I never saw the show, “Office Space.” However, I did see the opening trailer (1 min) recently and it is very funny. YouTube Link: Office Space – Peter’s Original Traffic Scene

MB Wallace et al. Gastroenterol 2022; 162: 295-304. Open access: Impact of Artificial Intelligence on Miss Rate of Colorectal Neoplasia
Design: In a multicenter and multicountry randomized crossover trial, patients (n=230) undergoing CRC screening or surveillance were enrolled in 8 centers (Italy, UK, US), and randomized (1:1) to undergo 2 same-day, back-to-back colonoscopies with or without AI (deep learning computer aided diagnosis endoscopy) in 2 different arms, namely AI followed by colonoscopy without AI or vice-versa.
Key finding: There was an approximately 50% reduction of the miss rate of colorectal neoplasia, mainly due to a decreased miss rate of flat and small lesions.
The editorial (pg 35-38, DK Rex et al. Artificial Intelligence Improves Detection at Colonoscopy: Why Aren’t We All Already Using It?) provides some perspective regarding the study limitations and why AI will not be widely adopted in the near term.
Limitations:
- “Tandem studies are more often positive than parallel design studies. In a parallel design study, endoscopist bias toward any study arm is mitigated by the clinical and medical-legal demands to protect patients from colorectal cancer in a single withdrawal.”
- “Detection gains for AI are largely for diminutive lesions.3 This is generally true for detection gains from ancillary devices, because powering trials for improved advanced lesion detection is not practical”
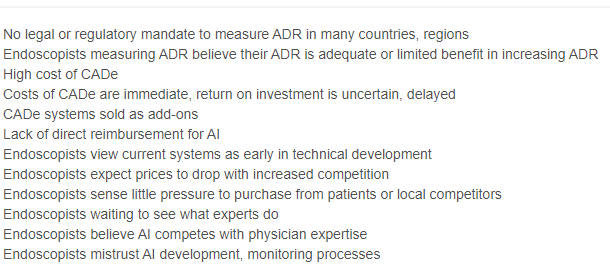
Slow Uptake of AI:
- First, other adjunctive detection devices have received approval from the US Food and Drug Administration and then failed to reach widespread use…the limited adoption of this entire category suggests that physicians attach a relatively low price point to the value of detection gains produced by add-on devices…Incorporating detection devices with add-on cost is particularly problematic in US ambulatory surgery centers.”
- The authors indicate that an endoscopy company could add AI to standard equipment as one way to advance use of this technology
My take: AI will likely improve interpretation and usefulness of colonoscopy, whether for cancer surveillance and other reasons. Cost and familiarity are current barriers to early adoption.
Related blog post: #NASPGHAN19 Impact of New Technologies on Patient Health