of patients achieved sustained medication-free remission of IBD and 60% with prior ostomy underwent re-anastomosis. There was 100% survival at a median follow-up of 3 years
There was significant improvement in growth, hospital days, and severe infections
Disease activity scores at the time of IBD presentation, immediately prior to transplant, 1-year post-transplant, and at most recent follow up if ≥2 years since transplant.
Discussion points:
“Delay of HSCT with the goal of obtaining remission of IBD prior to transplant may prove to be determinantal, as outcomes of HSCT are in general improved for younger patients,20 and medical remission is often unattainable for more severe forms of monogenic IBD. Within our cohort, 32% of patients had moderate or severe disease at the time of transplant despite medical optimization. None of these patients developed intestinal GVHD, which was a rare event in our total cohort”
“HSCT is not without risk, and complications occurred in our cohort, at rates typical of other IEI cohorts”
“The selection of patients who would benefit from HSCT requires multidisciplinary discussion.”
With regard to patient selection, one item that was not included in the discussion was the one patient excluded from their analysis who had a TTC7A gene defect. In the results section, it was explained that the patient with “TTC7A was subsequently excluded as transplant was performed for the indication of SCID alone, rather than treatment of intestinal disease.” More discussion on this point is merited as many centers would NOT have a patient with TTC7A undergo HCST specifically because it cannot correct the underlying bowel disease.
Also, it was noted that one patient with CTLA4 deficiency had undergone HSCT prior to the discovery of the genetic defect. With the more widespread use of genetic testing available now, this discovery may have obviated the need for HSCT as treatment with abatacept is typically effective.
My take: Overall, the authors present impressive results for HSCT for monogenic IBD and strengthen the need for genetic testing in those with early onset disease and those refractory to treatment.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
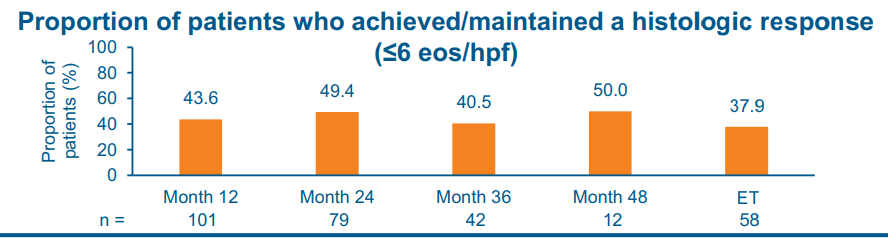
The study by Dellon et al was a 4-year, phase 3, open-label study in patients with EoE who completed up to 52 weeks of BOS therapy (Budesonide oral suspension 2 mg 2/day) in 2 preceding phase 3 studies.
Key findings:
At month 48 of treatment, 50.0% and 58.3% of patients achieved/maintained a histologic response (< or =6 and <15 eosinophils per high-power field, respectively)
Safety:
Treatment-emergent adverse events (TEAEs) occurred in 76.3% of patients; most were mild/moderate in severity and unrelated to study drug.
The most frequently reported BOS-related TEAEs included abnormal adrenocorticotropic hormone stimulation test results (8.4%, 11/131; number of events [m] [ 12) and adrenal insufficiency (2.3%, 3/131; m [ 3). Esophageal candidiasis occurred in 3.1% of patients (4/131)
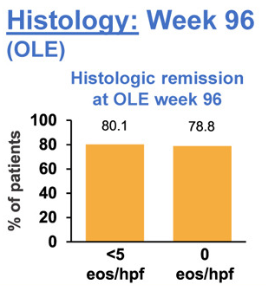
The study by Biedermann et al explored the use of an orodipsersible tablet for EoE up to 3 years in patients who achieved remission during a 12-week induction. This tablet is not available in the U.S.
Key findings:
At week 96, 80.1% of patients were in histologic remission, defined as peak eosinophils per high-power field of <5, at week 96 vs 91.8% at open label extension baseline
No new safety concerns were observed across 96 weeks of treatment. Suspected symptomatic candidiasis occurred at similar rates to prior BOT studies and was predominantly mild and resolved with treatment
My take: The pharmaceutical budesonide suspension, Eohilia, is labelled by the FDA for use as a 12 week treatment course. Since EoE is a chronic disease, 12 weeks is insufficient. These long-term studies provide data that may address this shortcoming.
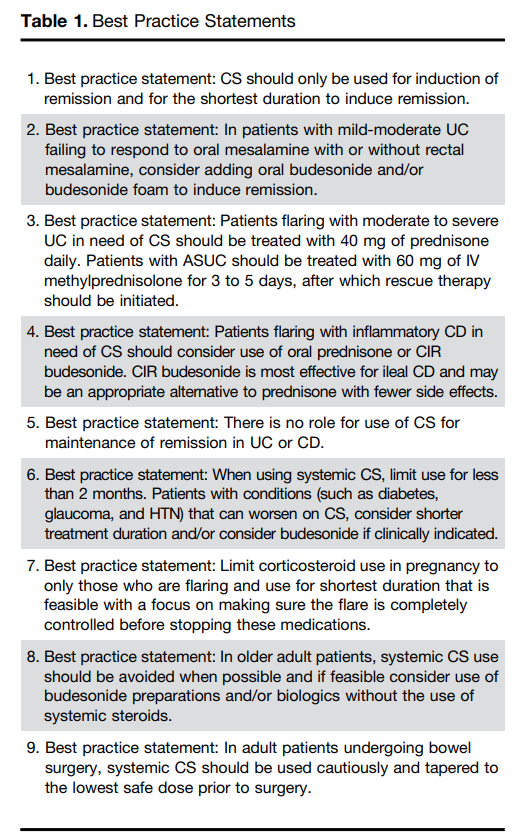
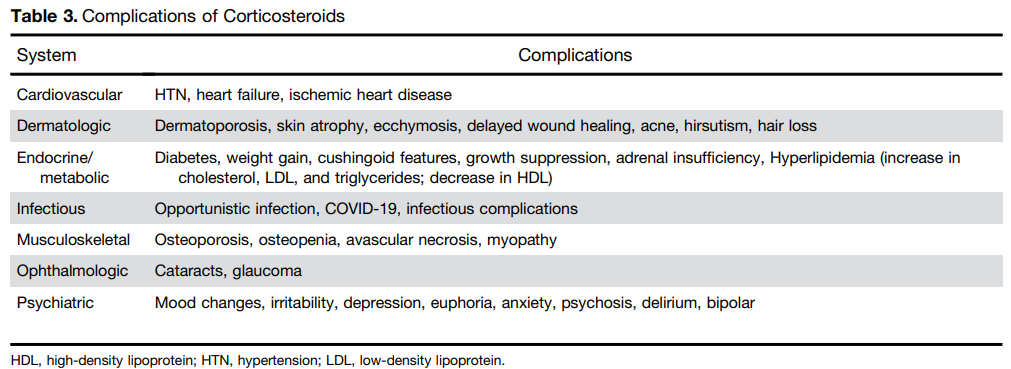
Steroids are commonly used and misused for inflammatory bowel disease. This article reviews best practices, steroid formulations/dosing, and potential complications.
For moderate to severe ulcerative colitis (in adults), the authors recommend treatment with 40 mg of prednisone daily. Patients with ASUC (acute severe ulcerative colitis) should be treated with 60 mg of IV methylprednisolone for 3 to 5 days, after which rescue therapy should be initiated
Use of budesonide is recommended as an option for many clinical situations to minimize steroid adverse effects. These situations include mild-moderate UC failing to respond to mesalamine, ileal CD and older patients
Postoperative complications: “In the postoperative period, patients treated with CS had a higher risk of both infectious complications (aOR, 3.69; 95% CI, 1.24–10.97) and major infectious complications (aOR, 5.54; 95% CI, 1.12–27.26) [Abrerra et al].135 Subramanian pooled data from 7 studies showing that preoperative CS use is associated with increased postoperative complications (OR, 1.41; 95% CI, 1.07–1.87) as well as infectious complications.
The authors note that corticosteroids “remain widely available and are an effective short-term option for induction of remission in patients with active UC or inflammatory CD. However, their well-described and significant safety profile warrants proactive strategies to limit their use through non-systemic formulations, short-term exposures, steroid-sparing maintenance options, and most recently, complete steroid avoidance strategies.”
My take: Continuing steroids when they are not effective prior to potential surgery (eg. ASUC) remains a frequent problem. Sometimes, it is difficult to know it they are helping some.
M Hook et al. JPGN 2025; DOI: 10.1002/jpn3.70221. Esophageal coin with moth eaten appearance: A cause for caution
This case report describes a penny ingestion by a 10 yo with autism that likely happened nine months before attempted retrieval. The coin was not able to be retrieved due to stricturing but was advanced into the stomach (the authors note advancement into duodenum would be better); in addition, there was an esophageal diverticulum that was identified likely secondary to the caustic damage.
In the discussion, the authors note that “the ‘moth eaten’ appearance is a rare finding that indicates prolonged foreign body retention and unforeseen mucosal injury…It is specific to post-1982 pennies, composed of 97.5% zinc.4 Hydrochloric acid exposure dissolves zinc, forming caustic zinc chloride.”
My take: Future generations will not see this radiologic finding. For now, if this finding is seen, it likely indicates a more difficult foreign body removal.
For those trying to understand the success of the current HBV immunization strategy and why altering the timing of HBV vaccinations is a bad idea, this is a worthwhile article.
Key points:
“To date, more than 1 billion doses of HepB vaccines have been administered worldwide, and they are considered one of the safest and most effective vaccine ever made.1,2,6“
“Because of the high risk for chronic HBV infection, the CDC/Advisory Committee on Immunization Practices (ACIP), WHO, and health ministries of many countries recommend universal HBV vaccination of all infants beginning with a “birth dose” for newborns, preferably within the first 24 hours of birth, followed by completion of the 3-dose infant vaccination schedule…Implementation of routine infant and childhood vaccination, including birth dose HBV vaccine, prevented an estimated 210 million infections globally between 1980 and 2015.4“
“In 1991, with evidence showing substantial number of infants and others at risk were missed by a risk-based approach to HepB vaccination, the ACIP recommended universal HepB vaccination for all infants, with the first dose administered before hospital discharge along with hepatitis B immune globulin (HBIG) for infants born to mothers who tested positive for HBsAg or whose HBsAg status was unknown.5,6,14“
“In 2018, the CDC/ACIP recommendation specified that the birth dose of HepB vaccine should be administered within 24 hours of birth including for preterm infants, regardless of maternal HBsAg status.14 …Timely birth dose HepB vaccination regardless of maternal HBsAg status serves as a safety net for perinatal transmission from HBsAg-positive mothers missed by HBsAg screening programs and protects against the small but non-zero risk of HBV infections from household and other exposures for infants born to HBsAg-negative mothers.”
“HepB vaccination alone prevents 75% to 80% of perinatal HBV transmission.2 The addition of maternal HBsAg screening and further testing for hepatitis B e antigen or HBV DNA if HBsAg test is positive allows for additional interventions to eliminate mother-to-child transmission of HBV.”
US CDC recommendations for HBV vaccination. Decline in reported number of acute HBV infections in the United States in association with CDC recommendations for HBV vaccination, 1980–2022.
My take (borrowed in part from authors): It would be a big mistake to resume the risk-based approach to newborn HepB vaccination. “HepB vaccine is a safe and highly effective vaccine. HepB vaccination prevents an incurable chronic infection and related morbidity and mortality from cirrhosis and HCC. Indeed, HepB vaccine is the first cancer-prevention vaccine…Universal HepB birth dose vaccination regardless of maternal HBsAg status is the most effective as well as the most cost-effective strategy in eliminating HBV infection. Newborns and infants are those at highest risk of chronic HBV infection. Delaying the first dose of HepB vaccine even by a few days exposes the infants to increased risk of developing lifelong infection,18 chronic liver disease, and premature death.”
“Delaying the first vaccine in the series to one-month, four years, or 12 years of age will undermine the vaccine’s effectiveness, and relying on just screening pregnant women for hepatitis B is insufficient.
Although some of the changes that have been discussed by ACIP sound small, they are not grounded in new evidence and would undo more than three decades of a prevention strategy that has nearly eliminated early childhood hepatitis B in the United States.“
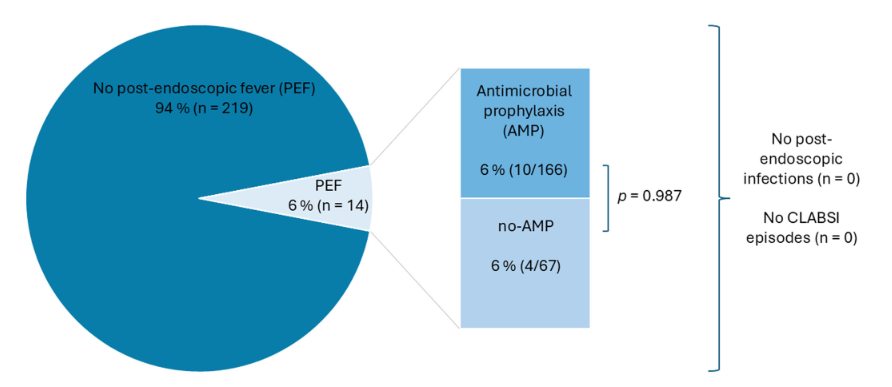
Methods: This was a retrospective single-center observational study which included children with IF and CVC who underwent GI endoscopy between 2019 and 2024. Intravenous antibiotic prophylaxis was used in 71.2% of the procedures.
Key findings:
The overall post-endoscopic fever (PEF) rate was 6%, with no significant difference between the group that received prophylactic antibiotics and the group that did not. Specifically, there were 10 with PEF that had received prophylactic antibiotics and 4 that had PEF with no prophylaxis
No infections, including central line-associated bloodstream infections, were observed
5/14 of the cases with PEF had an interventional procedure. The remainder had a diagnostic EGD, colonoscopy or both.
Interventional Cases:
Discussion Points:
“PEF in children with IF was 6%, which is approximately 10 times higher than the recently published 0.55% in pediatric patients following endoscopic procedures by Boster et al.” (see: Must-Read: How to Handle Post-Procedure Fevers)
A strength of this study was that the comparison of children with IV antibiotics versus those without was due to an institutional policy change in 2022. This helps eliminate selection bias in the determination that IV antibiotics were not beneficial in preventing PEF
My take: The high rate (6%) of PEF should be discussed with families prior to endoscopic procedures. The rate was increased (36%) in those with interventional procedures. It is reassuring that no definitive infections were identified despite the fevers.
This article reviews the growing health concerns regarding microplastics and nanoplastics (MNPs) specifically regarding the GI tract.
Key points:
“As these [plastic] products degrade, they break down into smaller particles, forming microplastics (< 5 microm) and nanoplastics (<1 microm), collectively referred to as MNPs”
“Although many plastic products are deemed recyclable, in the United States, less than 10% are actually recycled…annual global production projected to reach 1.1 billion tons by 2025. Simultaneously, over 12 billion tons of plastic wastes are expected to accumulate in landfills”
“The average American ingests approximately 5g of plastic per week, equivalent to 1 credit card, and 39,000–50,000 particles annually”
Potential association of MNPs with metabolic-associated steatotic liver disease, liver and pancreatic cancer and inflammatory bowel disease. “Studies have reported significantly higher levels of MNPs in patients with IBD compared with healthy controls.”
In a related article in Gastroenterology and Endoscopy News (October 2025), Dr. Johnson noted that “reduction of plastic intake from bottled water to tap water in one study reduced microplastic intake, the number of particles within human tissues, from 90,000 to 4,000…Avoid heating food in plastics…the effect of microwave increased the evidence of microplastics by over 4.2 million and the nanoplastics, 2 billion, just in three minutes in the microwave.”
My take: Something that almost everyone could agree on – they would like less plastic in their food and environment. How to achieve this is much more difficult.
JM Perrin, TL Cheng. NEJM 2025; 393: 1869-1872. “Truly Prioritizing Child Health — The Missed Opportunities of the MAHA Commission”
This commentary welcomes the attention to child health which was a focus of the MAHA commission. This review provides perspectives on the stated policy aims and on what else is needed.
An excerpt:
The [MAHA] commission has highlighted four specific areas of concern: poor diet, environmental chemicals, lack of physical activity and chronic stress, and overmedicalization. The strategy outlined in the MAHA Commission’s recent report, however, misses real opportunities to address the chronic disease epidemic and “whole-person health”…
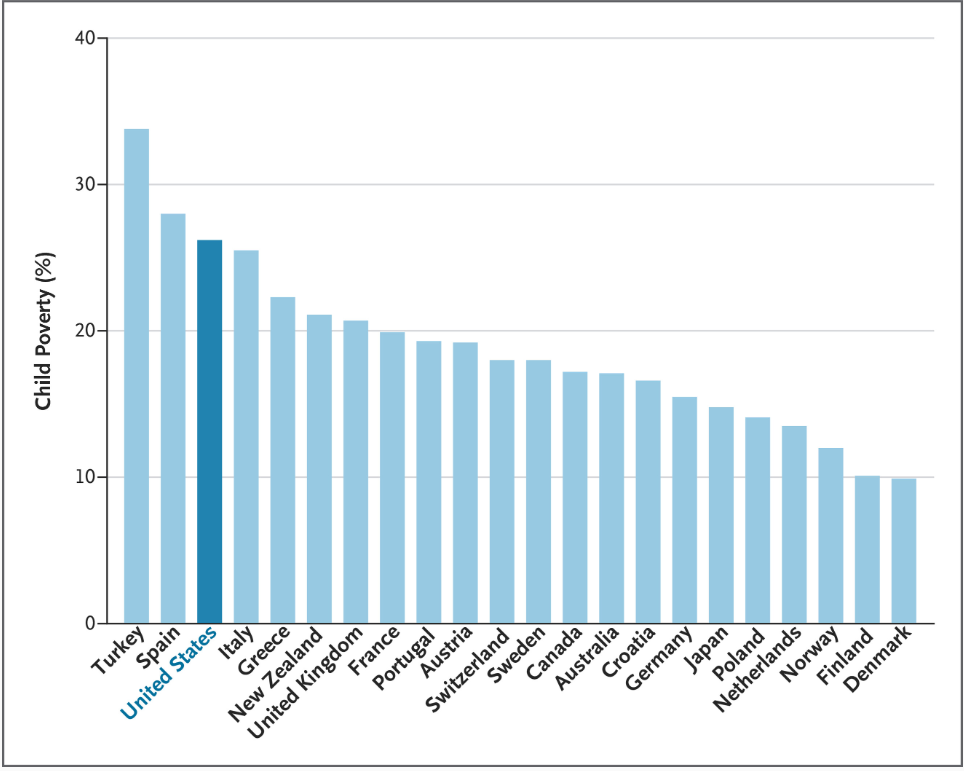
The MAHA Commission’s view of the state of U.S. child health ignores leading contributors to rising childhood morbidity and mortality: firearm injuries (the leading cause of death among U.S. children), drug overdoses, and motor vehicle injuries. Most striking is the commission report’s silence regarding the association of poverty with poor child health… which contributes to higher rates of asthma, obesity, and mental health conditions...
The first MAHA priority, children’s diets, has long been a concern of the U.S. child health community, particularly the intake of sugar-sweetened beverages, excessive portion sizes, and food additives. But pediatricians and researchers also know that food insecurity, food-industry marketing practices, and limited access to healthy foods are prime drivers of childhood obesity rates. Nutritious meals require money…
The MAHA strategy recommends marginal changes to the diets of U.S. children, such as reducing the use of food dyes and reducing consumption of ultraprocessed foods, even as the government is increasingly limiting public food assistance.
The commission’s focus on environmental chemicals is appropriate, given that exposures to potentially toxic chemicals in foods, household supplies, cleaning agents, farm supplies, and elsewhere have grown dramatically. The MAHA strategy provides little relief, however: a few research projects and no regulatory change…The MAHA report stops short of recommending the research and regulatory reform necessary for identifying, restricting, and mitigating harmful exposures.
Concerns about physical activity and stress are also justified. Many studies have documented alarming declines in physical activity, examined the causes and effects, and found associations with mental health and well-being… Strengthening early-childhood, school-based, and community-based physical activity programs, as well as social media strategies for promoting lifestyle changes, could improve health and reduce stress among young people, but the MAHA Commission mainly orders schools and communities to increase physical activity.
Finally, the commission has raised concerns about medications, especially stimulants and psychotropic agents…In response, the MAHA Commission primarily proposes studying prescribing patterns and “solutions that can be scaled up to improve mental health.” It does not address more fundamental ways of changing medication use…
Despite its attention to children’s health, the MAHA Commission’s lengthy list of aspirations and recommended changes is unlikely to make a real impact. Instead, next steps should include implementing policies, programs, and research supported by the strong evidence base that clinicians and investigators have built painstakingly for many years.
My take: The policies pursued by the current administration like limiting food dyes do not target the big drivers of poor health outcomes in children.
The authors of this commentary also “chaired the National Academies of Sciences, Engineering, and Medicine (NASEM) study described in “Launching Lifelong Health by Improving Health Care for Children, Youth, and Families”1 [which] provides clear, evidence-based lessons that could help in achieving MAHA objectives.”
Childhood Poverty Rates: Shown is the percentage of children in households with incomes below 60% of the median national income. Data are from UNICEF and reflect averages from 2019 through 2021.