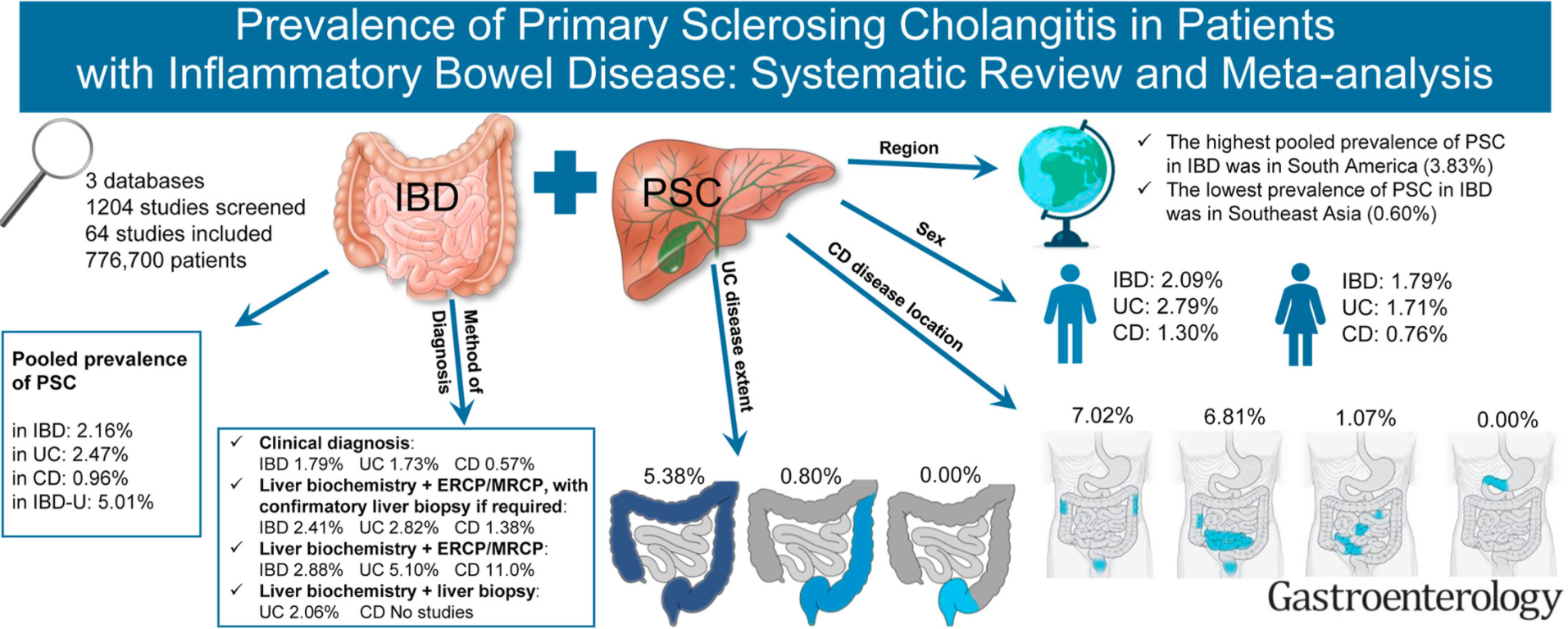
Key findings: Overall, pooled prevalence of PSC in IBD was 2.16%; the pooled prevalence was significantly higher in UC versus CD (OR 1.69)
Related blog posts:
Aspen Webinar 2021 Part 5 -Autoimmune Liver Disease & PSC This lecture highlights studies show lack of efficacy with vancomycin, ursodeoxycholic acid and vedolizumab. Also, there is potential utility of MMP-7 for distinguishing between PSC and AIH
I would urge colleagues when they see infants in the first few months of life to always discuss safe sleep which is the number one cause of mortality in infants. A simple message can be added to standard ‘Smartphrases’ for every infant seen with reflux, colic and formula intolerance.
A terrific website that focuses on this crucial issue: Charlieskids.org; it has videos, do’s and don’ts as well as a link to Cribs for Kids (discounted safe crib website). In addition,this website has a book called “Sleep Baby Safe and Snug” which incorporates updated recommendations on safe sleep practices.
Here are some screenshots from CHOA’s twitter feed on this topic.
Related blog posts:
The High Toll of Sudden Infant Death From 2013-2015, there was an average of 3523 US infants each year who died from SUID (sudden unexpected infant death), peaking at 1-2 months of life. More black infants died of SUID in the first year than black children who died from firearm homicides in all of childhood through age 19 years. SUID deaths from 2013-2015 (10,568) was similar to the total number of motor vehicle-traffic deaths in all of childhood (10,714) and greater than the total number of any of the other causes.
Methods: The Rochester Epidemiology Project (REP) was used to identify Olmsted County, Minnesota residents aged <19 years who had 25-hydroxyvitamin D [25(OH)D] levels measured between January 2, 2002 and December 31, 2017. Using each patient’s first 25(OH)D measurement during this period, patients were categorized as vitamin D deficiency/insufficiency if Vit 25(OH)D level was <20 ng/mL.
To convert nmol/L to ng/mL= nmol/L x 0.401 OR nmol/L =ng/mL x 2.496
Key finding:
There was a 42-fold increase in the proportion of the county’s pediatric population tested each year, starting at 3.7 per 10,000 persons in 2002 and increasing to 156.1 per 10,000 persons in 2017
During the 16-year period, the incidence of vitamin D deficiency/insufficiency (per 10,000 persons) increased from 1.7 in 2002-2003 to 19.9 in 2016-2017, but the proportion that were tested and had vitamin D deficiency/insufficiency remained stable –rates of 21.9% in 2006-2007 and 18.5% in 2016-2017
There was a higher rate of Vit D deficiency/insufficiency in females (22.8%) vs males (16.9%) (P<.001)
There was a significant association with obesity and Vit D deficiency/insufficiency (32.7% with moderate and 32.9% with severe obesity). It is unclear whether this is a causal link or an association (perhaps associated with less outdoor activity)
Limitation: Study was performed in Olmstead county which is 90-95% white; this limits generalizability (though other reports have noted increased testing rates as well in other locations)
My take: Clearly more kids are being screened for vitamin D deficiency. More data is needed on whether this results in any meaningful improvements in outcomes and the associated costs. In addition, it is important to recognize that vitamin D levels can be inversely proportional to inflammatory conditions and can improve without supplementation by addressing these disorders.
When investigating elevated liver enzymes in teenagers, serology for autoimmune hepatitis (AIH) is frequently obtained. In the face of overweight/obesity, the majority will have nonalcoholic fatty liver disease (NAFL). How many with elevated autoantibodies actually have autoimmune liver disease (ALD)? Some information regarding this issue is available in the article by Khayat et al.
Methods: A retrospective, cross-sectional study of 181 children with a biopsy-proven diagnosis of NAFL, NASH, autoimmune hepatitis (AIH), or primary sclerosing cholangitis (PSC) and a body mass index (BMI) >85th percentile treated between 2007 and 2016.
Key findings:
Antinuclear antibody (ANA), anti-actin antibody, and anti–liver kidney microsomal (LKM) antibody were positive in 16.1%, 13.8%, and 0%, respectively, of the patients with NAFL and in 32.8%, 15.5%, and 0%, respectively, of those with NASH
Total immunoglobulin G (IgG) was elevated in 27.3% of the patients with NAFL and in 47.7% of those with NASH, but in 100% of those with ALD. A normal IgG level was the “strongest negative predictor of ALD, followed by a negative ANA and actin.”
The positive predictive value of LKM was 100% for ALD but only 29% for ANA and 46% for anti-actin antibody. ANA positivity in this cohort was associated with more insulin resistance
ALD was present in 29/181 (16%). 12 (6.6%) with isolated ALD (AIH, PSC, or overlap), and 17 (9.4%) with combined ALD and NAFLD
BMI >98% “appears to be an important breakpoint above which ALD is less likely” even when IgG is high with a positive ANA
Limitations: Retrospective study, not every patient had all of the ALD serology tests
My take: Even heavy kids may have autoimmune liver disease. In those with abnormal serology, about 1 in 6 will have ALD, either in combination with NAFL or as the sole etiology of abnormal LFTs.
Background: “SER-109, an investigational oral microbiome therapeutic composed of live purified Firmicutes bacterial spores, was developed to reduce the risk of C. difficile infection recurrence.14 We hypothesized that these spore-forming bacteria would compete metabolically with C. difficile for essential nutrients, modulate bile-acid profiles to reestablish resistance to colonization, or have both of these effects. Here, we report the 8-week efficacy and safety results from a phase 3 [double-blind, randomized, placebo-controlled] trial involving patients with recurrent C. difficile infection, along with supportive microbiome engraftment and metabolomic analyses.”
Methods: N=182 enrolled in the “ECOSPOR III” trial; all patients had at least 3 infections in past year and positive toxin test. After standard-of-care antibiotic treatment, patients received SER-109 or placebo (four capsules daily for 3 days). The primary efficacy objective was to show superiority of SER-109 as compared with placebo in reducing the risk of C. difficile infection recurrence up to 8 weeks after treatment.
Key findings:
The percentage of patients with recurrence of C. difficile infection was 12% in the SER-109 group and 40% in the placebo group (relative risk, 0.32)
The recurrence risk following SER-109 was even lower after fidaxomicin than vancomycin: relative risk, 0.09 [95% CI, 0.01 to 0.63] with fidaxomicin and 0.41 [95% CI, 0.22 to 0.79] with vancomycin
SER-109 dose species were detected as early as week 1 and were associated with bile-acid profiles that are known to inhibit C. difficile spore germination.
My take: This study shows that clinical outcomes with C difficile may be improved by the addition of this microbiome therapeutic after standard therapy. Engraftment of Firmicutes bacteria as a dominant component of the microbiome is generally associated with a healthy state. This opens the door for treatment of other conditions that may benefit from microbiome modulation.
Methods: This interview-questionnaire study used a test-negative case-control design, enrolling persons who received a positive (case-participants) or negative (control-participants) SARS-CoV-2 test result, from among all California residents, without age restriction, who received a molecular test result for SARS-CoV-2 during February 18–December 1, 2021. A total of 652 case- and 1,176 control-participants were enrolled in the study equally across nine multi-county regions in California.
Limitations included the following:
This study did not account for other preventive behaviors that could influence risk (eg distancing)
This analysis relied on an aggregate estimate of self-reported face mask or respirator use across, for some participants, multiple indoor public locations
Estimates do not account for face mask or respirator fit
Data collection occurred before the expansion of the SARS-CoV-2 B.1.1.529 (Omicron) variant
On this website: “Four presentations/lectures were released at the Nutritional Therapy for IBD Virtual Booth that provide a comprehensive review and update of the latest information regarding the use of EEN and therapeutic diets in the management of IBD”
Why Do We Need Dietary Therapies for IBD
Presenter: Lindsey Albenberg, DO
Dr. Lindsey Albenberg, a clinician and researcher from Children’s Hospital of Philadelphia, describes the rapidly increasing incidence of IBD and its relationship to diet, microbiome and the immune system. She reviews the rationale and science supporting the use of dietary therapy to compliment drug therapy as an avenue to potentially achieve higher, more sustainable and possibly safer levels of remission long term in pediatric patients.
The Crohn’s Disease Exclusion Diet Updates: December 2021
Presenter: Rotem Sigall Boneh, RD. Rotem Sigall Boneh, RD, a primary researcher and developer of CDED, provides an overview of the accumulating data with CDED in combination with PEN, including the newly published results of adult data with important endoscopic findings and further shares real world experience and application of nutritional therapy.
IBD Anti-inflammatory Diet or IBD-AID: Proof of Concept
Presenter Ana Maldonado-Contreras, MSc, PhD. Dr. Ana Maldonado-Contreras, a lead researcher in IBD-AID explains the relationship between diet, microbiome and immune function with the design and rational of IBD-AID to manipulate the microbiome. She shares the recently published data of the impact of IBD-AID on the microbiome and cytokine levels specific to food components.
At the NTforIBD Nutritional Symposium prepared for NASPGHAN2021, Professor Day provides insight into the important role of EEN, an underutilized option to both induce remission and improve outcomes in complicated and peri-operative patients.
This editorial helps provide needed context on the associated observational study by Xia et al (B Xia, M Yang et al. Gastroenterol 2021; 161: 1842-1852. Open Access. Regular use of proton pump inhibitor and the risk of inflammatory bowel disease: pooled analysis of 3 prospective cohorts) which showed a mild increase risk of IBD among PPI users. While the PPI users were at 42% increased risk of IBD compared to nonusers, if correct, “the absolute risk associated with PPI use is modest. Number needed to harm is 3770, meaning that when 3770 individuals are treated with PPIs for 1 year, 1 additional case of IBD is observed.”
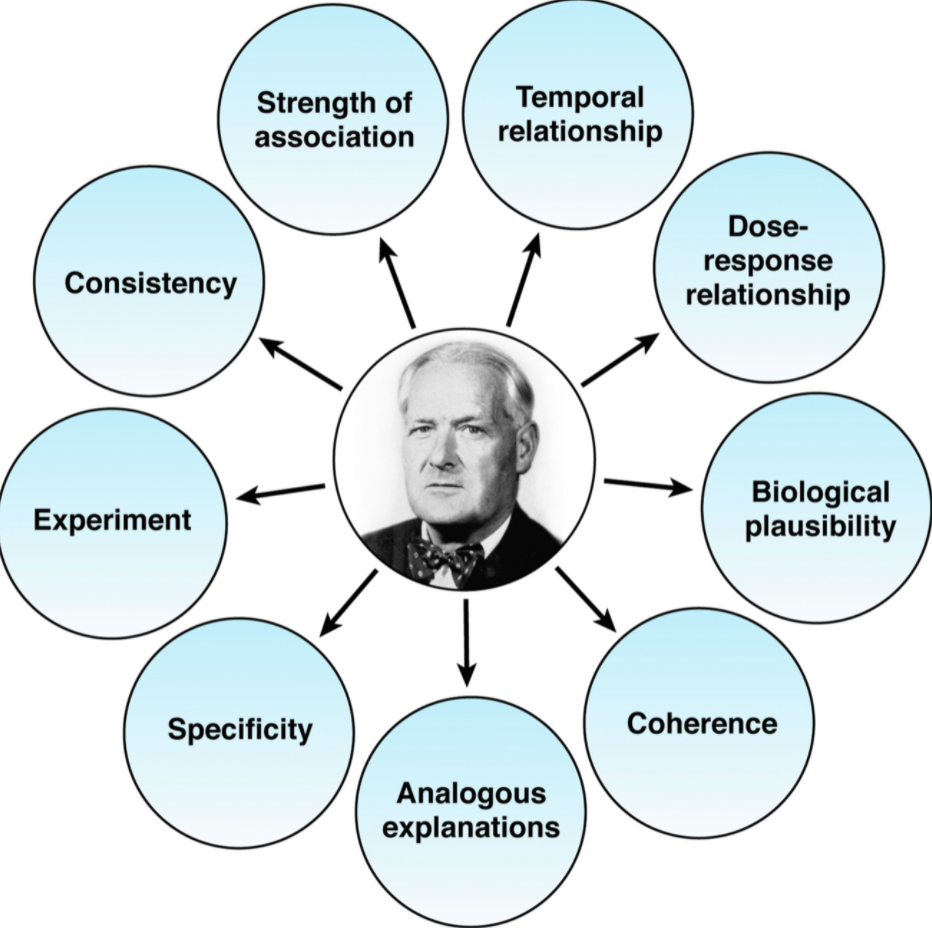
Despite the efforts of the study authors to minimize confounders, the editorial focuses on the work of Austin Bradford Hill (Proc R Soc Med. 1965;58: 295-300. The environment and disease: association or causation?) who “realized making causal inferences on observational data was challenging and outlined a list of factors that would make this interpretation more or less likely….strength of association, dose response, and consistency are important and often not commented on in observational studies.”
In a previous “a double-blind, randomized clinical trial comparing pantoprazole with placebo over 3 years with more than 53,000 patient years follow-up found there was no association” with IBD identified…Interestingly, this trial reported a slightly higher risk of enteric infections, and this is the underlying mechanism proposed for how PPI therapy may increase the risk of IBD.”
My take (borrowed from editorial): “Most associations for PPI and harm are likely to be residual or unmeasured confounding, whether this is also true for IBD will only be determined by further study.”
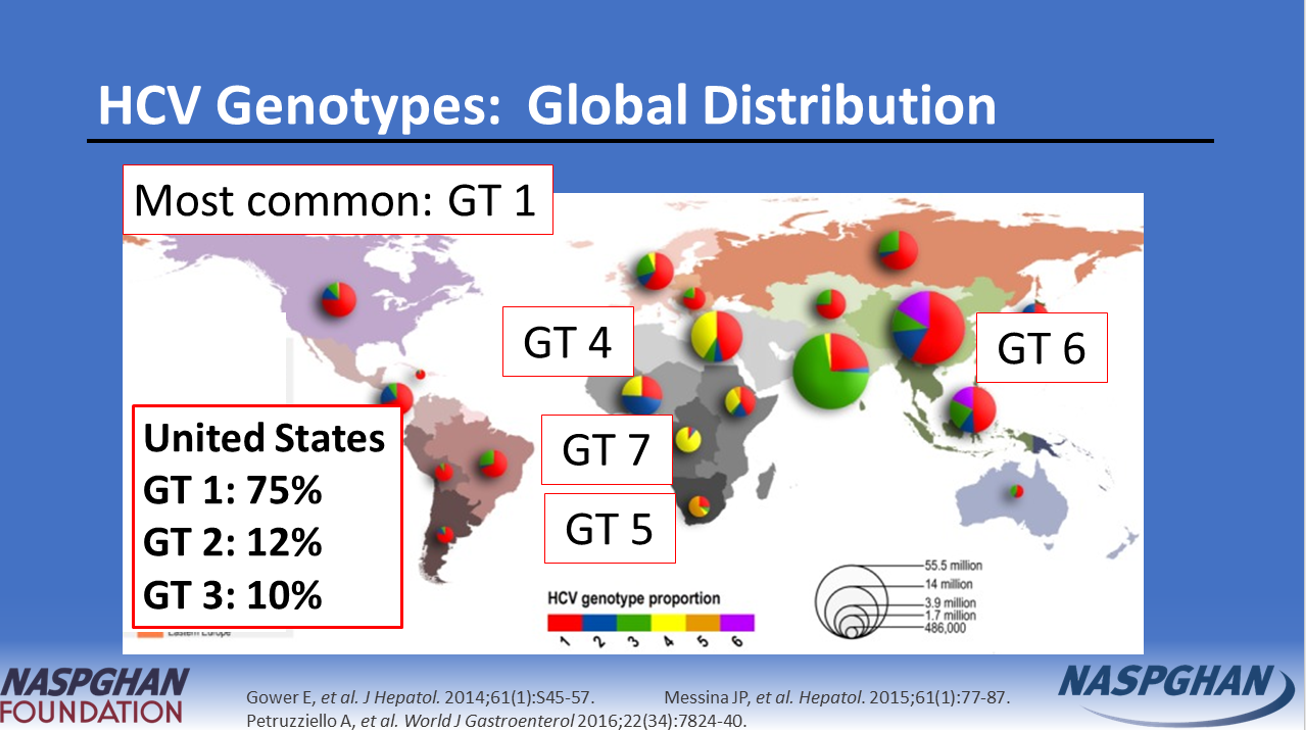
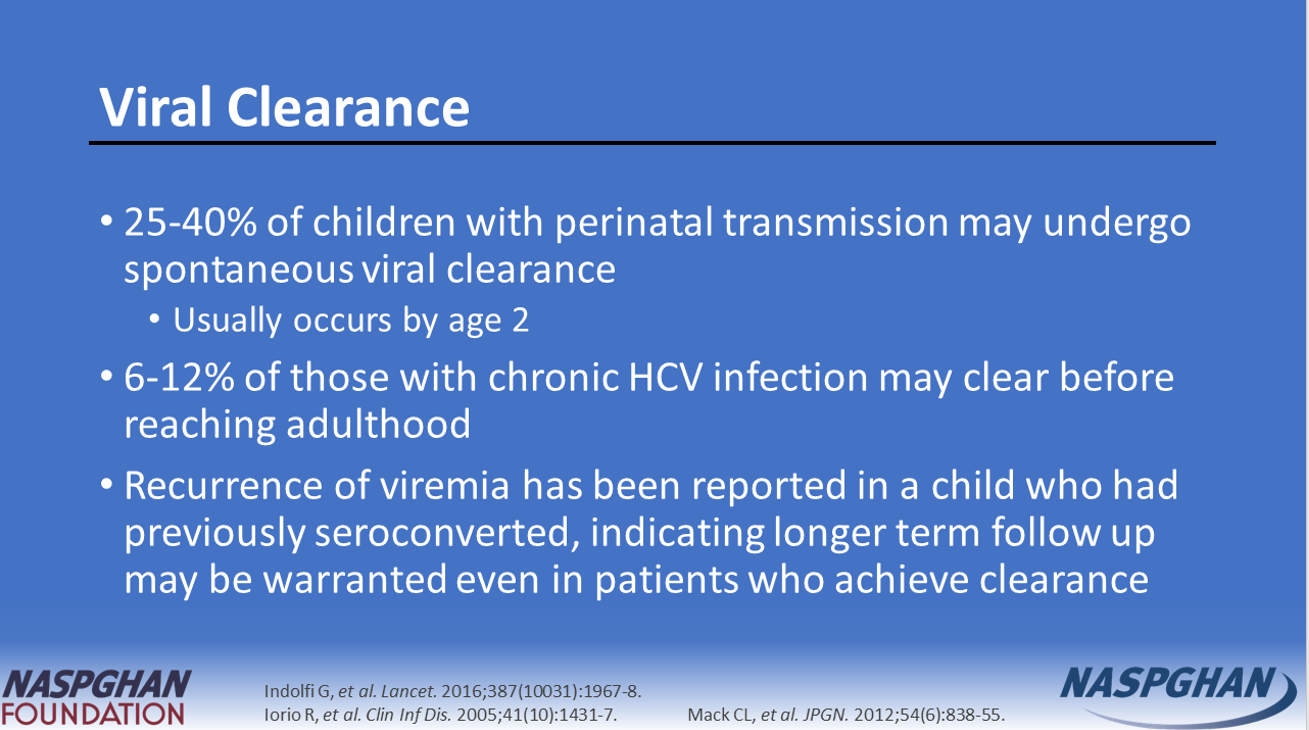
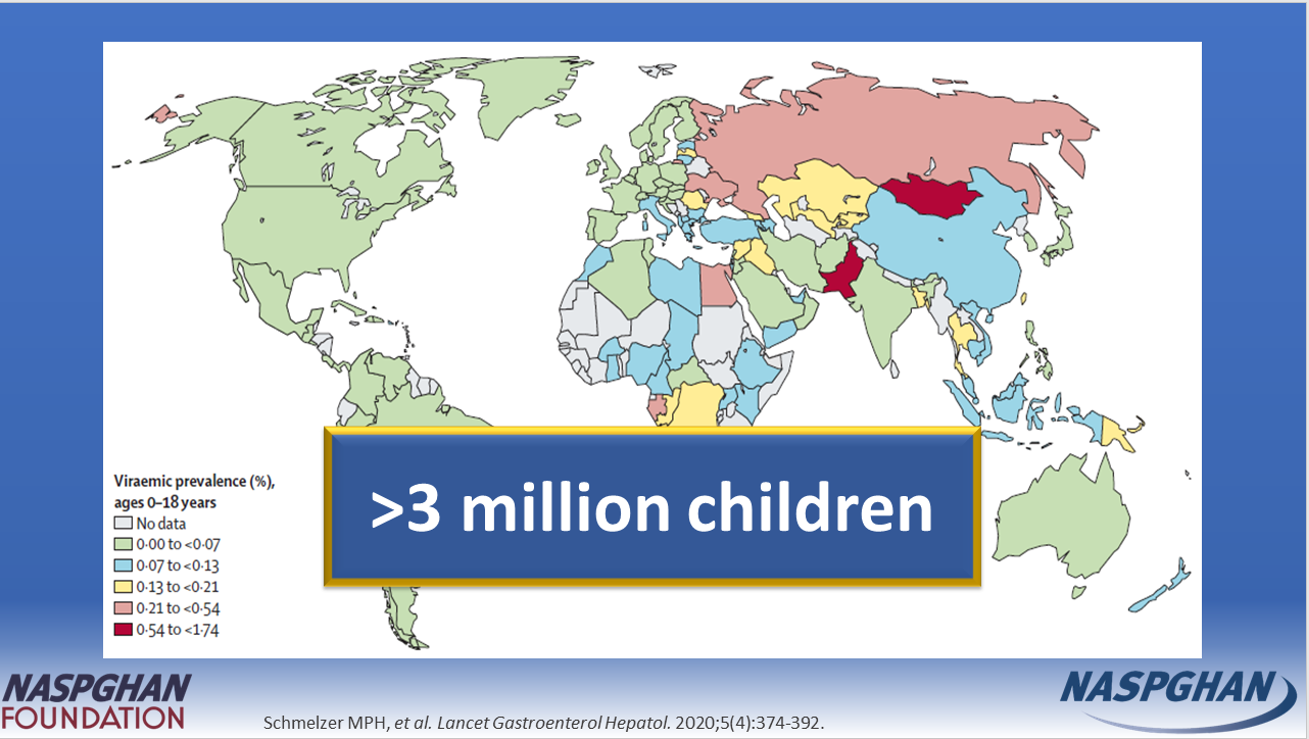
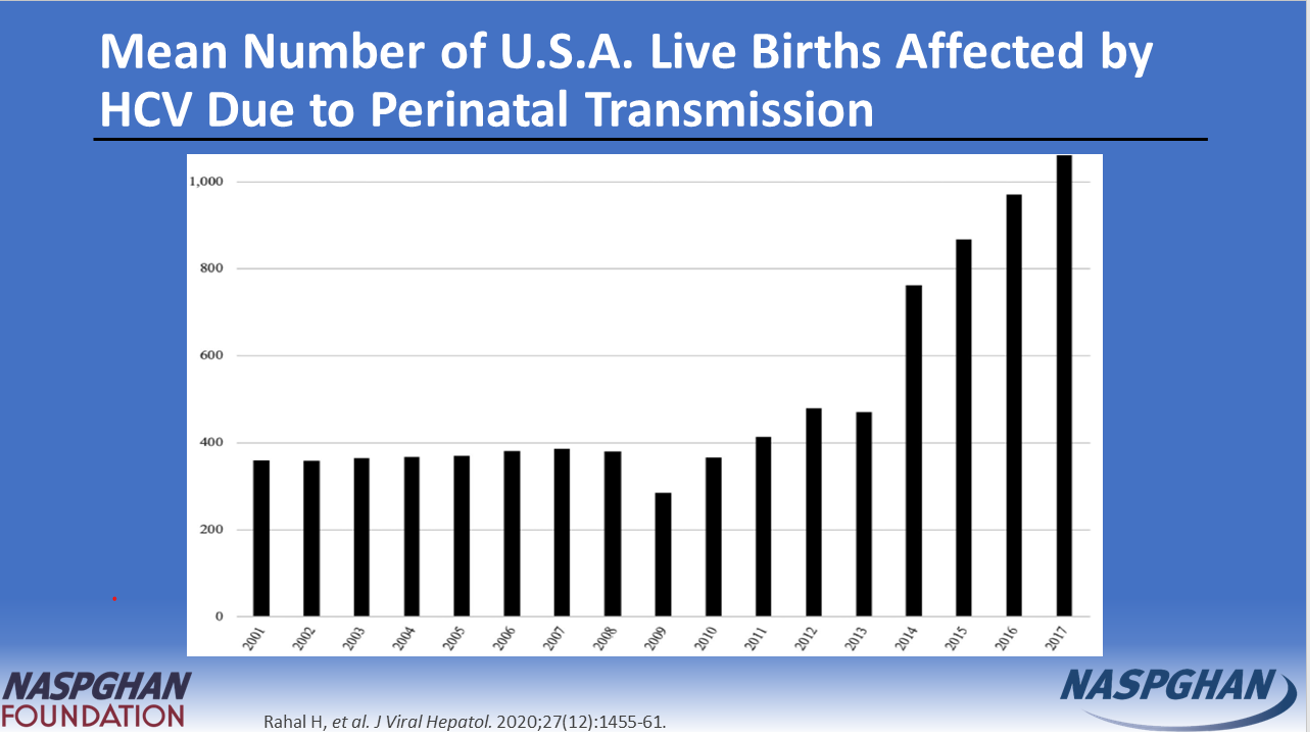
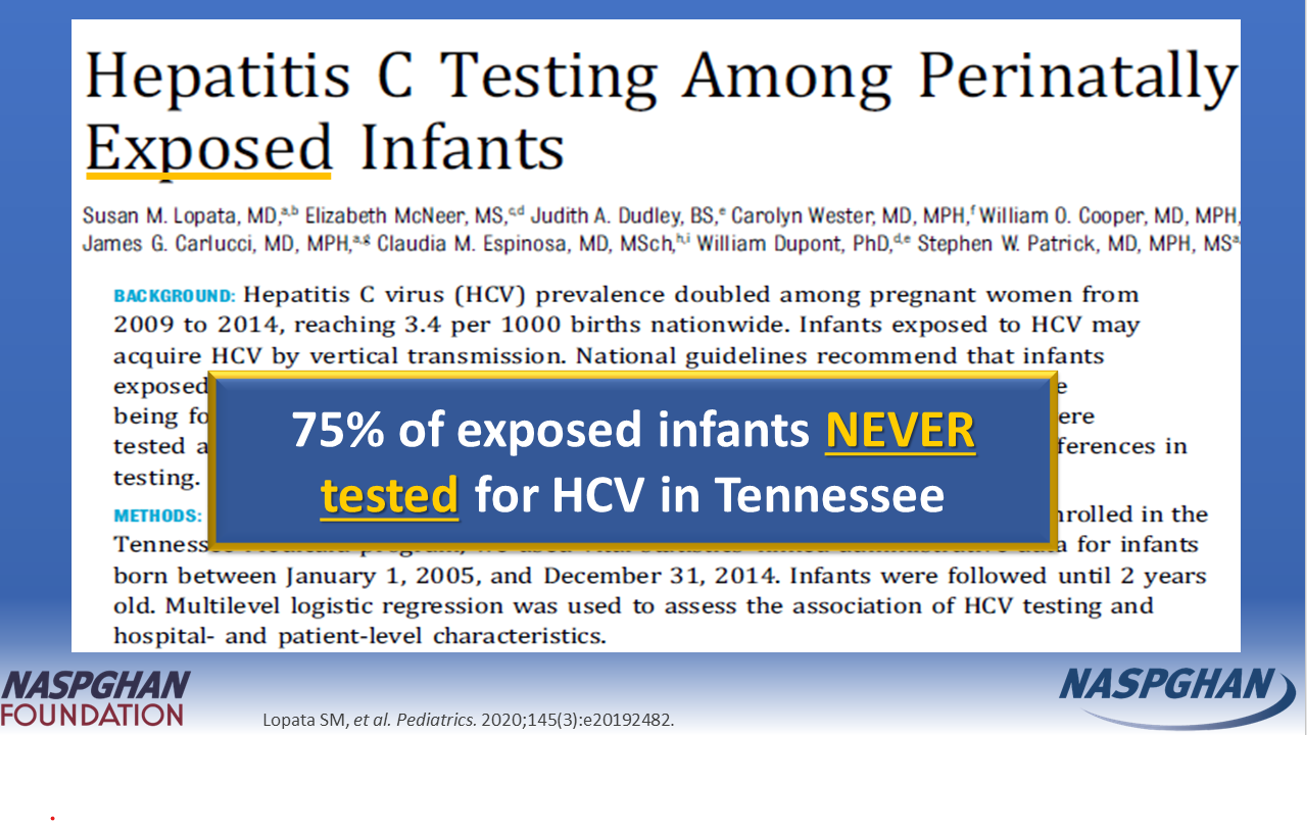
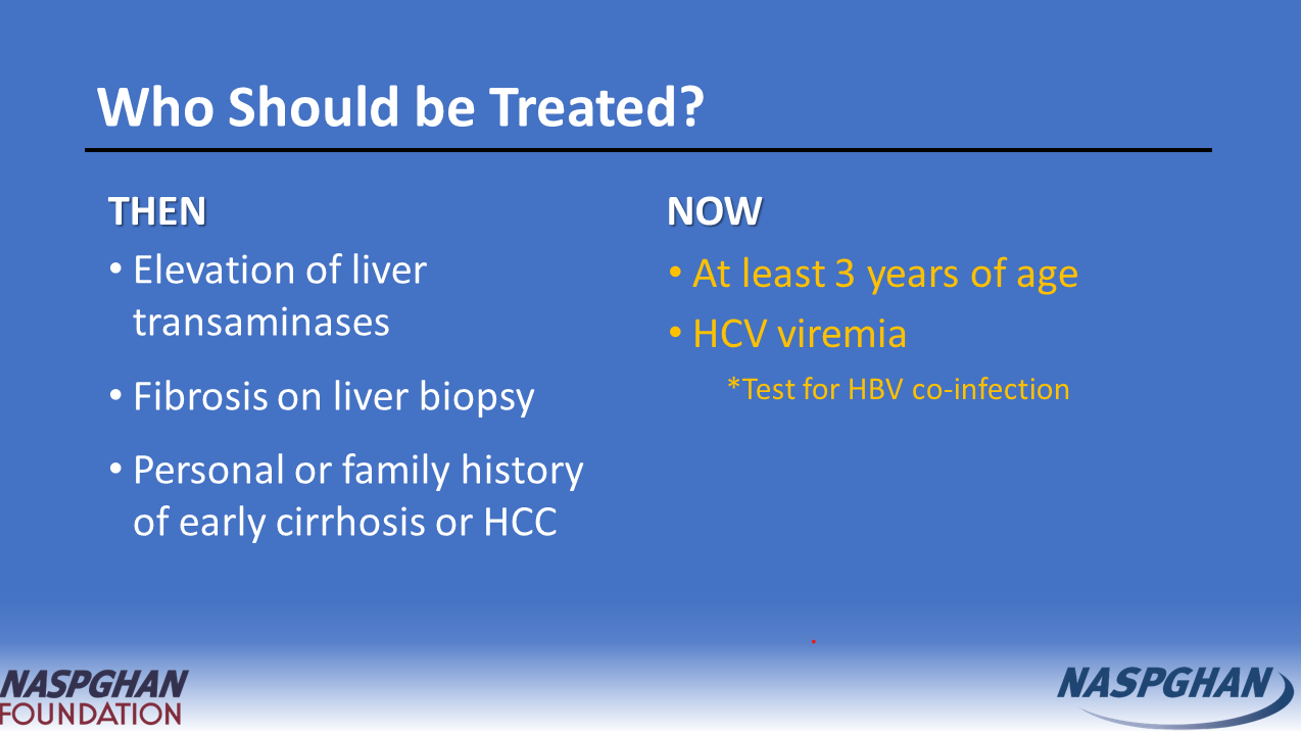
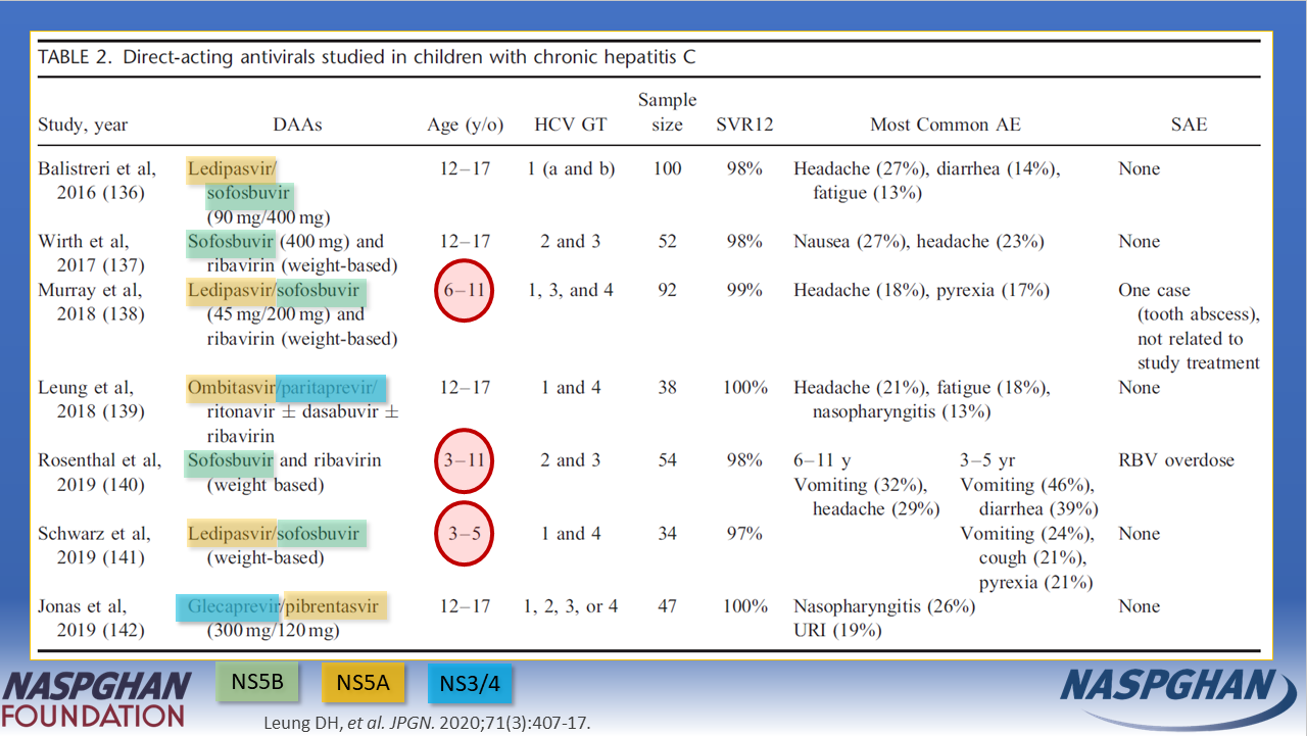
This past month, I participated as a lecturer for the NASPGHAN Foundation’s educational campaign on Hepatitis C in Children and Adolescents. The slides highlight some tremendous advances and challenges in the field of viral hepatitis. I have copied some of the slides below (used with permission) and the full slide deck can be obtained via this link: Hepatitis C in Children and Adolescents
Gilead is a corporate sponsor for these talks. (Disclosure: I have requested that the honorarium for these lectures to be directed back to the NASPGHAN Foundation.)
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.