Taft et al performed a retrospective study of 103 adult patients with eosinophilic esophagitis. Patients completed the following questionnaires immediately before to endoscopy:
Esophageal Hypervigilance and Anxiety Scale (EHAS)
Brief Esophageal Dysphagia Questionnaire (BEDQ)
Eosinophilic Esophagitis Symptom Activity Index (EEsAI)
Northwestern Esophageal Quality of Life Scale (NEQOL).
Endoscopic severity of EoE was graded using the EoE Endoscopic Reference Score System (EREFS). Dysphagia was the primary symptom in 73% of the patients.
Key findings:
Patient’s symptom severity (via EEsAI or BEDQ) did not correlate with histology (distal or proximal peak eosinophil count), endoscopic severity of the disease (EREFS), or the distensibility index (measured via functional lumen imaging probe)
Symptom severity was correlated with the Esophageal Hypervigilance and Anxiety Scale (EHAS)
There was no correlation between EHAS and histologic activity, endoscopic severity (EREFS), or the presence of a stricture
The associated commentary emphasizes some of the study limitations including taking surveys prior to endoscopy (increased anxiety).
My take: This study indicates that with eosinophilic esophagitis, similar to other organic diseases (eg. IBD), patient symptoms do not always correlate with disease severity, and addressing the impact of anxiety and hypervigilance is critical, especially in refractory symptoms.
This case series of 13 nondirected liver donors (ND-LLDs) (from 2012-2020) helps highlight this increasing trend of motivated donors who do not have a predetermined recipient. The Scientific Registry of Transplant Recipients documented 105 patients who underwent a living donor liver transplantation (LDLT) from ND-LLDs 2000-2019, with 39 in 2019 alone.
Key points:
While the article states that carefully selected ND-LLDs at high volume centers have excellent outcomes, the associated editorial (pg 1373-74) notes that there is a 0.2% living donor operative mortality. And, a significant number experience negative physical and socioeconomic effects of donation
The authors advocate more use of SPLIT livers to increase the donor pool (currently at 10 centers) to lower pediatric deaths on the waitlist
The authors note that the likelihood of receiving a LT is increased at high-volume pediatric centers (85%) compared to low-volume centers (41%). “Center expertise and volume is an important consideration…especially true for pediatric liver transplantation, which is relatively infrequent…551 [in 2019]” compared to 8345 adult liver transplants.
The commentary places some context regarding the donors.
70% had previously donated a kidney (“Repetitive donor disorder?”)
Yet, “in some sense, nondirected donors may be the best qualified donors, as they are free of coercion”
The authors advocate for a “safe, well-informed” process and for national guidelines to address risks and the components of evaluation, medical and psychosocial
My take: It is amazing how much some individuals are willing to sacrifice to help others, especially in age when some react so harshly to being asked to consider the needs of their community.
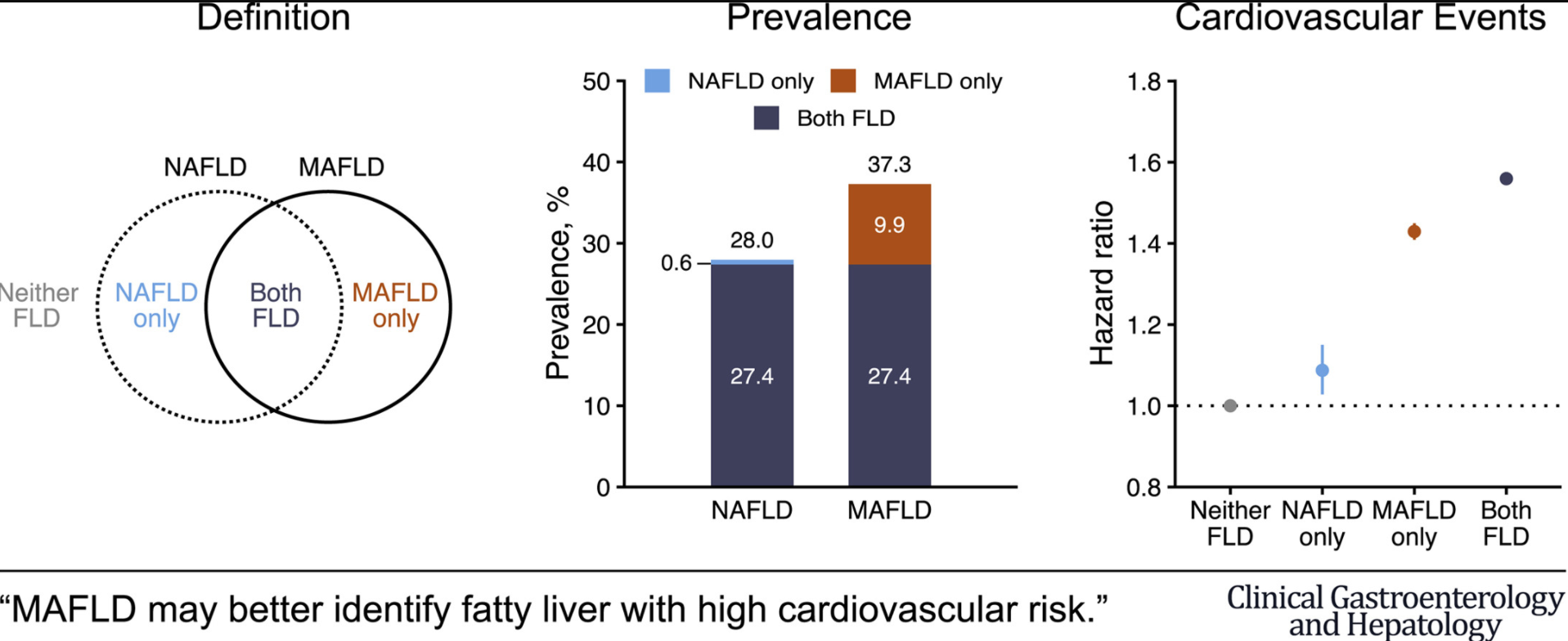
A recent study from South Korea with 9.5 million participants (followed for 10 years) shows that changing to metabolic dysfunction–associated fatty liver disease (MAFLD) as a name change from nonalcoholic fatty liver disease (NAFLD) changes the prevalence of at-risk individuals.
Key findings:
Prevalence of NAFLD and MAFLD were 28.0% and 37.3%, respectively
NAFLD and MAFLD were each associated with significantly higher risk for CVD events: multivariable-adjusted hazard ratios (95% confidence interval) for CVD events were 1.09 (1.03-1.15) in the NAFLD-only group, 1.43 (1.41-1.45) in the MAFLD-only group, and 1.56 (1.54-1.58) in the Both-FLD group
In the same issue, a study from Hong Kong showed similar prevalence rates between MAFLD (25.9%) and NAFLD (25.7%) (Clin Gastroenterol Hepatol 2021; 19: 2161-2171). This study noted that many people with hepatic steatosis at baseline have less severe metabolic burden.
Also, in the same issue, using a well-define population of more than 13,000 from NHANES III, this retrospective study (Clin Gastroenterol Hepatol 2021; 19: 2172-2181) found that Non-NAFLD MAFLD patients had the highest all-cause and cardiovascular-cause related mortality. In addition, this group had the highest rate of advanced fibrosis >7% (compared to <2% in other groups.
My take (borrowed from authors of first study): “The change from NAFLD to MAFLD criteria may identify a greater number of individuals with metabolically complicated fatty liver and increased risk for CVD.”
MAFLD is diagnosed based on the presence of hepatic steatosis with one or more of the following:
diabetes mellitus
overweight/obesity (BMI >/= 23)
at least 2 metabolic abnormalities: a) Waist circumference ≥90 cm in men and 80 cm in women. b) Blood pressure ≥130/85 mmHg or under anti-hypertension therapy. c) High-density lipoprotein cholesterol (HDL-C) <40 mg/dL for males and <50 mg/dL for females. d) Triglyceride (TG) ≥150 mg/dL or specific drug treatment. e) fasting glucose ≥100 f) Homeostasis model assessment-insulin resistance (HOMA-IR) score ≥2.5; and g) Hypersensitive C-reactive protein (hs-CRP) level >2 mg/L.
NAFLD Criteria in this study:
The presence of hepatic steatosis without 1. excessive drinking ( ≥30 g/day in men, ≥20 g/day in women) and 2. concomitant liver diseases
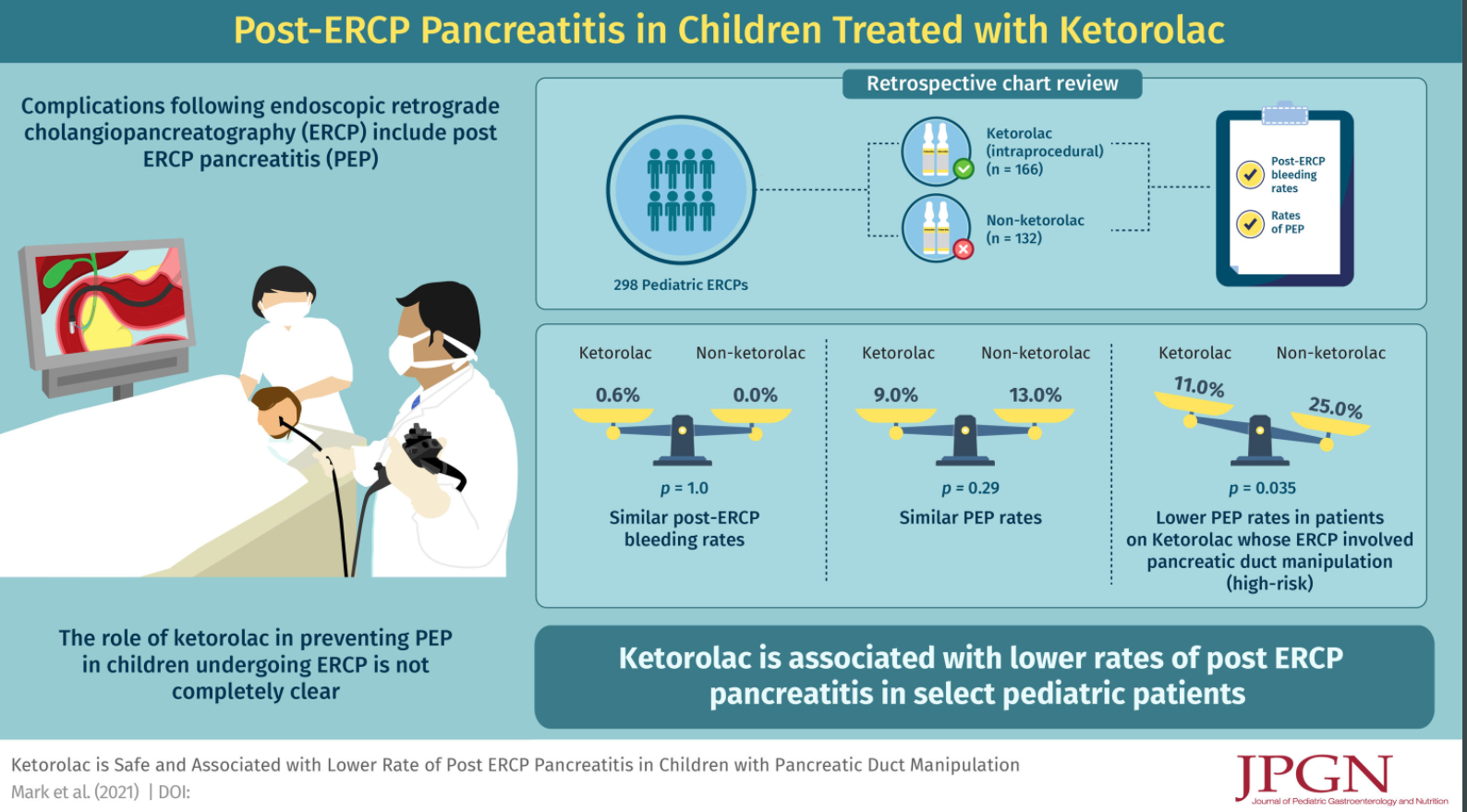
Methods: This retrospective chart review (n=298) examined the outcomes of pediatric patients who receivied ketorolac during ERCP compared to those who did not; ketorolac, was dosed using weight-based dosing (0.5 mg/kg/dose max 30 mg).
Key findings:
Most common indications for ERCP were choledocholithiasis, biliary stricture, and chronic/recurrent pancreatitis
Therapeutic ERCP: 91% of ketorolac group and 89% of non-ketorolac group; sphincterotomy was performed in 55% of both groups
Post-ERCP bleeding rates were not significantly different between ketorolac and non-ketorolac groups (0.6% vs 0%, P = 1)
PEP (post-ERCP pancreatitis) rates were not significantly different between the ketorolac and no ketorolac group 15/166 vs 17/132 (9% vs 13%, P = 0.29)
Patients who had cannulation and/or injection of the PD had significantly higher rates of PEP (23/140 (16%) vs 9/158 (6%), P < 0.003)
For high-risk pediatric patients with injection of contrast into and/or cannulation of the pancreatic duct, the rates of PEP were significantly lower for patients who received ketorolac (11% vs 25%, P = 0.035). In Table 2, the authors indicate that PEP in this high risk group occurred in 11/88 (12.5%) [mild discrepancy from abstract of 11%] of ketorolac group and 13/52 (25%)
It is possible that ketorolac (or other NSAIDs) in all patients may be beneficial but difficult to demonstrate without a larger cohort. In adults, “indomethacin reduces risk and severity of PEP in both high and average risk adults…and there is some evidence that NSAIDS given before ERCP may be more effective than those given later.” Thus, the authors state that use of ketorolac could be administered to all ERCP patients beforehand (w/o contraindication) or limited to the higher risk patients.
My take: In pediatric patients needing an ERCP, those with high-risk features (eg. injection of contrast into and/or cannulation of the pancreatic duct), use of ketorolac is likely to reduce the frequency of post-ERCP pancreatitis.
“It was Feb. 1, 1960, when four black students sat down at Woolworth’s lunch counter in Greensboro, N.C., and ordered coffee” (Time: Why the Woolworth’s Sit-In Worked)
This lunch counter sit-in was a big step in the civil rights movement. The article cited above shows that there is still a lot of work to make sure black patients have equal access to the liver counter too.
Using two databases (CDC WONDER, and UNOS) for 2014-2018, the authors identified 135,367 patients who died of ESLD, 54,734 patients who were listed for transplant, and 26,571 who underwent transplant.
Key findings:
The national LDR (listing-to-death ratio) was 0.40, significantly lowest in Black patients (0.30), P < 0.001. The highest LDRs clustered in the Northeast and the lowest in the Southeast and Northwest
The national transplant to listing ratio was 0.48, highest in Black patients (0.53), P < 0.01
The national transplant to death ratio was 0.20, lowest in Black patients (0.16), P < 0.001
“The most desirable outcome is a high transplant to death ratio—which was present in states like Maryland as well as Georgia, Nebraska, and Wisconsin.” (State values are provided in Tables 1, 3, and 4). Overall, these data show low listing rates for black patients relative to deaths from ESLD. Due to the adoption of MELD score which has objective criteria, the lower transplant rates indicate that Black patients face a disparity in access to liver transplantation.
The authors point out potential roadblocks:
ESLD first needs to be identified and patient referred to a liver transplant center
Black patients “were much less likely to understand the LT process”
Timing is critical, “especially in patients with HCC, which presents a more advanced in Black patients”
Insurance: “Black patients are more likely to be uninsured or to have public insurance, which is associated with poor access to listing and LT”
My take: This study shows that Black patients face disparities prior to transplant listing. In order to improve outcomes, patients first need to get a seat at the table.
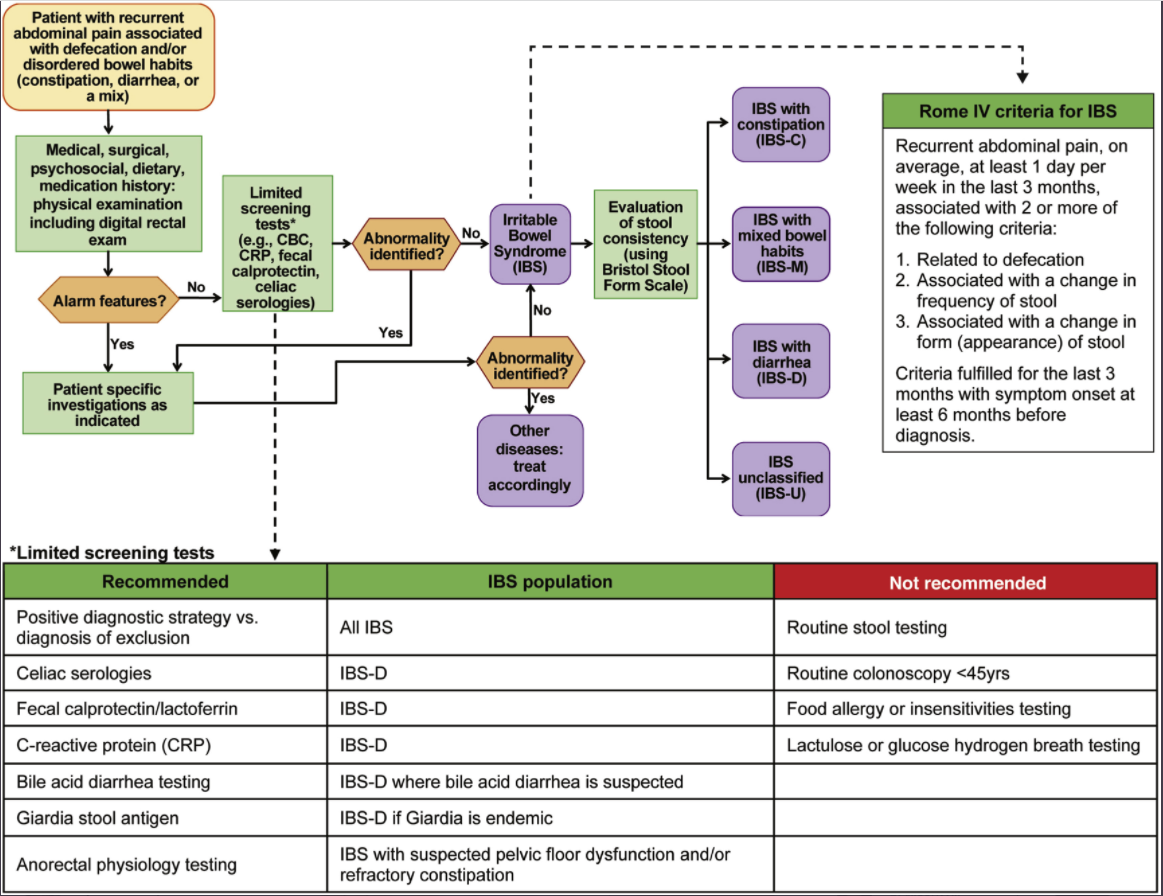
For a short article, this review provides a lot of practical advice. Challenges with IBS include the lack of objective biomarkers and “patients are often dissatisfied with a positive diagnostic approach or even after multiple negative tests.” The author recommends the following:
Confidently communicate the diagnosis of IBS
Explain visceral hypersensitivity and its associated with pain, and bloating and why central neuromodulators and behavioral therapy are often used. Explain that IBS can be associated with high-amplitude propagating contractures which can cause pain/diarrhea
Treatment focused on ‘RESET’ =Relationship with patient-provider, Education/reassurance, Symptom assessment, Exacerbating/alleviating factors, and Targeting treatment (see Table 1)
Treatment may need to target gut, brain and/or both
Dietary treatments considered 1st line approach
Treatment pharmacology options for IBS-D include antidiarrheals, antispasmotics, rifaximin, eluxadoline, alosetron (rarely, can cause ischemic colitis), bile acid sequestrants
Treatment pharmacology options for IBS-C include polyethylene glycol, lubiprostone, linaclotide, plecanatide, and tegaserod (restricted to women <65 yrs w/o cardiovascular dz)
Treatment pharmacology options for all IBS include TCAs (start with low dose and can titrate upwards; amitriptyline for IBS-C, nortriptyline or desipramine for IBS-M or IBS-C), SNRI (eg. duloxetine (may be better than TCAs in patients with IBS-C and comorbidities like fibromyalgia and depression), mirtazapine (small studies demonstrated benefit for IBS-D and functional dyspepsia), SSRIs (“consider…in patients with predominant anxiety and/or depression…advise against its use as primary treatment for IBS w/o comorbid psychological disorder”), delta ligand agent (eg. pregabalin) (consider if refractory to other treatments), and brain-gut therapies (eg. CBT, GDH)
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Carvedilol (not approved in children) is a NSBB that has additional α1 adrenergic blocking activity that enhances the portal pressure–reducing effect, compared to other NSBBs (eg. nadolol, propranolol).
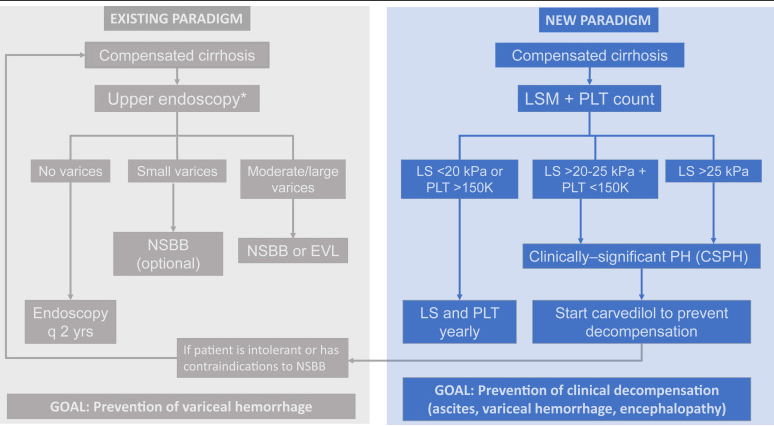
New paradigm focuses on “the most relevant end point in compensated cirrhosis…development of decompensation” (ascites, variceal hemorrhage, and/or hepatic encephalopathy).
In the PREDESCI study with 201 patients with compensated cirrhosis and CSPH, with no or small varices, to NSBBs or placebo…”clinical decompensation, was significantly lower in the NSBB arm than in the placebo arm (from 27% to 17% over a median follow-up of 37 months: HR 0.51, 95% CI 0.26–0.97)”
This model favors carvedilol over endoscopic variceal ligation; the “only RCT of carvedilol vs EVL in the prevention of first variceal hemorrhage showed a survival benefit of carvedilol over EVL.” Carvediol has been associated with improved survival in patients with cirrhosis (McDowell H.R. et al. Carvedilol is associated with improved survival in patients with cirrhosis: a long-term follow-up study. Aliment Pharmacol Ther. 2021; 5: 531-539)
This model “consists of identifying those with CSPH (by means of noninvasive methods) and treating them with carvedilol, with the goal of preventing any decompensating event (not only variceal hemorrhage).”
Screening endoscopy would still be recommended in newly-diagnosed decompensated cirrhosis and those intolerant to NSBBs.
My take: This new paradigm is one approach for portal hypertension in adults. More studies are needed in the pediatric age group to help determine whether medical therapy can obviate the need for EVL in most children with cirrhosis.
“Whereas the existing paradigm focuses on the use of NSBBs for the prevention of variceal bleeding, in the new paradigm the presence of CSPH [clinically significant portal hypertension ](determined noninvasively) establishes the indication for NSBBs with the goal of preventing cirrhosis decompensation. CSPH, clinically significant portal hypertension; EVL, endoscopic variceal ligation; NSBB, nonselective beta-blocker; LS, liver stiffness; PLT, platelet count. ∗Patients with LS <20 kPa and PLT >150,000/mm3 can circumvent endoscopy because the risk of having high-risk varices is minimal“
Related blog posts:
#NASPGHAN19 Liver Symposium (excellent presentation by Dr. Romero on varices in children and portal hypertension)
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
In this review, the authors propose expanding treatment indications for chronic hepatitis B virus (HBV).
The authors review current guidelines (Table 2 lists the major society recommendations). For example, the AASLD recommends HBV treatment for the following:
Antiviral treatment in all patients with cirrhosis and detectable viremia, independent of alanine aminotransferase (ALT) or HBV DNA levels
For patients without cirrhosis, all guidelines recommend treatment in patients with immune active disease; treatment is mainly with a NA (nucleos(t)ide analog) until 1 year after confirmed HBeAg seroconversion for patients who were HBeAg-positive and until HBsAg loss for patients who were HBeAg-negative at the start of treatment
AASLD cut-offs for distinguishing immune active disease: ALT ≥2× ULN or evidence of significant histologic disease and HBV DNA >20,000 IU/mL for HBeAg (+) and >2000 IU/mL for HBeAg (–)
Why Expand Treatment Indications?
The main reason for advocating treatment of patients in the immune tolerant phase is the mounting evidence that persistently high viremia and persistent presence of HBeAg are associated with increased risk of cirrhosis, HCC, and liver-related mortality…In one study of 438 HBeAg-positive patients, the 15-year cumulative risk of cirrhosis and HCC increased from 3.7% and 2.1% in patients who seroconverted before age 30 to 12.9% and 3.2% in those who seroconverted between ages 30 and 40 and 42.9% and 7.7% in those who did so after age 40
Why Not Treat All Patients with Chronic Hepatitis B?
“An important reason for deferring treatment of patients in the immune tolerant phase is that spontaneous HBeAg and HBsAg clearance with remission of liver disease can occur.” This happens in 80% or more over 10-20 years.
Who Else Should Receive Treatment (Beyond Guidelines)?
“Available data support expanding treatment to immune tolerant patients and patients in the grey zones who have evidence of active/advanced liver disease based on liver biopsy or non-invasive tests and those who remain in the immune tolerant phase after age 40. Evidence supporting treatment expansion to confirmed inactive carriers and other immune tolerant patients is lacking.” “Grey zones” indicate that “the course of chronic HBV infection is characterized by fluctuations in HBV DNA and ALT levels, and many patients will be in the grey zone at some point.”
My take: Given the safety/tolerability of newer HBV treatments, these recommendations make sense. If/when HBV treatments improve further (higher loss of HBsAg or HBV DNA), then even more widespread use of HBV treatments would be worthwhile.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
This study, using a rat animal model, demonstrated how gastro-resistant mixed micelles (MMs) could be used to overcome the limitations of current prophylactic vitamin K formulations which are associated with failures in newborns with unrecognized cholestatic liver diseases (1:2,500 live births).
Key findings:
Under cholestatic conditions, gastro-resistant formulations greatly improved vitamin K absorption.
Pathophysiology: “Our data provide an explanation why: unstabilized MMs will aggregate during gastric passage, once aggregated vitamin K will not be sufficiently resolubilized upon a subsequent pH increase”
My take: It is likely that these gastro-resistant MMs would be effective in pediatric patients. If proven in clinical trials, this would reduce bleeding events in infants and lower bleeding risks in those with chronic liver disease while obviating the need for parenteral Vitamin K.
My take: The need for a gastrostomy for nutritional support is associated with more severe CDH (~1/3rd of patients). Over a third of patients who received a GT, no longer needed a GT at a median of 26 months.