
JA Sninsky et al. Clin Gastroenterol Hepatol 2026; 24: 1666-1674. Open Access! The Real-World Impact of Vitamin D Supplementation on Inflammatory Bowel Disease Clinical Outcomes
Methods: This was a retrospective cohort study of adult patients (n=5021) with IBD seen in the national Veterans Health Administration system from 2000 to 2023. The researchers used 3 different methods to try to determine causality of improved outcomes with supplementation of Vitamin D.
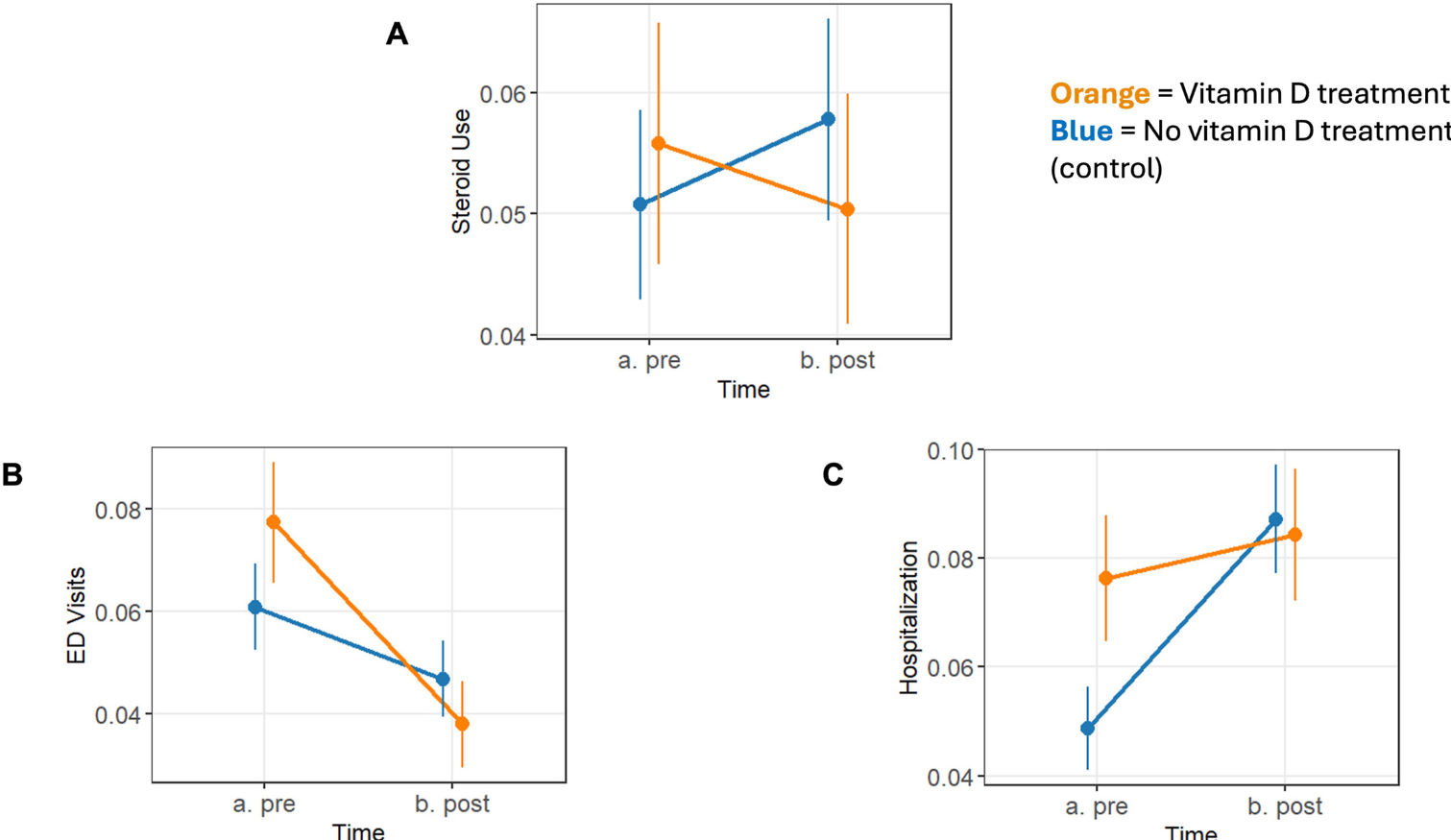
- “Difference-in-differences (DiD) approach to compare changes in clinical outcomes before and after vitamin D testing between patients who did and did not receive supplementation”
- “The regression discontinuity design leveraged the clinical threshold of 30 ng/mL serum 25-hydroxyvitamin D, comparing outcomes in patients just lower than and just higher than this cutoff, who are assumed to be otherwise similar”
- “The inverse probability weighting method adjusted for confounding by weighting patients based on their likelihood (propensity) of receiving vitamin D15“
Key findings:
- The median 25-hydroxyvitamin D level was 23 ng/mL, and 41% received vitamin D supplementation
- Vitamin D supplementation was associated with reduction in IBD-related emergency department visits by 2.17% (34.4% relative risk reduction; P = .007), hospitalizations by 2.64% (53.18% relative risk reduction; P = .003), and corticosteroid prescriptions by 1.29% (25.13% relative risk reduction; P = .066)
Discussion:
- “Collectively, our data strongly suggest that vitamin D supplementation reduces the risk of IBD flare, underscoring its promise as an effective adjunctive therapy in clinical practice.”
- “Vitamin D deficiency is prevalent among patients with IBD and is strongly linked to poor clinical outcomes, including higher rates of hospitalization and surgery. Patients with IBD are 64% more likely to be vitamin D deficient compared with healthy control subjects.29“
- “Vitamin D deficiency is prevalent among patients with IBD and is strongly linked to poor clinical outcomes, including higher rates of hospitalization and surgery. Patients with IBD are 64% more likely to be vitamin D deficient compared with healthy control subjects.29“
- “Although these findings support a strong association between vitamin D deficiency and worse clinical outcomes, they do not address whether supplementation itself mitigates the risk of adverse events, because disease severity confounds this relationship.33 Our study fills this knowledge gap and provides rigorous real-world data to support the effectiveness of vitamin D supplementation.”
My take: There have been large studies (eg. VITAL) study showing that Vitamin D supplementation does not help most people in the general population. In addition, many individuals with IBD who have low Vitamin D levels may see improvement in Vitamin D status by treating the IBD (without Vitamin D supplement). Yet, studies like this one by Sninsky indicate that Vitamin D supplementation is associated with improved outcomes in this retrospective cohort; the study methods likely indicate a causal effect of supplementation; however, a prospective randomized controlled study would be more definitive.
Related blog posts:
- The End of the Vitamin D Epidemic (VITAL Study) (2022)
- IBD Updates: How to Get Rid of Pesky Antibodies to Infliximab, Neoplasia in pouch, Vit D associated with improved IBD outcomes (2024)
- Why I Don’t Check Vitamin D Levels During IBD Flareups
- Vitamin D and IBD, More Data
- How Important Is It to Correct Vitamin D Deficiency in a Critically-Ill Patient?
- Common to be “D-ficient” | gutsandgrowth
- Explaining the Vitamin D Paradox | gutsandgrowth
- Why Adding Vitamin D May Not Help IBD | gutsandgrowth
- Understanding Why Vitamin D Deficiency is Not So Common Afterall | gutsandgrowth
- Single High-Dose Oral Vitamin D Therapy … – gutsandgrowth








