Related blog posts:

L Berman et al. Pediatrics 2022; 149 (6): e2021055213. Gastrostomy Tube Use in Pediatrics: A Systematic Review
This lengthy review (27 pages) authored by a multispecialty team makes 17 graded recommendations regarding gastrostomy tubes/gastrostomy tube (GT) placement. The authors state that this review was based on nearly 900 publications with 58 influencing final recommendations.
Here are several of them:
Elaborating on these recommendations::
My take: This article’s recommendations need to be carefully considered by pediatric gastroenterologists along with pediatric surgeons and interventional radiologists.
Related blog posts:
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.


CMA de Bruijn et al. J Pediatr 2022; 244: 107-114. Open Access: Development of a Bowel Management Scoring Tool in Pediatric Patients with Constipation
This report describes the “newly developed and validated PBMST (Pediatric Bowel Management Scoring Tool) is a reliable tool for evaluating bowel management strategies in children with constipation.”
Key finding:
“This study shows that use of the PBMST (see below) can better guide management of childhood constipation, with its fair reproducibility indicating that it is stable over a specified time period. Indeed, consistent use of the PBMST can objectify the patient’s clinical condition over a longer period. Consequently, the score provides feedback regarding the effect of the applied bowel management strategy for each individual patient.”
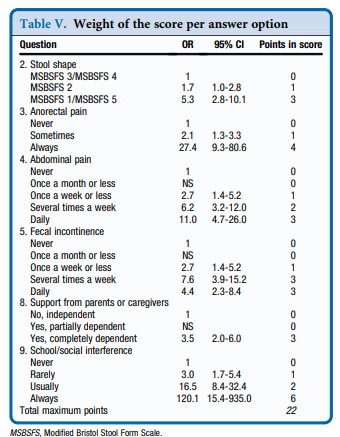
My take: 6 key questions for constipation visits: stool form, anorectal pain, abdominal pain, soiling, support from parents, and social limitations.
Related blog posts:
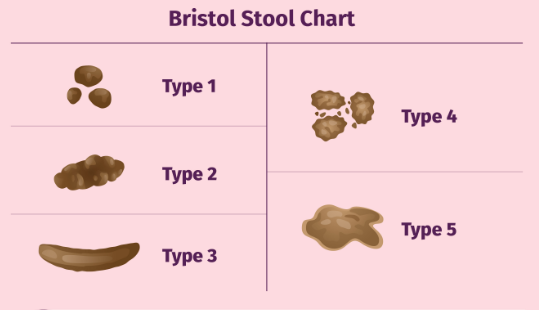
Modified Bristol Stool Form (see link: CAM Wegh et al. JPGN 2021; 73: 210-216. The Modified Bristol Stool Form Scale: A Reliable and Valid Tool to Score Stool Consistency in Dutch (Non)Toilet-trained Toddlers)
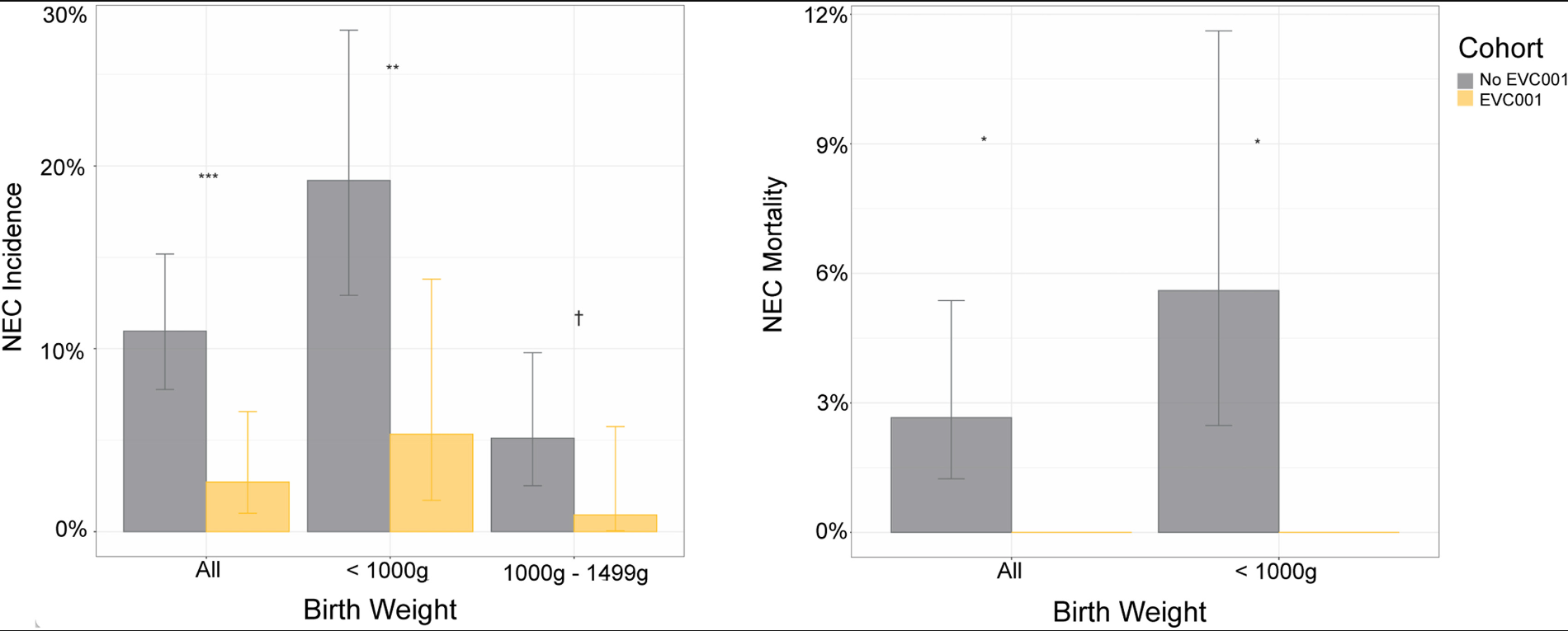
J Tobias et al. J Pediatr 2022; 244; 64-71. Open Access: Bifidobacterium longum subsp. infantis EVC001 Administration Is Associated with a Significant Reduction in the Incidence of Necrotizing Enterocolitis in Very Low Birth Weight Infants
Editorial: MA Underwood J Pediatr 2022; 64: 14-16. Open Access: Bifidobacterium infantis, Necrotizing Enterocolitis, Death, and the Role of Parents in the Neonatal Intensive Care Unit
Methods: Nonconcurrent retrospective analysis of 2 cohorts of 483 very low birth weight (VLBW) infants not exposed and exposed to B infantis EVC001 probiotic at Oregon Health & Science University from 2014 to 2020
Key findings:
Key points from editorial:
My take: It is hard to understand that, despite 20 years of research showing probiotics can reduce mortality and morbidity in premature infants, we have not been able to manufacture a consistent, reliable high-quality probiotic capable of meeting FDA standards.
J Strauss et al. JPGN 2022; 74: 776-781. Mechanical Complications in Central Lines Using Taurolidine Versus Ethanol Lock Therapy in Children With Intestinal Failure
This retrospective study with 13 patients (10,187 catheter days [CDs]) compared ethanol locks (EL) with taurolidine locks (TL). Taurolidine is a “non-toxic, broad-spectrum antimicrobial” with growing use outside the U.S. Manufacturing issues still need to be addressed to gain FDA approval. Link: CORMEDIX RECEIVES COMPLETE RESPONSE LETTER FROM FDA FOR DEFENCATH™ CATHETER LOCK SOLUTION
Key findings from this study:
My take: Taurolidine, when available in U.S., may be a suitable alternative to ethanol, when available in U.S., in preventing CRBSI. In addition, taurolidine locks appear to have fewer mechanical risks.
Related blog posts:

This weekend, on “Wait, Wait, Don’t Tell Me” (Transcript July 2) on their ‘Bluff the Listener’ game, they highlighted three stories of a new Philadelphia tourist attraction. The true (very funny) story was regarding “The Relief Room.” A bathroom (suitably) dedicated to Philadelphia pitcher relievers and covered in memorabilia.
GONDELMAN: 45-year-old Matt Edwards, has gone above and beyond turning his home’s downstairs bathroom into a monument to his beloved Phillies.
GONDELMAN: The Relief Room, as Edwards calls the commode, is a celebration of retired Phillies relief pitchers.
GONDELMAN: Though the room is jampacked with Phillies ephemera, such as signed photographs and figurines, the area above the toilet remains largely empty. That’s because it’s reserved especially for pitchers who have played for Phillies championship teams.
GONDELMAN: Edwards did miss an opportunity for guests to declare their need for personal relief the same way that catchers deliver signals to a pitcher – throw down one finger if you need to do what the Phillies do with a late-inning lead…
GONDELMAN: …Two fingers if you need to do what the team is playing like overall.
Here’s a link to a very descriptive NY Times article/pictures: When Nature Calls, Phillies Relievers Have a Place to Go

W-Q He, GN Guo, C Li. Hepatology 2022; 75: 1566-1578. The impact of hepatitis B vaccination in the United States, 1999-2018
In the past 30 years, the hepatitis B vaccine has been included in infant immunization schedules in the U.S. The authors studied a large, comprehensive, and nationally representative data set (NHANES data from 1999-2018) to assess its efficacy.
Key findings:
Context for these findings is noted in the associated editorial (pgs 1365-1367):
HBV remains one of the most deadly viruses worldwide with nearly 1 million deaths yearly and nearly 300 million people chronically-infected. The vast majority of unvaccinated children less than 1 year of age become chronically-infected. In the U.S., 98% of children acquired HBV through vertical transmission “including 26% of pediatric cases who were born in the USA or Canada”
My take: This study shows that HBV vaccine maintains strong protection for 20 years and protects against cancer and death.
Related blog posts:


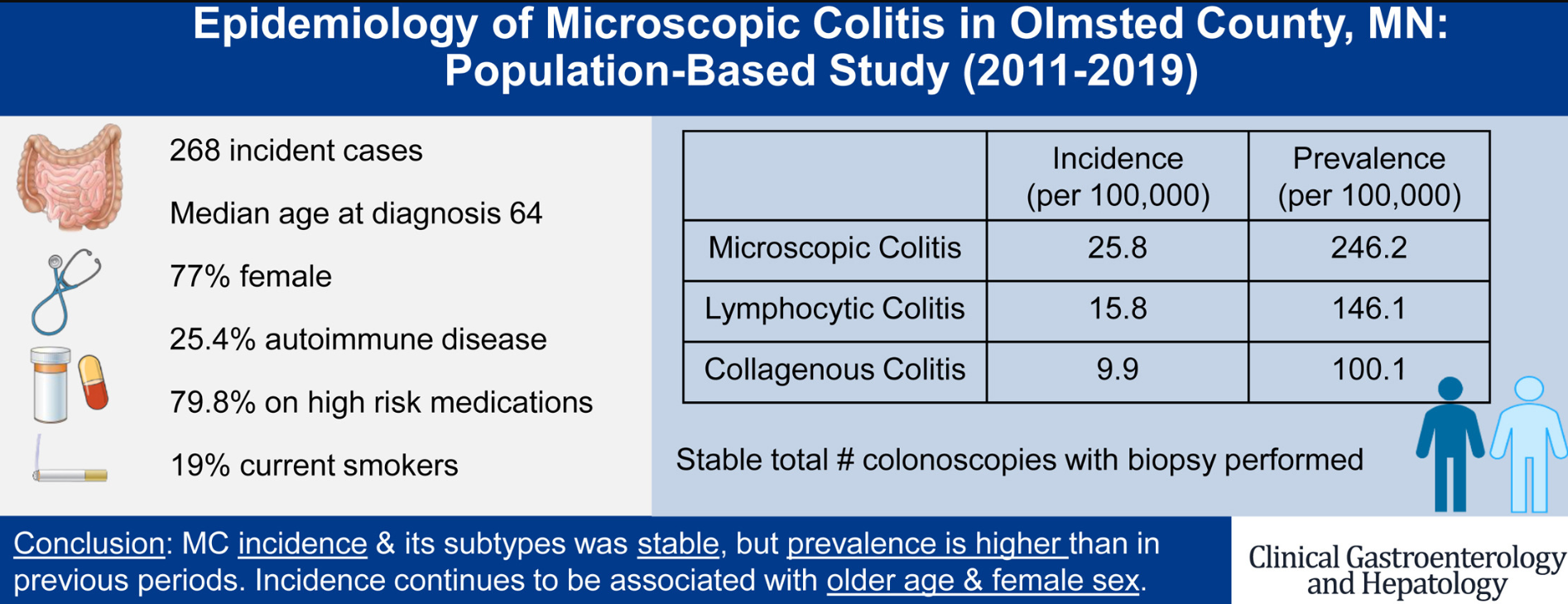
J Tome et al. Clin Gastroenterol Hepatol 2022; 20: 1085-1094. Open Access: The Epidemiology of Microscopic Colitis in Olmsted County, Minnesota: Population-Based Study From 2011 to 2019
Key points:
Related blog post/related article:
BK Burton et al. JPGN 2022; 74: 757-764. Open Access: Long-Term Sebelipase Alfa Treatment in Children and Adults With Lysosomal Acid Lipase Deficiency
This was open-label study of enzyme replacement therapy (ERT) in 31 children and adults with lysosomal acid lipase deficiency (LALD). Sebelipase Alfa, a recombinant human lysosomal acid lipase, was FDA approved in 2015 for LALD.
Key findings:
In the associated commentary (pgs 726-727), the authors state this study showed that “in contrast to infantile disease, ERT is not universally beneficial in individuals with attenuated disease…[and] it is impossible to predict response to ERT.” Testing for LALD is recommended for infants with hepatomegaly, poor growth, diarrhea or adrenal insufficiency. In older groups, LALD needs to be considered in those with hepatomegaly, steatosis, and dyslipidemia.
My take: There are still many questions regarding ERT’s long-term benefit in individuals with LALD, especially those with mild disease.
Related blog posts:
S Mckirdy et al. JPGN 2022; 74: 801-804. The Impact of Compliance During Exclusive Enteral Nutrition on Faecal Calprotectin in Children With Crohn Disease
The expression ‘90% of Success is Showing Up’ has been attributed to Woody Allen. With dietary and medical treatments, adherence is the equivalent of showing up.
In this study, the authors measured fecal gluten immunogenic peptides (GIP), a biomarker of gluten intake, in 45 children (3– 17 years) with Crohn’s disease to assess adherence to enteral nutrition. This, in turn, was correlated with fecal calprotectin (FC) levels.
Key findings:
My take: Dietary therapies are really difficult for most people. This study shows that those with poor compliance are unlikely to benefit.
Related blog posts:
Related blog post: Why I No Longer Need to Be A Billionaire
