In this retrospective study with 218 inpatient pediatric patients with active ulcerative colitis, the key findings:
Use of enoxaparin did not result in a greater fall in hemoglobin among those with acute severe colitis (initial PUCAI ≥65) during the week following admission and there was not an increased risk of needing a transfusion
VTE occurred in 2 of 130 in control group and 1 of 88 in enoxaparin group (enoxaparin group was sicker)
My take: The absolute risk of VTE is low in the pediatric population. This study shows that enoxaparin prophylaxis is NOT associated with increased issues with blood loss. In those with active disease, the presence of CVC and use of steroids are known risk factors and require consideration of, at minimum, nonpharmacologic interventions.
This article is a large retrospective single-center (Boston Children’s) review of laparoscopic gastrostomy (LAP, n=545) compared to percutaneous endoscopic gastrostomy (PEG, n=545) (2010-2015). The authors note a shift in attitude in their institution in favor LAP due to perceived safety advantages (citing references 14-16 -reviewed below).
Key findings:
Total complication rate: 33% (146) in PEG group, 36% (197) in LAP group; cellulitis reported in 18% in PEG group compared with 10% of LAP group
ED visits: 89% (394) of PEG group had zero ED visits compared with 84% of LAP patients; In PEG group, 9% and 1% had one ED visit and two ED visits respectively compared to 15% and 1% in LAP group
In the early postoperative period (first week), patients undergoing PEG placement had more gastrostomy-related complications (PEG 30 [6.7%] vs LAP 13 [2.4%], P = 0.0007) and cellulitis (PEG 23 [5.1%] vs LAP 2 [0.4%], P = 0.03). Complications included postoperative pain, leakage, tube dislodgement, and stoma erythema
The authors reported higher total costs and operative time for LAP compared to PEG but note that in their institution, total cost may be higher for PEG due to frequent need for 2nd procedure for placement of a skin level device
In the discussion, the authors acknowledge that in their institution, “no differences in total complication rates within the first 6 months were seen.” My view is that the difference in cellulitis needs to interpreted cautiously in a retrospective study. The swelling and erythema around a PEG site in the first days postoperatively can be difficult to determine conclusively if there is cellulitis. With regard to potential cost advantages of LAP, this is affected in the PEG group by whether changing to a skin level device is done at the time of another procedure and whether the case is done in an outpatient surgery center where costs are lower.
My take: There is likely a lower rate of visceral perforation among children who have LAP placement over PEG placement. However, overall, it is uncertain if the complication rate from LAP placement is lower than PEG placement.
Review of some of the cited studies from this article:
F Sandberg et al. Pediatr Surg Int. 2018; 34 (12):1321-1327. Comparison of major complications in children after laparoscopy-assisted gastrostomy and percutaneous endoscopic gastrostomy placement: a meta-analysis While this meta-analysis with eight studies (n=1500 patients) found a lower risk of complications with LAP compared to PEG, the authors note that “there were no randomized-controlled trials. Overall, the quality of the included studies was determined to be unsatisfactory.” In addition, the results were heavily influenced by one study which reported 20 major complications (death or reoperation within 30 days) among 134 PEG patients.
L Baker et al.J Pediatr Surg 2015; 50: 718-725. A systematic review and meta-analysis of gastrostomy insertion techniques in children In this study, the authors examined 22 studies with 5438 patients that met inclusion criteria. No differences in major complications were noted in studies comparing open versus laparoscopic approaches or open versus PEG. Then, in a subset 10 studies (n=1599 laparoscopic, n=1161 PEG), the authors state that laparoscopic gastrostomy and PEG revealed a significantly increased risk in major complications with PEG (OR 0.29, 95% CI: 0.17–0.51, p < 0.0001). In this study, the most striking difference were 20 cases of visceral perforation with PEG and one case with LAP. Again, the data are limited by the retrospective nature of all but one study. This “suggest that individual-specific and/or institutional-specific factors likely influence outcomes and diminish the generalizability of the presented results.” Cited advantages of LAP: better visualization of site, ability to transfix stomach to abdominal wall, and ability to place primary button.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
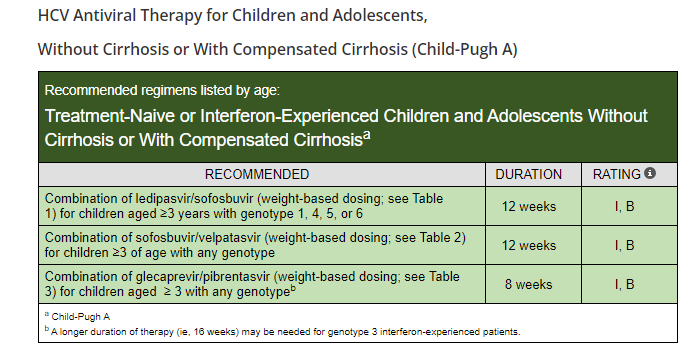
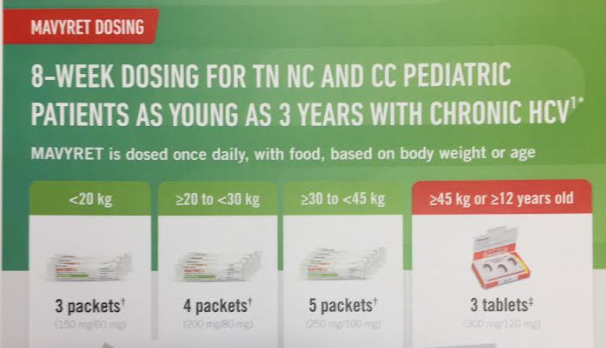
“The Food and Drug Administration (FDA) has approved Epclusa (sofosbuvir and velpatasvir) and Mavyret (glecaprevir and pibrentasvir) for treatment of chronic hepatitis C virus (HCV) infection in pediatric patients as young as 3 years. These products are the first all-oral, pan-genotypic (genotypes 1-6) HCV treatment regimens for pediatric patients 3 years and older…Both products are available as oral tablets and as newly approved oral pellets in dosing strengths suitable to accommodate the recommended weight-based dosing in pediatric patients.”
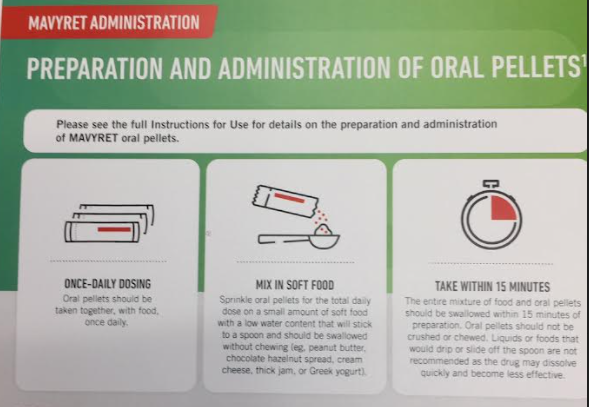
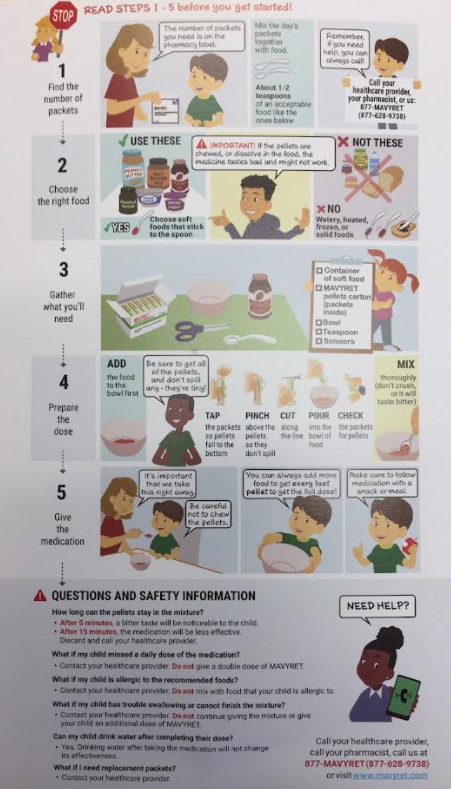
The following images are from Abbvie patient-provider handouts. I do not receive any funding from any pharmaceutical company but think these instructions are useful.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
In this open-label trial of adults with mild-to-moderate biologic naive Crohn’s disease, key findings:
At week 6, 13 (68%) of 19 patients in the CDED plus partial enteral nutrition group and 12 (57%) of 21 patients in the CDED group had achieved clinical remission (p=0·4618)
Among the 25 patients in remission at week 6, 20 (80%) were in sustained remission at week 24 (12 patients in the CDED plus partial enteral nutrition group and eight in the CDED alone group)
14 (35%) of 40 patients were in endoscopic remission at week 24 (eight patients in the CDED plus partial enteral nutrition group and six in the CDED alone group)
My take: Dietary therapy may be effective option for motivated adult patients with Crohn’s disease.
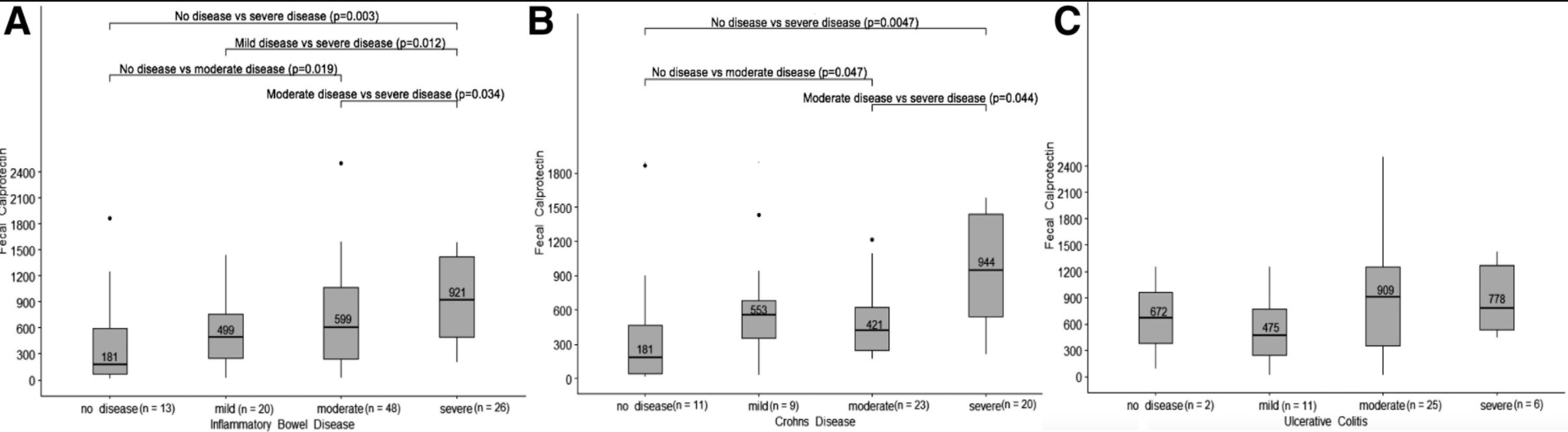
This retrospective study used data from 331 patients (n=107 with IBD). Fecal calprotectin (FC) was done between 30 days and 1 day before colonoscopy.
Key findings:
Correlation with endoscopy: median FC was lowest for all IBD patients with no active disease (181 μg/g) and highest in severe disease (921 μg/g), with significant difference between no disease and moderate and severe disease (P = 0.019, 0.003), and between mild and severe disease (P = 0.012)
Correlation with histology: median FC was lowest with no active disease (328 μg/g) and highest in severe disease (895 μg/g), with significant difference between no disease and moderate and severe disease (P = 0.021, 0.018)
The control population had median FC of 35.5 compared to 181 μg/g for the IBD population in endoscopic remission (P = 0.018).
My take: Calprotectin levels are particularly helpful as a screen for IBD (probably using threshold of at least 120) and its use to monitor clinical response. This study shows it has some utility in predicting disease severity.
Figure 1: Fecal calprotectin association with endoscopic disease severity of IBD (A), Crohn’s disease (B) and ulcerative colitis (C). IBD = inflammatory bowel disease.
“When faced with someone in a white coat, don’t go mute. Assert yourself, particularly if you’re confused. Try repeating what you’re hearing”
“People recalled less than half of what their doctors told them a week earlier”
”In practice, though, patients bring up as many as 15 different issues during a visit. Show up with a list of the three main things you want to talk about, and go over all three before your doctor starts talking.”
“Communication onus should be on medical providers. Still, as a patient, you have agency. ‘When people participate, they remember better'”
My take: This article makes some good points. I think in this era, more written information (after visit instructions) are being provided which helps as well.
In this retrospective study, the authors examined recurrent PSC (rPSC) in children who had undergone liver transplantation (LT) with 3 yrs of median followup. Key findings:
rPSC occurred in 36 children, representing 10% and 27% of the subjects at 2 years and 5 years following LT, respectively
Subjects with rPSC were younger at LT (12.9 vs. 16.2 years), had faster progression from PSC diagnosis to LT (2.5 vs. 4.1 years), and had higher alanine aminotransferase (112 vs. 66 IU/L) at LT (all P < 0.01)
After LT, rPSC subjects had more episodes of biopsy-proved acute rejection (mean 3 vs. 1; P < 0.001), and higher prevalence of steroid-refractory rejection (41% vs. 20%; P = 0.04)
My take: rPSC, not surprisingly, was associated with a more agressive, immunoreactive phenotype prior to LT characterized by younger age, faster progression to end-stage liver disease, higher prevalence of IBD and more frequent/difficult allograft rejection
Related blog posts:
PSC -Aspen 2021 Webinar This lecture highlights studies show lack of efficacy with vancomycin, ursodeoxycholic acid and vedolizumab. Also, there is potential utility of MMP-7 for distinguishing between PSC and AIH
Recently, Carlo DiLorenzo came to Atlanta as the speaker for the William Meyers Lectureship. He provided a terrific talk and was the perfect speaker for this lectureship which honors Billy.
Some of the key points:
When giving a lecture, often ‘a great study is one that supports the speaker’s view’
Physicians often have biases against patients with functional disorders as compared to those who have “rightful” suffering (eg. cancer, pancreatitis)
Key part of patient-physician relationship is listening (by the physician). Patients report better satisfaction and perceive to be understood better when a physician is sitting (while listening). “The most important technological advance in the practice of medicine was the invention of the chair. For you to sit in. While you take the history” (Mark Reid, MD)
Diagnoses have side effects
Families remember our words for years
We are not well-equipped to deliver good news: “This is one of the best colons I have ever seen…Your child has irritable bowel and no other tests are needed.”
The most under prescribed treatment: 30 minutes of physical activity everyday
2nd most under prescribed treatment is a good night’s sleep. Increased symptoms when tired
“Psychobezoar,” referring to a fear of discomfort with eating, could be used as an alternative to ARFID
Most effective treatment for IBS: cognitive behavioral therapy
Distraction is helpful tool for pain but need to teach parents to accept this tool
Some of the axioms in the lecture are attributed to Mark Reid, MD