S Mckirdy et al. JPGN 2022; 74: 801-804. The Impact of Compliance During Exclusive Enteral Nutrition on Faecal Calprotectin in Children With Crohn Disease
The expression ‘90% of Success is Showing Up’ has been attributed to Woody Allen. With dietary and medical treatments, adherence is the equivalent of showing up.
In this study, the authors measured fecal gluten immunogenic peptides (GIP), a biomarker of gluten intake, in 45 children (3– 17 years) with Crohn’s disease to assess adherence to enteral nutrition. This, in turn, was correlated with fecal calprotectin (FC) levels.
Key findings:
- FC decreased in patients with undetectable GIP at both 33 and 54 days of EEN (mean decrease, 33 days: −743 mg/kg, 54 days: –1043 mg/kg, P< 0.001) but not in patients who had detectable GIP levels
- At EEN completion, patients with undetectable GIP had a lower FC by 717 mg/kg compared with patients with a positive GIP result (P = 0.042) and demonstrated a greater decline from baseline FC (–69% vs +5%, P = 0.011)
- 13% and 23% had detectable GIP levels at 33 days and 54 days respectively. It is noted that GIP levels are only indicative of short-term consumption (eg. prior 1-2 days) of gluten-containing foods
My take: Dietary therapies are really difficult for most people. This study shows that those with poor compliance are unlikely to benefit.
Related blog posts:
- Dietary Therapy for Inflammatory Bowel Disease This is good lecture review on dietary therapy
- Mediterranean Diet vs Specific Carbohydrate Diet for Crohn’s Disease
- Trial by Diet for Pediatric Crohn’s Disease
- Can IBD Be Treated with Diet Alone?
- Good Food and Bad Food for Crohn’s Disease -No Agreement | gutsandgrowth
- Pushing the Boundaries on Dietary Therapy for Crohn’s Disease: CD-TREAT
- Position Paper: Nutrition in Pediatric IBD
- CDED + PEN: An Alternative Diet to Exclusive Enteral Nutrition?
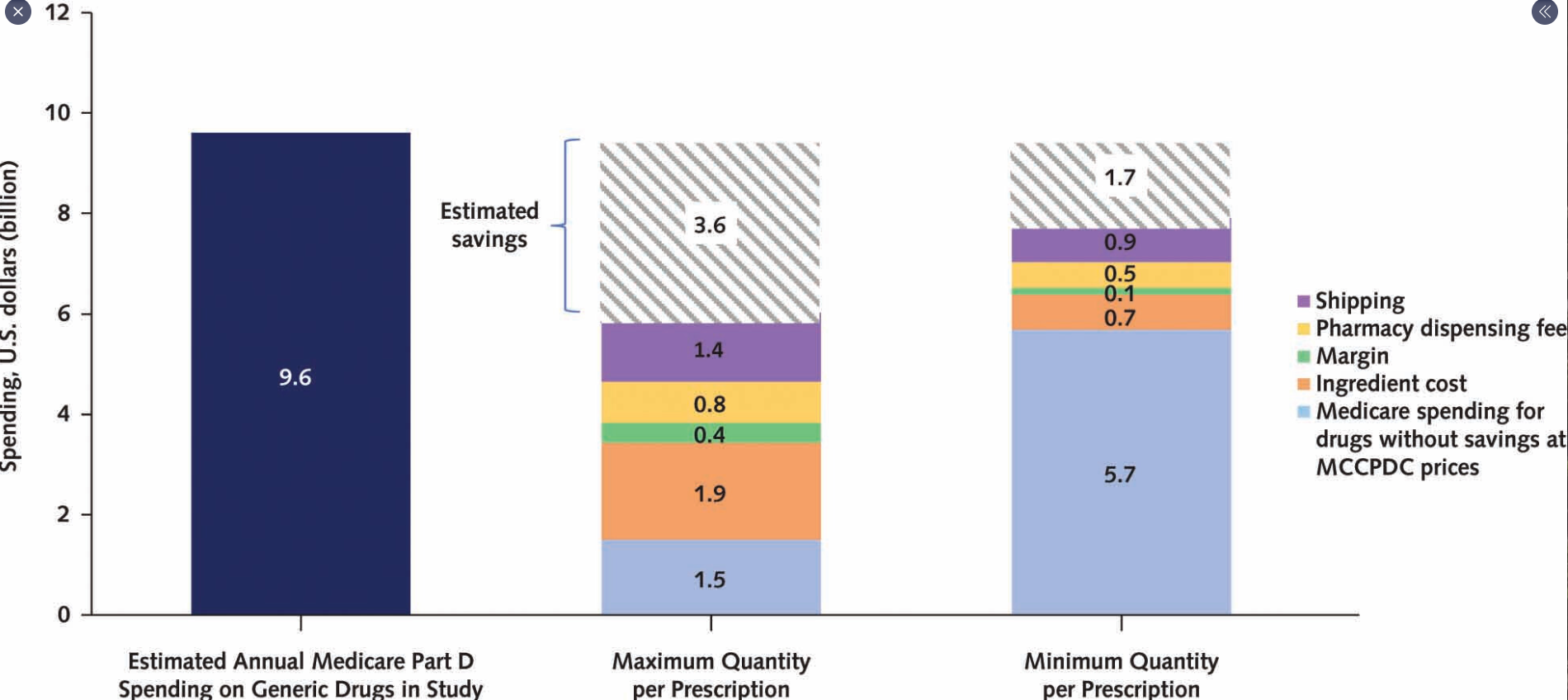
Related blog post: Why I No Longer Need to Be A Billionaire