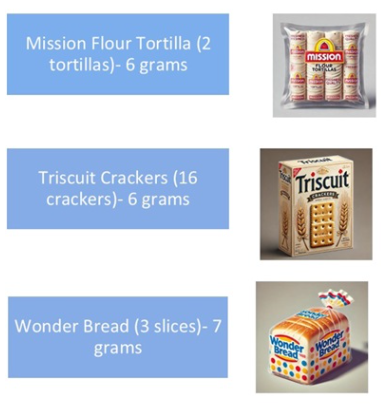
Figure 3 lists the content of several common foods -some noted below
While gluten exposure increases the diagnostic yield of currently available tests, there are novel tests being developed “which may aid in the diagnosis of CeD regardless of diet, with a particular focus on immune-based assays. One such innovation involves the use of tetramer-based assays, which enable the direct detection of gluten-specific T cells in the blood. These tetramers, designed to bind to HLA-DQ2 molecules, can help identify T cells that have been activated by gluten exposure. This presents a highly specific immune marker for CeD. Even for those on a GFD, sensitivity (97%) and specificity (95%) have been impressive.”
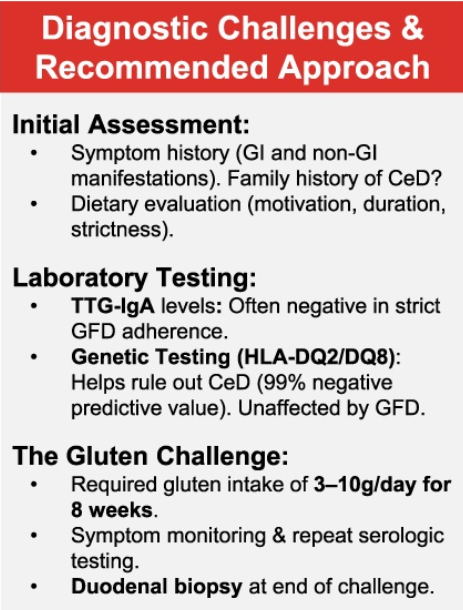
My take: This article provides practical advice for evaluating whether celiac disease is present in those already consuming a GFD.
Briefly noted: The authors present a case report of an adolescent girl post cardiac transplant with hypergammaglobulinemia and presumed celiac disease (CD), who had a persistently elevated anti‐tissue transglutaminase immunoglobulin A despite a gluten free diet. Ultimately, she was diagnosed with polytypic plasmacytosis from suspected immune dysregulation.
Key point:
This case serves as a reminder that when treating those with persistently elevated tTG IgA on a strict GFD, etiologies outside of CD need to be considered.
My take: I had a young girl several years ago who had celiac diagnosis at an outside institution. She had multiple autoimmune disorders. After not responding to treatment, she had a follow-up panendoscopy showing ongoing IELs in duodenum and villous blunting. These findings were noted in the ileum as well. On reviewing her initial biopsies, the pathologist indicated that her findings could be celiac but it was suspected to be an immune dysregulation. Subsequently, she was diagnosed with CTLA4 deficiency and had a marked response to abatacept therapy.
Methods: The researchers conducted a 17‐item Qualtrics survey of patients who participated in intensive multidisciplinary intervention treatment to improve the volume and variety of solid food intake and replace enteral feeding due to chronic food refusal an average of 6 years following intervention. 75 met eligibility criteria; 36 caregivers (48%) completed the survey
Key findings:
Most patients (80%) who achieved full wean from feeding tube dependence at program discharge maintained their wean at the time of the survey
Most caregivers (89%) described their child’s relationship with food as “good” or “neutral”
My take:
Our group works closely with the authors and appreciate all of their help
Survey studies have a lot of limitations and often conclusions are hampered by low participation
It looks like intensive feeding therapy has good durability. It would be interesting if we could know what would have happened to these children without therapy. How many would have gradually improved on their own?
Recently Dr. Bezerra gave our group a terrific lecture. I have taken some notes and shared some of his slides. There may be inadvertent omissions and mistakes in my notes. In addition, Dr. Bezerra’s presentation included several lengthy animations which helped explain the basic science concepts. These are not included in this summary.
Prior to his presentation to our group, Dr. Bezerra’s accomplishments had been recognized with the Shwachman Award, the highest honor bestowed by our national pediatric GI organization NASPGHAN (NASPGHAN Awards 2025). On a personal note, Jorge was the first person to give me hands-on instruction with an endoscope and I have a great deal of admiration for his humility, thoughtfulness and scientific achievements.
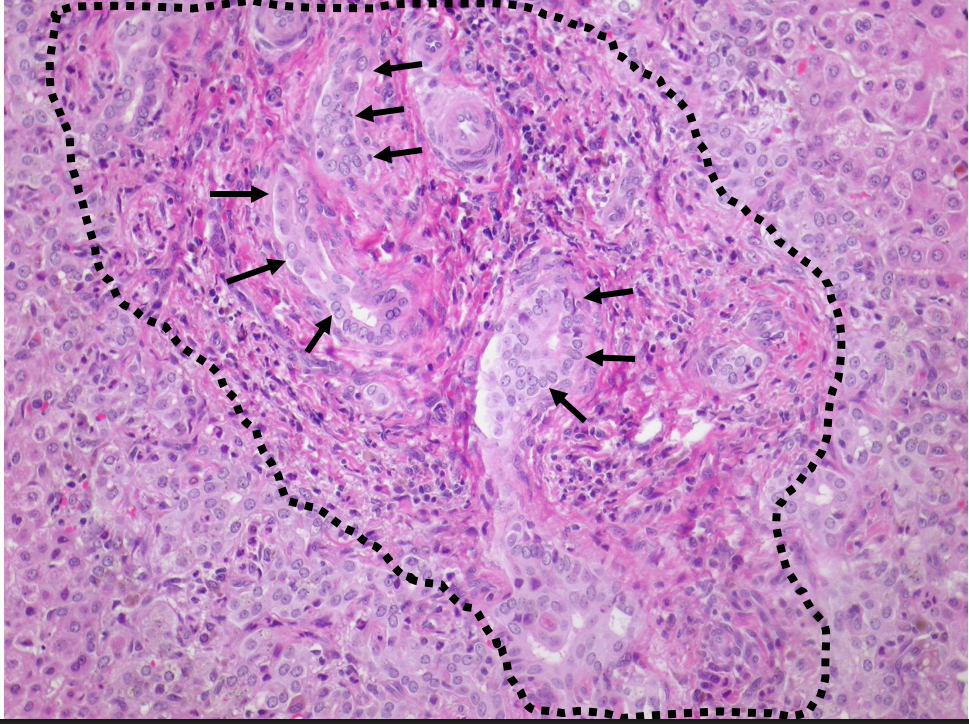
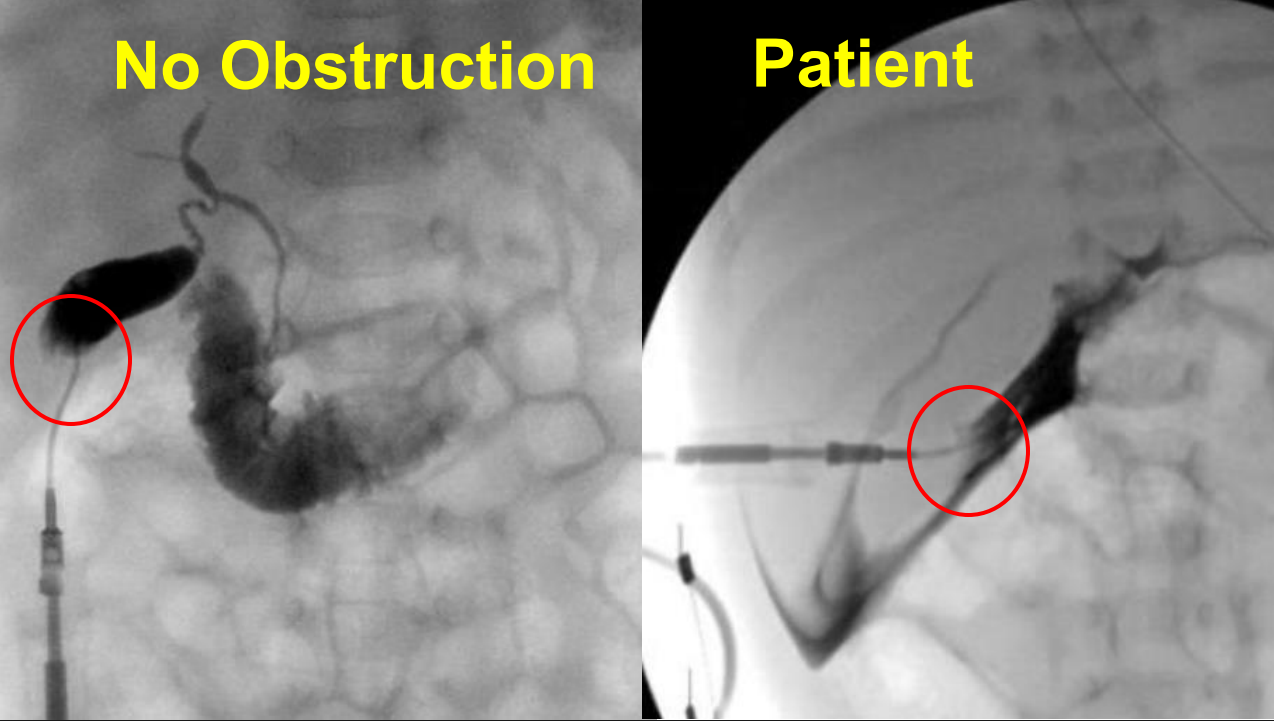
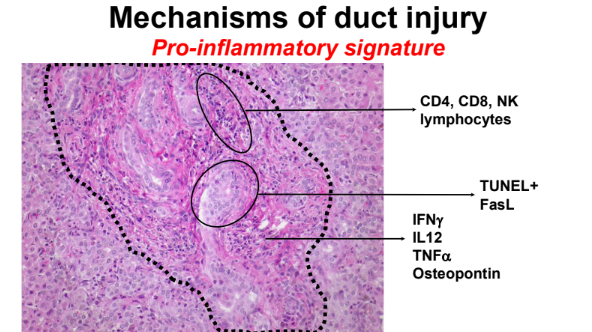
Liver biopsy from patient with BA showing bile duct proliferation .Operative cholangiograms from a patient with normal anatomy and one with BA that shows contrast extravasation without patent biliary tract
Key points:
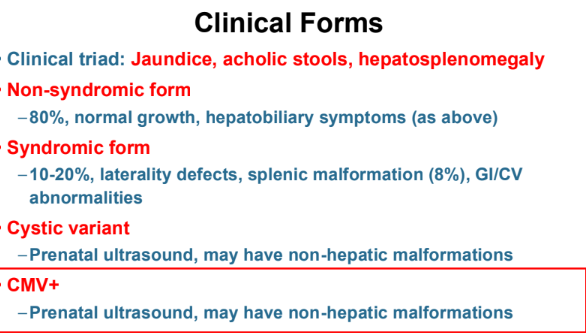
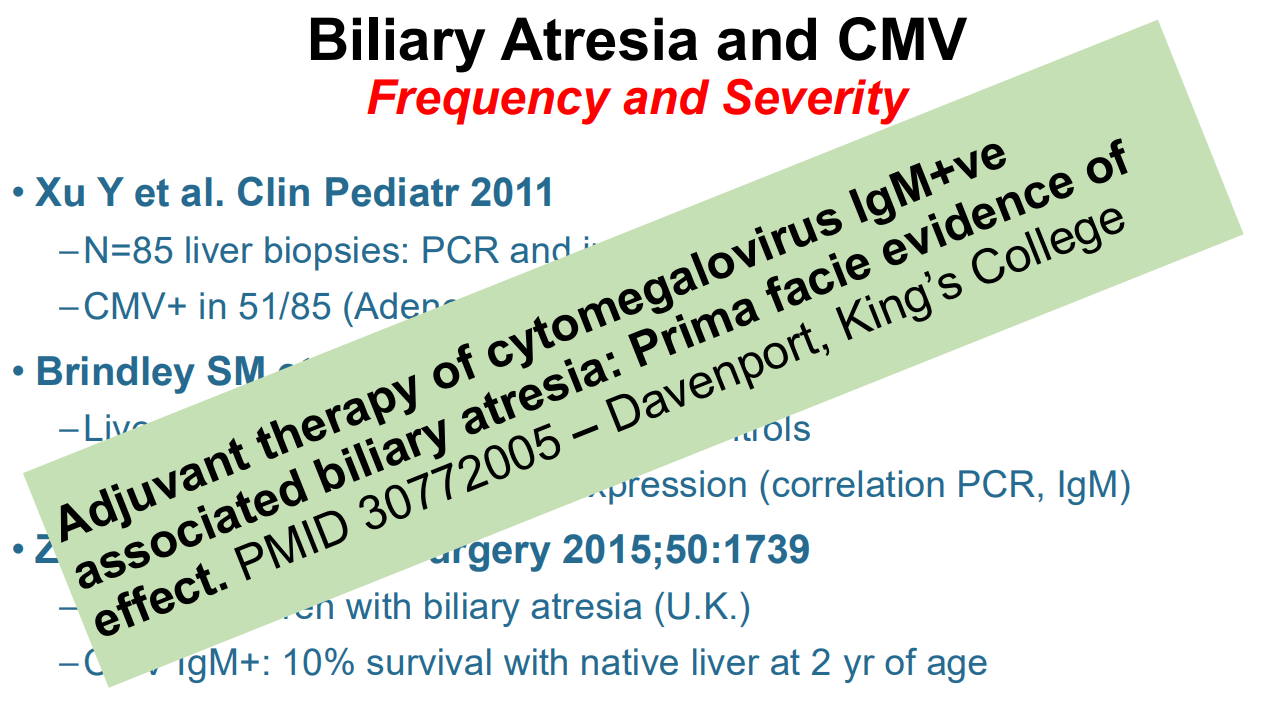
Cytomegalovirus (CMV) is frequently associated with biliary atresia (BA). Treatment of CMV when detected may improve outcomes
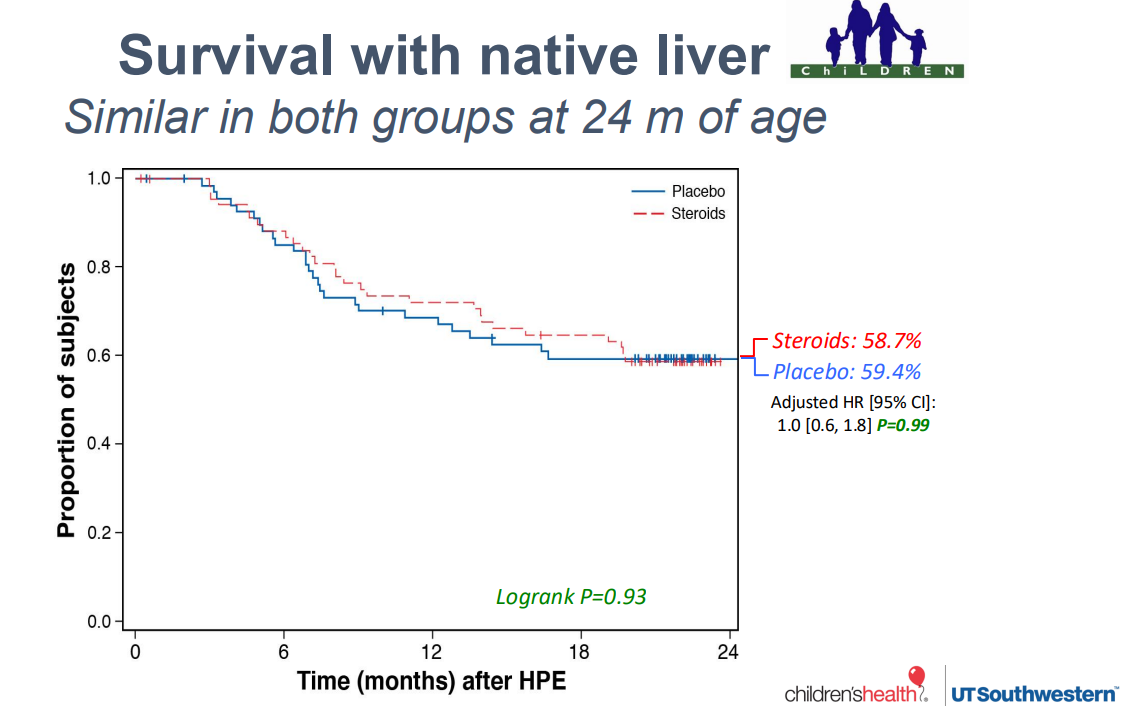
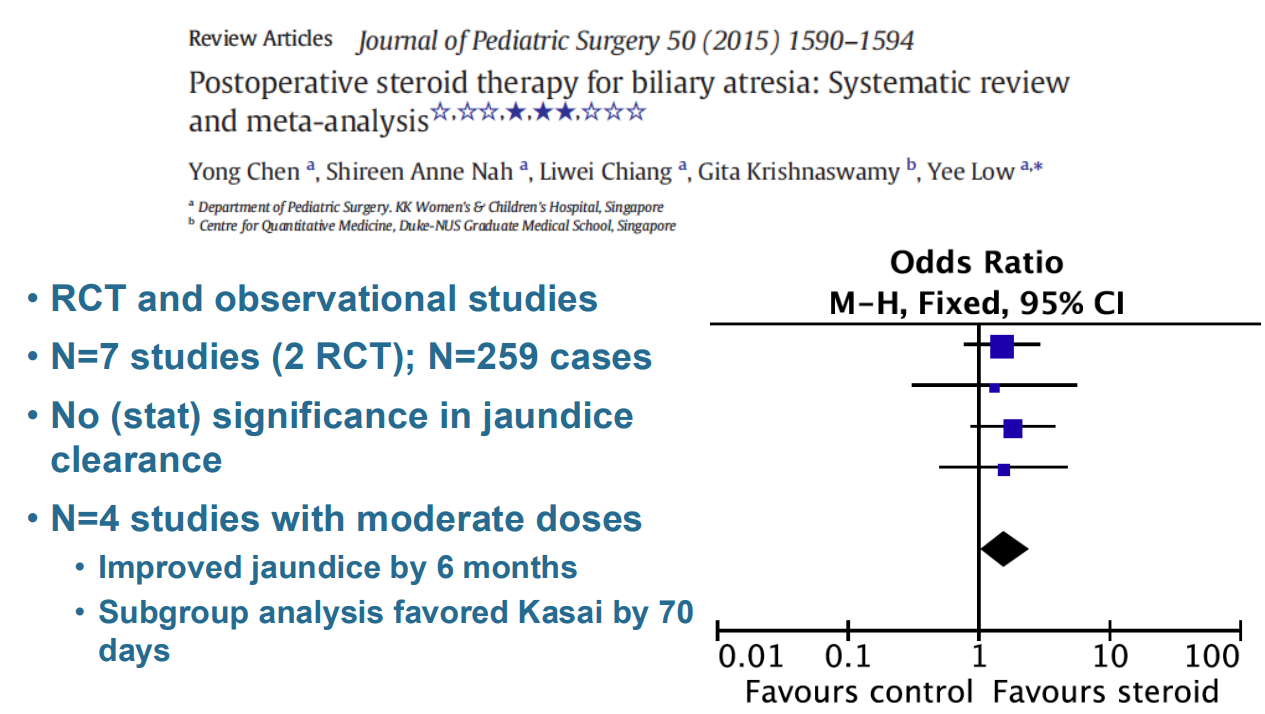
Hepatoportoenterostomy (HPE) (aka Kasai procedure) is effective in about half of patients. The remainder develop complications that include recurrent cholangitis, portal hypertension, and cirrhosis which may lead to the need for liver transplantation
10-year survival rates for liver transplantation are >85%.
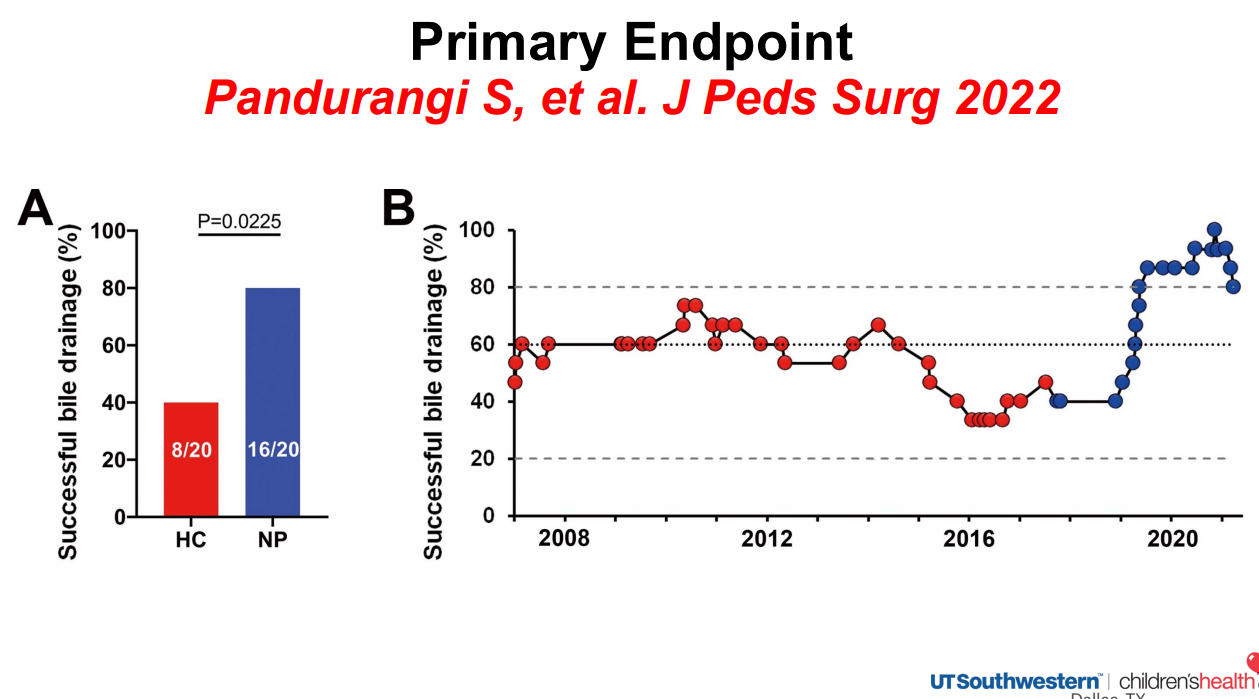
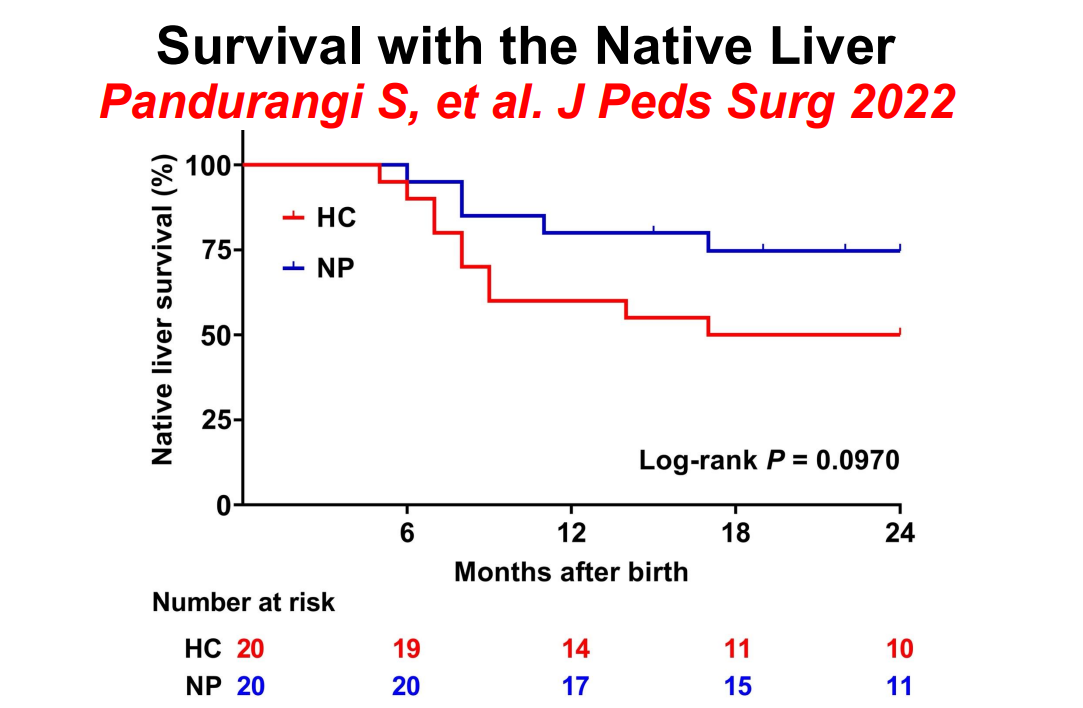
Historical controls in red and new protocol in blue
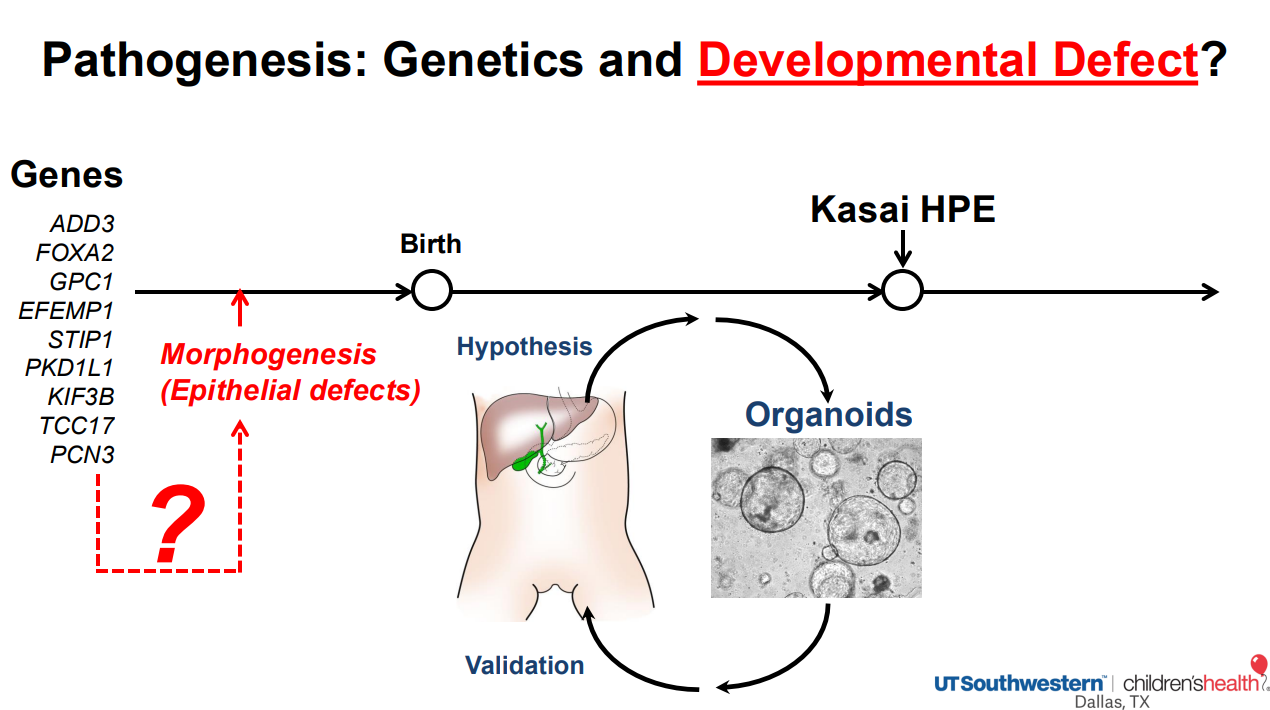
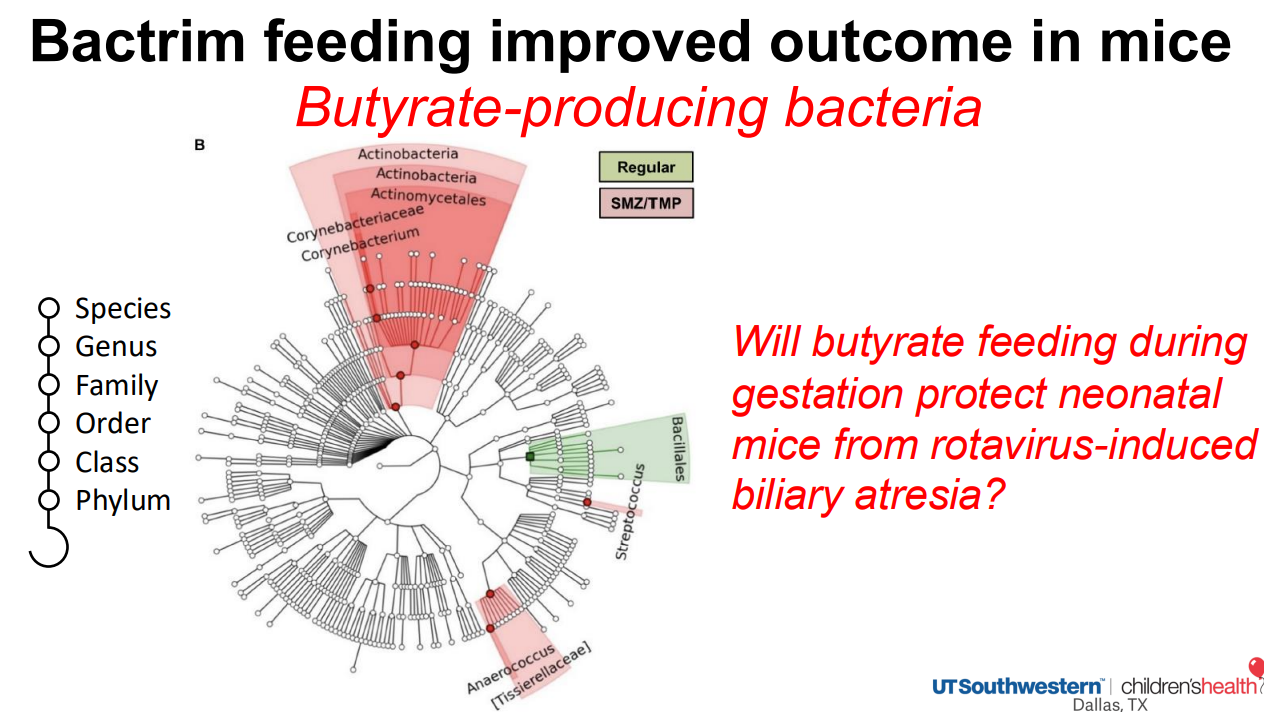
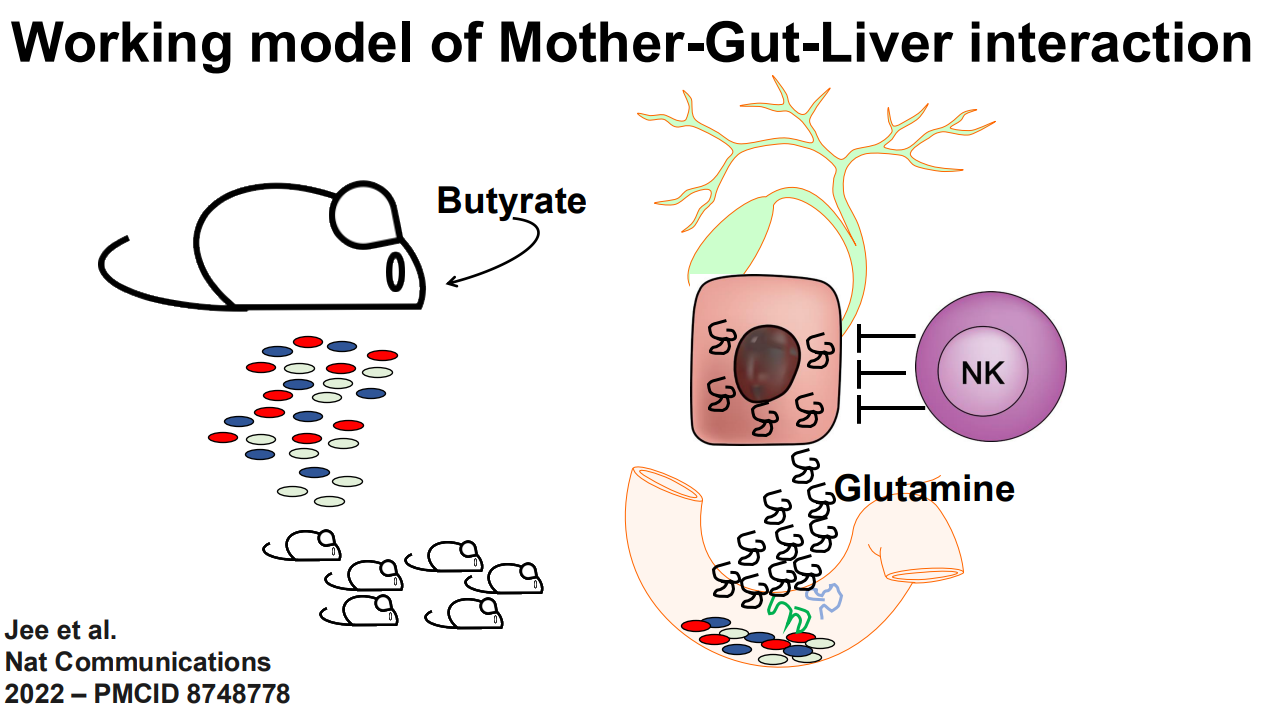
The role of the microbiome is being explored as a factor in the predisposition to BA
Biliary atresia organoid studies: Biliary atresia organoids had decreased expression of genes related to EGF signaling and FGF2 signaling. When treated with EGF+FGF2, biliary atresia organoids expressed differentiation markers, which restored polarity (Reference: Hepatology 2022 Jan;75(1):89-103. doi: 10.1002/hep.32107. Biliary organoids uncover delayed epithelial development and barrier function in biliary atresia). Thus, these organoids can help understand the underlying pathogenesis and may lead to improved treatments
More recently, compared to normal liver organoids, the epithelium of BA organoids was fragmented and peribiliary glands (PBGs) were small, had abnormal intercellular junction (ZO1 expression), and expressed markers of epithelial-mesenchymal transition (EMT), with a prominent expression of TGF-β3. Upon TGF-β inhibition, EMT decreased in the diseased epithelium, the population of PBGs increased, and ZO1 expression improved. In vivo, TGF-β inhibition suppressed the BA phenotype and substantially decreased liver fibrosis in neonatal mice. Thus, the modulation of TGF-β-dependent EMT regulates bile duct epithelial development and influences the susceptibility of neonates to biliary injuries. (Reference: Nat Commun 2025 Jul 17;16:6575. doi: 10.1038/s41467-025-61442-5. Open Access! Cellular crosstalk mediated by TGF-β drives epithelial-mesenchymal transition in patient-derived multi-compartment biliary organoids)
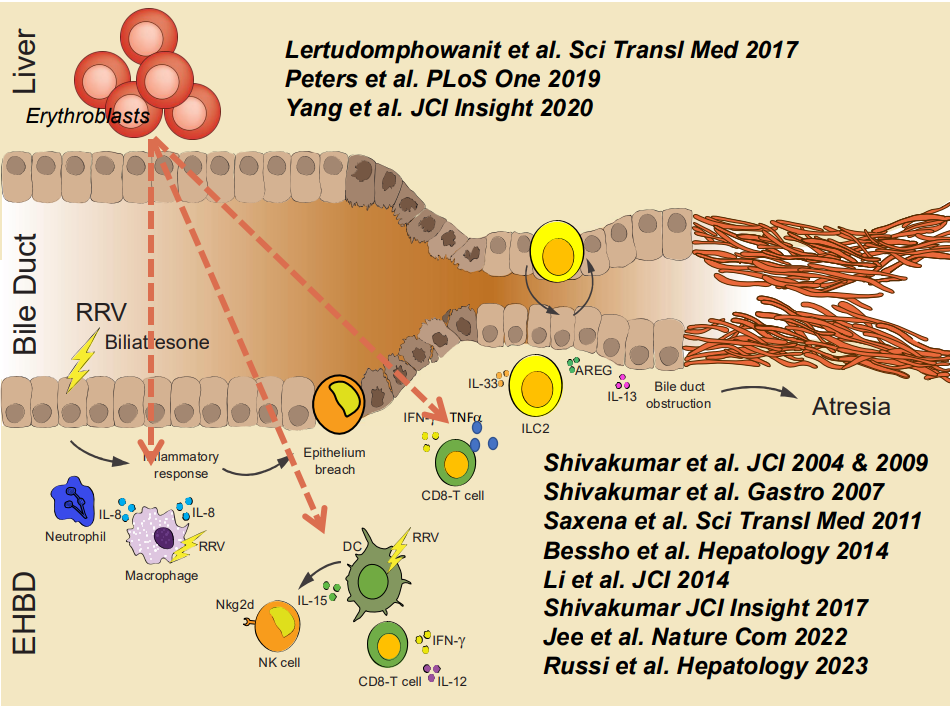
RRV (rhesus rotavirus) can create an experimental model of BA in the mouse. In this mouse model, ILC2 cells (innate lymphoid cells in yellow) play a role in bile duct proliferation, possible attempt at recanalizing damaged bile ducts
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition
Methods: This was a retrospective review of records of children (n=54, median age 9 years) who underwent MRI of spine between January 2021 and December 2023 for evaluation of refractory constipation (RC). RC was defined as constipation not responding to optimal conventional treatment for at least 3 months. Conventional treatment included—education, disimpaction (if required), osmotic and stimulant laxatives, timed‐toileting and biofeedback.
Key findings:
Thirteen children (24%) had an abnormal MRI. Findings included—syringomyelia‐8,sacral canal meningeal cyst‐2, filum terminale lipoma‐1,spina bifida occulta‐1 (SBO‐1), and Schmorl’s node‐1. None of these patients had a tethered cord
Only one patient with a Chiari malformation and syrinx required a neurosurgical intervention. The surgery did not improve his constipation
On a median follow‐up duration of 677 (range181–1240) days, constipation resolved in 48% (n = 26) of the entire cohort
There was no difference in the number of patients or time to constipation resolution between those with and without abnormal MRI respectively
My take: In children with refractory constipation who do not have abnormal cutaneous/abnormal neurological exam, an MRI is unlikely to be helpful.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition
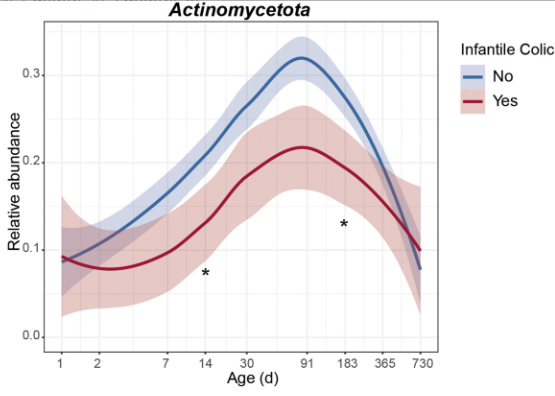
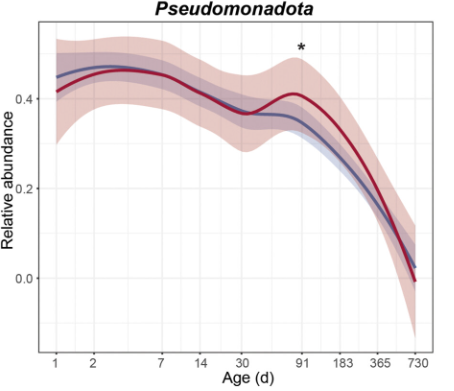
E Van Daele et al.J Pediatr Gastroenterol Nutr. 2025;81:217–225. Aberrant microbiota signatures precede symptomdevelopment in infantile colic
My take: There has been an interest in altered microbiome and colic for a long time. Whether these alterations are causally-related to colic and whether there is a way to treat these alterations remains unclear.
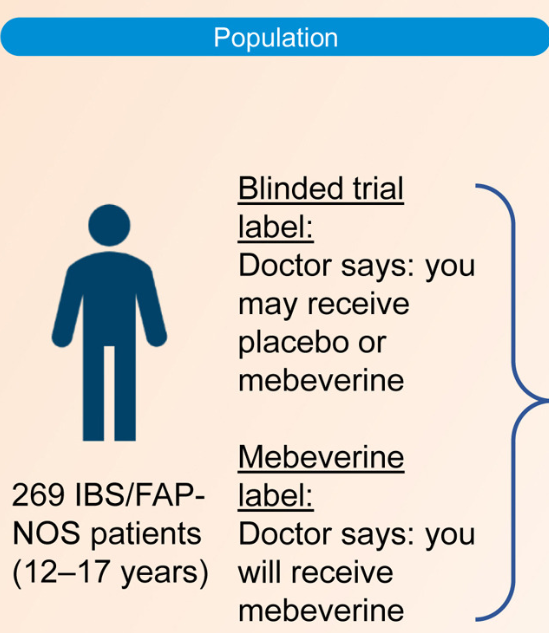
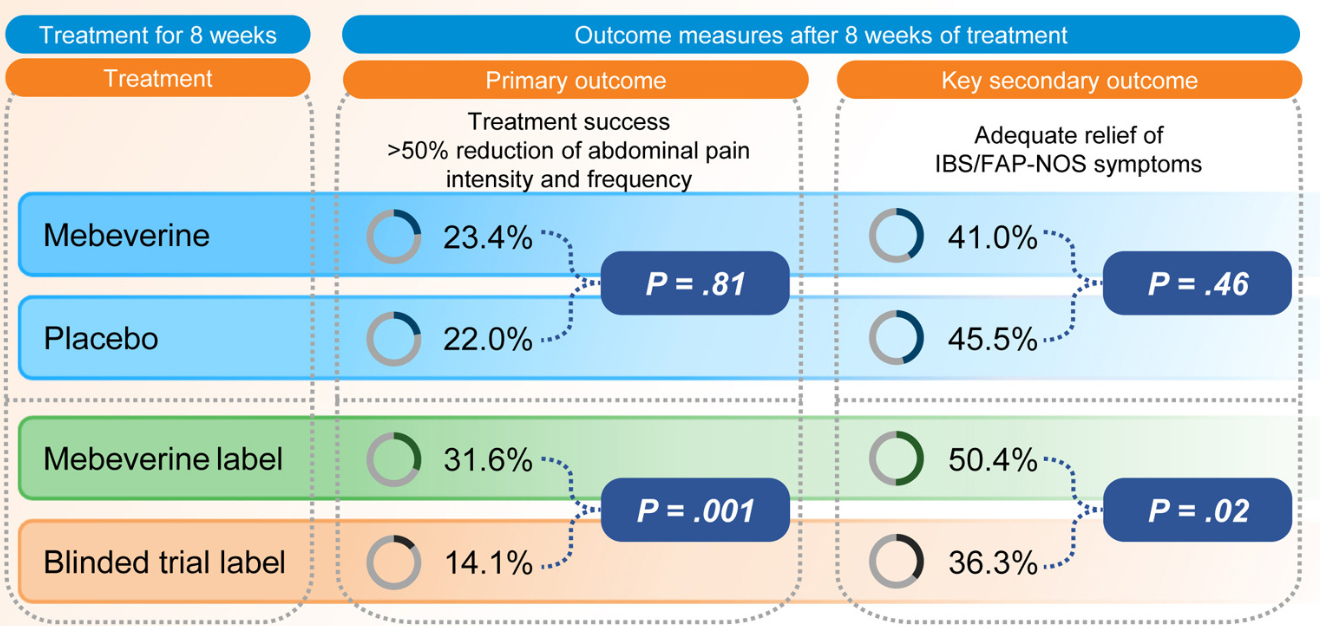
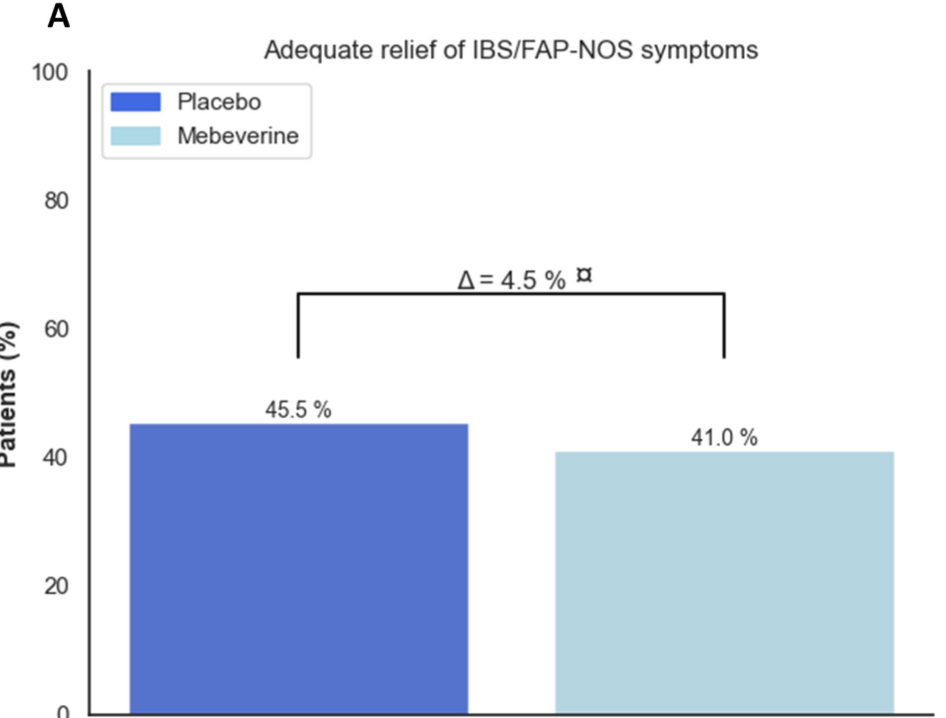
Methods: This was a randomized trial with 12-17 yr olds with irritable bowel syndrome or functional abdominal pain who received mebeverine (200 mg twice daily) or placebo for 8 weeks. Treatment was labeled as “mebeverine or placebo” (blinded trial label) or “mebeverine” (mebeverine label), creating the following 4 groups: (1) mebeverine-blinded trial label, (2) mebeverine-mebeverine label, (3) placebo-blinded trial label, and (4) placebo-mebeverine label. Randomization (1:1:1:1) was masked to physicians, except for drug labeling. Primary end point was treatment success (>50% reduction of abdominal pain intensity and frequency) after 8 weeks. The key secondary end point was adequate relief of symptoms.
Key findings:
Blinded Trial Label: Treatment success was similar between those receiving mebeverine (groups 1 and 2) (n = 31 [23.4%]) and placebo (groups 3 and 4) (n = 30 [22.0%]; odds ratio [OR], 1.08
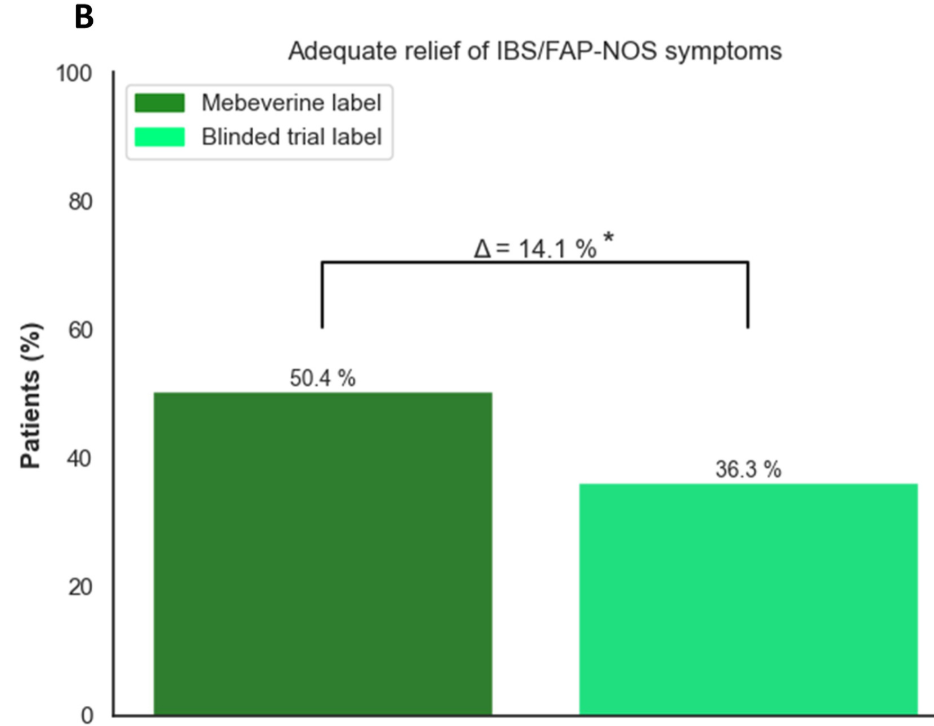
Effect of Being Informed of Treatment with Active Medication: Treatment success was higher in groups with the mebeverine label (groups 2 and 4) (n = 42 [31.6%]) compared with the blinded trial label (groups 1 and 3) (n = 19 [14.1%]; OR, 2.84
Discussion Points:
“This is the first study evaluating the impact of positive labeling on pain in a pediatric population. Our findings of a doubled treatment effect rate (32.9% vs 15.1%) when children were told they were receiving the active drug, are in line with adult studies showing higher pain reduction with positive labeling..14,19 It underscores the importance of positive expectations in pain management, which operates via multiple mechanisms.”
“Results of previous research has shown that children with IBS can also report symptom relief when they know that they are receiving an inert compound, known as an ‘“’open-label placebo.’22“
“Ethical norms state that ‘“’the use of a placebo without the patient’s knowledge may undermine trust, compromise patient–physician relationship, and result in medical harm to the patient.’26“
My take: This is a fascinating study showing how expectations for treatment can enhance the placebo effect. While the authors and the associated editorial mull over the ethical issues regarding deception of giving placebo without the family’s knowledge, in clinical practice many of the current drugs (eg. antispasmotics, neuromodulators, probiotics) have uncertain benefit and can be given without concern for deception.
Related blog posts:
Good Study, Bad Practice: Placebo for IBS and Functional Abdominal Pain “It is a mistake to consider placebo as a treatment for functional abdominal pain. In many children, pain fluctuates and may improve with reassurance, distraction, healthier diets, and physical activity. However, we also need more effective therapies including pain psychology, dietary approaches and medications. The idea that placebo helps is misleading and undermines the fact that patients with functional disorders need effective treatment.”
A Upton et al. J Pediatr Gastroenterol Nutr. 2025;81:204–211. An ultrasound approach to visualize the “duct at the hilum” in infants undergoing evaluation for biliary atresia
Methods: Ultrasound exams were reviewed from infants undergoing evaluation for biliary atresia at Texas Children’s Hospital during two periods. First, exams performed before 2021 were reviewed to develop a systematic approach to visualize the duct at the hilum (DaH). Second, exams performed during a subsequent 26-month period were reviewed to assess the approach’s diagnostic performance in 64 infants (mean age 25 days).
Key findings:
The approach identified all 12 patients with biliary atresia and excluded 49 out of 52 infants without biliary atresia, for a sensitivity of 1.00 and specificity of 0.94.
There were three false-positive studies (i.e., the DaH was absent, but diagnosis was not BA) in infants with choledochal cyst, Trisomy 18, and an aberrant main portal vein (which interfered with the US examination),
The approach could be performed in feeding infants and often in <5 min.
Discussion:
“First, the DaH was easier to identify when infants were allowed to feed. In some cases, a DaH could be seen in fasting images but was longer and more prominent in subsequent non-fasting images”
“Tthe approach had high sensitivity and could efficiently rule out infants who did not have biliary atresia”
“We have not determined the precise segment of the extrahepatic biliary tree visualized by our approach; however, in contrast to previous reports, we do not think the approach is imaging the “common bile duct.” Rather, the DaH is a segment closer to the liver and could be the common hepatic duct.”
“Larger, multisite studies are needed…we may have overestimated sensitivity because the 12 infants with biliary atresia were all categorized as Japanese Biliary Atresia Society classification Type II or III…Similarly, we may have overestimated specificity because all ultrasound exams were performed by 1 sonographer with 10+ years of experience.”
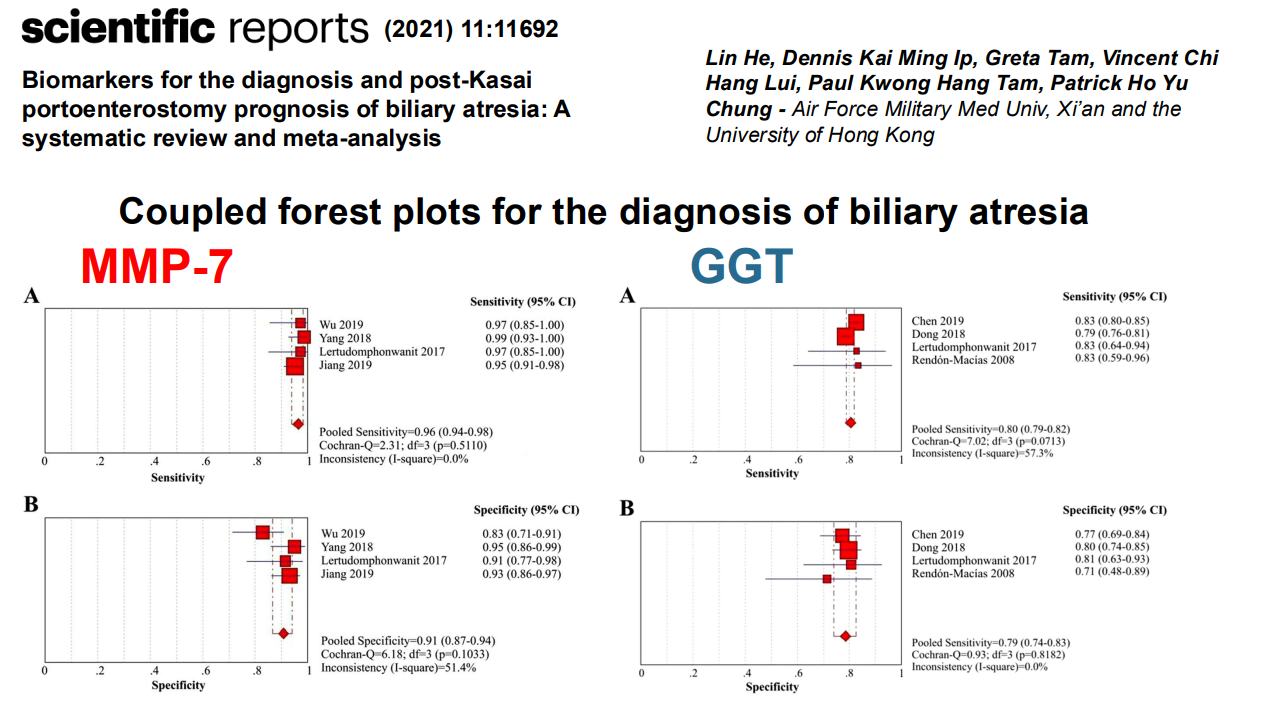
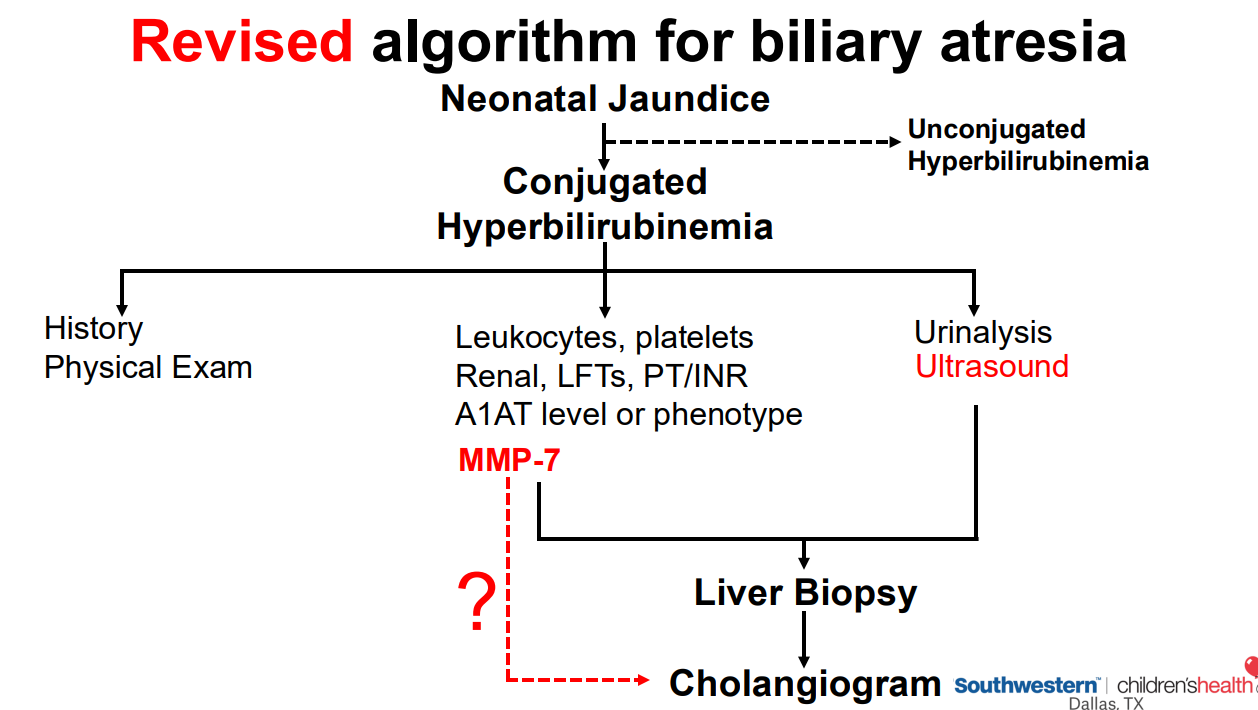
My take: It does seem that the presence of biliary atresia should be identifiable with ultrasound. However, this likely relies on the skills of the ultrasonographer, especially given the small size of these patients. Thus far, in clinical practice, an ultrasound has been mainly helpful at excluding choledochal cysts/anatomic malformations. A tiny or contracted gallbladder (with fasting) does increase the likelihood of biliary atresia. In my experience, other ultrasound findings like the ‘triangular cord’ sign are less helpful than serum matrix metalloproteinase 7 (MMP-7) tests.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition
Mehtods: This international, multicenter, retrospective cohort study consecutively enrolled JAK-inhibitor-treated patients with IBD who subsequently developed acne (aka JAKne).
Key findings:
Among 2183 JAK inhibitor–treated patients with IBD, 272 developed acne
70% of acne cases occurred within the first 3 months of treatment initiation
The crude prevalence rates of acne were 15.9% for upadacitinib, 4.3% for tofacitinib, and 1.9% for filgotinib, with dose-dependent relationships observed for upadacitinib and tofacitinib
Most cases were mild-moderate in severity. Mild (<10% of body surface area) was noted in 68%, Moderate (10-30% of BSA) was noted in 24%, and Severe (>30% of BSA) was note in 8%
Among those who developed acne, areas that were affected included the face in 89%, the back in 33%, the chest in 27% and the scalp in 1%
40% received pharmacologic intervention
18% of patients who developed acne had JAK inhibitor dose reduction or discontinuation
My take: JAKne is a common adverse effect. Early identification, proactive counseling, and timely interventions, such as dose reduction, acne therapies or referral to dermatology, are crucial in managing this side effect.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.