Preoperative TNFi exposure was not associated with postoperative infectious complications in a large prospective multicenter cohort. Any infection (18.1% vs 20.2%, P = .469) and SSI (12.0% vs 12.6%, P = .889) rates were similar in patients currently exposed to TNFis and those unexposed.
This lengthy review (27 pages) authored by a multispecialty team makes 17 graded recommendations regarding gastrostomy tubes/gastrostomy tube (GT) placement. The authors state that this review was based on nearly 900 publications with 58 influencing final recommendations.
Here are several of them:
Trial of home nasogastric feeding is safe and should be strongly considered before GT placement, especially for patients who are likely to learn to eat by mouth
Routine contrast studies are not indicated before gastrostomy placement
Laparoscopic placement is associated with the best safety profile
For most patients, a low-profile balloon GT is preferred
Elaborating on these recommendations::
Home NG: The authors note that Lagatta et al found that infants sent home with NG from nursery had shorter length of stay and fewer readmissions/emergency encounters than patient sent home with GT. However, this statement ignores the significant differences in the patient characteristics in the two groups noted in this article (see related blog post: Impact of NG Feeding Program for NICU Graduates). Interestingly, many of the return visits are due to dislodgements of button GTs.
Preoperative workup: While the authors discourage use of preoperative UGI and except in patients not achieving adequate enteral nutrition due to emesis, they also recommend “GT should only be pursued after appropriate workup has been performed to investigate the underlying medical diagnosis.” I find this vague recommendation to be problematic. Shortly before making this recommendation, the authors state “proper identification and management of the underlying diagnosis (eg. diet modification for eosinophilic esophagitis) may obviate the need for GT placement.” So, do the authors want every child who may need a GT to undergo an EGD? Or perhaps even more, such as an MRI or full exome sequencing? Also, which diet trial do they recommend for potential eosinophilic esophagitis -does this mean an amino acid based formula or is a hydrolysate sufficient?
GT technique: The review of the techniques of GT placement cite data comparing the techniques and complication rates (though noting critical risk of bias in these studies):
open gastrostomy (n=1471) vs PEG (n=679): 3.2% vs 4.1% (P=.35)
laparoscopic gastrostomy (n=787) vs PEG (n=1321) 1.2% vs 5.4% (P<.0001)
IR placement (n=321) vs PEG (n=417): 3.7% vs 1.9% (P=.04)
the authors note the decision needs to consider specific patient characteristics and institutional factors
My take: This article’s recommendations need to be carefully considered by pediatric gastroenterologists along with pediatric surgeons and interventional radiologists.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Lavender field (off season) at Poblanos Ranch, Albuquerque
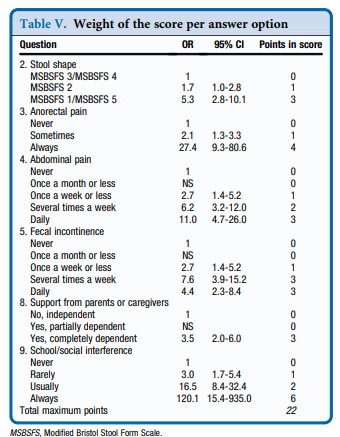
This report describes the “newly developed and validated PBMST (Pediatric Bowel Management Scoring Tool) is a reliable tool for evaluating bowel management strategies in children with constipation.”
Key finding:
“This study shows that use of the PBMST (see below) can better guide management of childhood constipation, with its fair reproducibility indicating that it is stable over a specified time period. Indeed, consistent use of the PBMST can objectify the patient’s clinical condition over a longer period. Consequently, the score provides feedback regarding the effect of the applied bowel management strategy for each individual patient.”
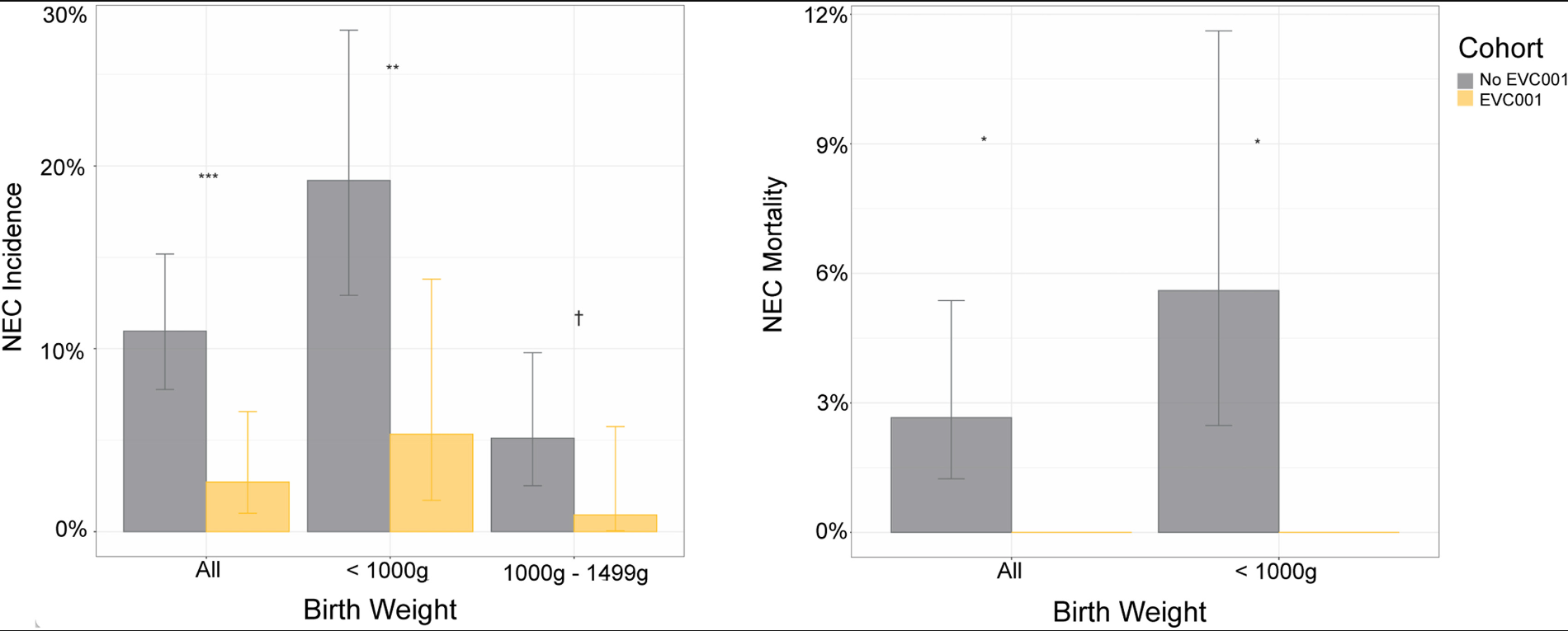
Methods: Nonconcurrent retrospective analysis of 2 cohorts of 483 very low birth weight (VLBW) infants not exposed and exposed to Binfantis EVC001 probiotic at Oregon Health & Science University from 2014 to 2020
Key findings:
The cumulative incidence of NEC diagnoses decreased from 11.0% (n = 301) in the no EVC001 (unexposed) cohort to 2.7% (n = 182) in the EVC001 (exposed) cohort (P < .01); this was a 73% risk reduction of NEC
NEC-associated mortality decreased from 2.7% in the no EVC001 cohort to 0% in the EVC001 cohort (P = .03)
There was a lack of adverse events (including probiotic sepsis)
Key points from editorial:
“The first cohort study showing a significant decrease in necrotizing enterocolitis (NEC) with the routine administration of probiotic dietary supplements [was] more than 20 years ago”
“The most recent Cochrane Database systematic review 2 included 56 randomized or quasi-randomized trials in which 10 812 infants participated. Meta-analysis found evidence for decreased risk of NEC (Risk ratio [RR] 0.54)”
Both the AGA and ESPGHAN have recommended routine probiotics administration to preterm infants. However, the AAP recommends “against routine probiotic administration citing ‘the lack of FDA-regulated pharmaceutical-grade products in the United States, conflicting data on safety and efficacy, and potential for harm in a highly vulnerable population.’”
“Recognizing that many neonatologists have opted to adopt routine probiotic administration to infants born preterm, the recent American Academy of Pediatrics statement6 recommends that an informed consent process for utilizing probiotics. Dr. Underwood counters: “there is no mention of a need to discuss these risks and benefits by those well-informed clinicians who may not believe that the data support administering probiotics. Inclusion of parents in decision-making in the NICU improves parent satisfaction and infant outcomes.”
My take: It is hard to understand that, despite 20 years of research showing probiotics can reduce mortality and morbidity in premature infants, we have not been able to manufacture a consistent, reliable high-quality probiotic capable of meeting FDA standards.
This retrospective study with 13 patients (10,187 catheter days [CDs]) compared ethanol locks (EL) with taurolidine locks (TL). Taurolidine is a “non-toxic, broad-spectrum antimicrobial” with growing use outside the U.S. Manufacturing issues still need to be addressed to gain FDA approval. Link: CORMEDIX RECEIVES COMPLETE RESPONSE LETTER FROM FDA FOR DEFENCATH™ CATHETER LOCK SOLUTION
Key findings from this study:
TL (vs EL) had lower rates of CVC breaks (1.11 vs 5.19/1000 CDs, P < 0.001), occlusions (0.83 vs 4.06/1000 CDs, P= 0.01) and repairs (1.94 vs 5.64/1000 CDs, P= 0.01)
There was no significant difference in CRBSI rates: 0.83/1000 CDs for TL vs 2.03/1000 CDs for EL (P= 0.25)
My take: Taurolidine, when available in U.S., may be a suitable alternative to ethanol, when available in U.S., in preventing CRBSI. In addition, taurolidine locks appear to have fewer mechanical risks.
This weekend, on “Wait, Wait, Don’t Tell Me” (Transcript July 2) on their ‘Bluff the Listener’ game, they highlighted three stories of a new Philadelphia tourist attraction. The true (very funny) story was regarding “The Relief Room.” A bathroom (suitably) dedicated to Philadelphia pitcher relievers and covered in memorabilia.
GONDELMAN: 45-year-old Matt Edwards, has gone above and beyond turning his home’s downstairs bathroom into a monument to his beloved Phillies.
GONDELMAN: The Relief Room, as Edwards calls the commode, is a celebration of retired Phillies relief pitchers.
GONDELMAN: Though the room is jampacked with Phillies ephemera, such as signed photographs and figurines, the area above the toilet remains largely empty. That’s because it’s reserved especially for pitchers who have played for Phillies championship teams.
GONDELMAN: Edwards did miss an opportunity for guests to declare their need for personal relief the same way that catchers deliver signals to a pitcher – throw down one finger if you need to do what the Phillies do with a late-inning lead…
GONDELMAN: …Two fingers if you need to do what the team is playing like overall.
In the past 30 years, the hepatitis B vaccine has been included in infant immunization schedules in the U.S. The authors studied a large, comprehensive, and nationally representative data set (NHANES data from 1999-2018) to assess its efficacy.
Key findings:
HBV vaccination was associated with reduced risk of all-cause mortality (HR, 0.78; 95% CI, 0.68–0.90) and cancer-related mortality (HR, 0.76; 95% CI, 0.58–1.00)
The highest vaccination uptake was found among those born after 1991, at 86.5%.
Vaccinated participants had higher prevalence of vaccine-induced immunity than the unvaccinated (47.2% vs. 7.4%). Among those born after 1991, vaccine efficacy (VE) was found at 58% (95% CI, 18%–79%) overall and 85% for those aged ≥20 years (mean age, 22), whereas no effect was found among those born prior to 1990
Context for these findings is noted in the associated editorial (pgs 1365-1367):
HBV remains one of the most deadly viruses worldwide with nearly 1 million deaths yearly and nearly 300 million people chronically-infected. The vast majority of unvaccinated children less than 1 year of age become chronically-infected. In the U.S., 98% of children acquired HBV through vertical transmission “including 26% of pediatric cases who were born in the USA or Canada”
My take: This study shows that HBV vaccine maintains strong protection for 20 years and protects against cancer and death.
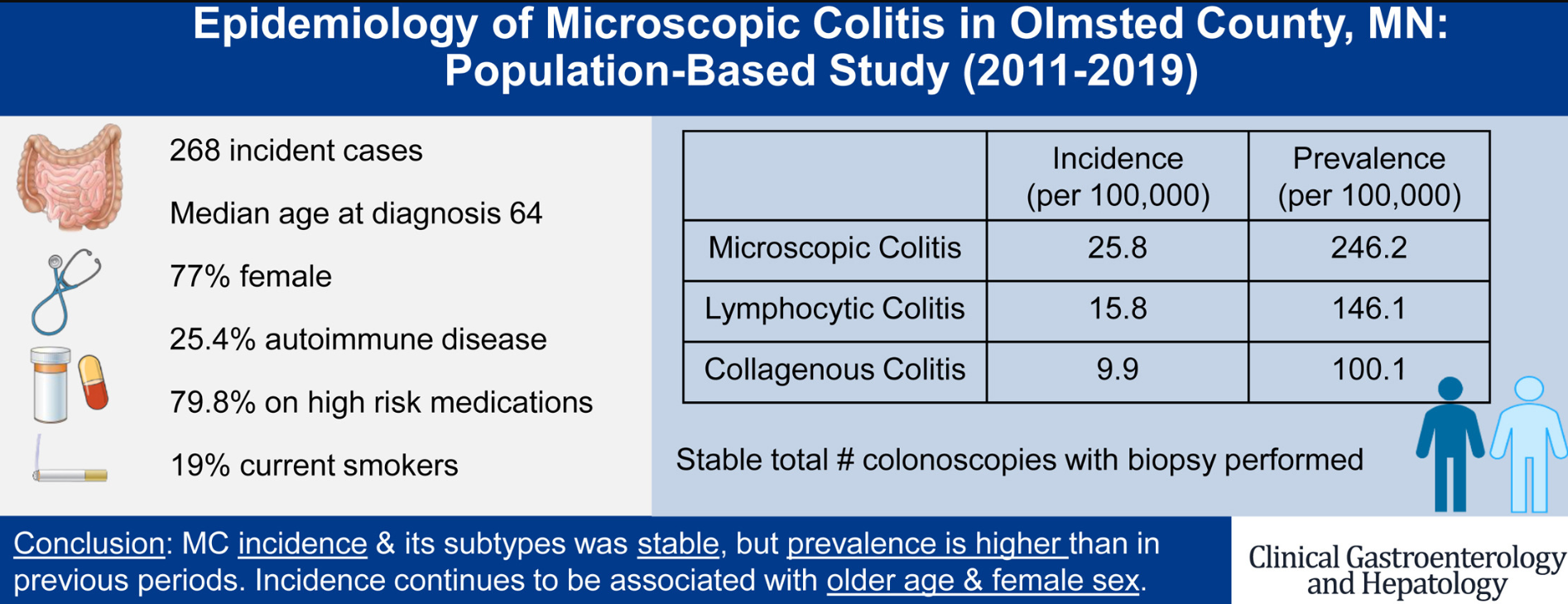
“The overall incidence of MC in Olmsted County, MN, increased from 1985 to 2001, stabilized between 2002 and 2010, and continues to show a plateau between 2011 and 2019.”
Medications associated with a risk of microscopic colitis (MC) include statins, SSRIs, PPIs, aspirin, other NSAIDs, and histamine H2-receptor antagonists within 3 months of diagnosis. “A recent US multicenter cohort study found an inverse association with PPIs and histamine H2-receptor antagonists when compared with controls with chronic diarrhea; only NSAID use was associated with MC. 31 It is plausible these medications do not cause MC, but instead aggravate diarrhea and bring the diagnosis to clinical attention.”
This was open-label study of enzyme replacement therapy (ERT) in 31 children and adults with lysosomal acid lipase deficiency (LALD). Sebelipase Alfa, a recombinant human lysosomal acid lipase, was FDA approved in 2015 for LALD.
Key findings:
Liver biopsies showed mostly improved or stable histopathology at 48 and 96 weeks versus baseline. In addition, there was modest improvement in transaminases; median ALT and AST levels changed by −42.0 and −22.0 U/L, respectively.
Median low-density lipoprotein cholesterol levels decreased by 52.6 mg/dL, and median high-density lipoprotein cholesterol increased by 9.8 mg/dL. Though, 55% of the study population had concomitant lipid-modifying therapy
Two patients tested positive for nonneutralizing, anti-drug antibodies
In the associated commentary (pgs 726-727), the authors state this study showed that “in contrast to infantile disease, ERT is not universally beneficial in individuals with attenuated disease…[and] it is impossible to predict response to ERT.” Testing for LALD is recommended for infants with hepatomegaly, poor growth, diarrhea or adrenal insufficiency. In older groups, LALD needs to be considered in those with hepatomegaly, steatosis, and dyslipidemia.
My take: There are still many questions regarding ERT’s long-term benefit in individuals with LALD, especially those with mild disease.