It appears that the Mediterranean diet works as well as the specific carbohydrate diet for adults with Crohn’s disease.
A Randomized Trial Comparing the Specific Carbohydrate Diet to a Mediterranean Diet in Adults with Crohn’s Disease (in press -thanks to Kipp Ellsworth for this reference) JD Lewis et al. Gastroenterol 2021; https://doi.org/10.1053/j.gastro.2021.05.047
Abstract:
Background & Aims
This study compared the effectiveness of the Specific Carbohydrate Diet (SCD) to the Mediterranean Diet (MD) as treatment for Crohn’s disease (CD) with mild to moderate symptoms.
Methods
Adult patients with CD and with mild-moderate symptoms were randomly assigned 1:1 to consume the MD or SCD for 12 weeks. For the first 6-weeks, participants received prepared meals and snacks according to their assigned diet. After 6-weeks, participants were instructed to follow the diet independently. The primary outcome was symptomatic remission at week 6. Key secondary outcomes at week 6 included: fecal calprotectin (FC) response (FC <250 μg/g and reduction by >50% among those with baseline FC >250 μg/g) and C-Reactive Protein (CRP) response (high-sensitivity CRP (hsCRP) <5 mg/L and >50% reduction from baseline among those with hsCRP >5mg/L).
Results
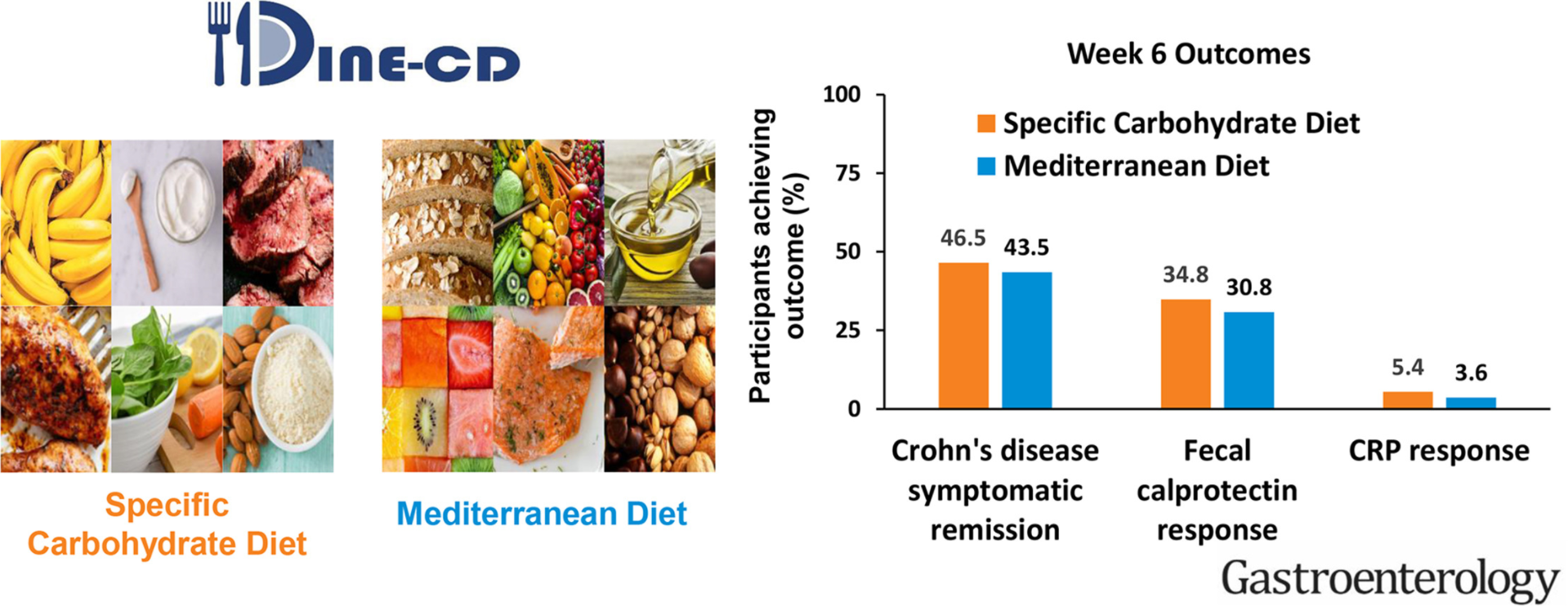
194 patients were randomized, and 191 were included in the efficacy analyses. The percentage of participants who achieved symptomatic remission at week 6 was not superior with SCD (SCD 46.5%, MD 43.5%; P = .77). FC response was achieved in 8/23 participants (34.8%) with SCD and 4/13 participants (30.8%) with MD (P = .83). CRP response was achieved in 2/37 participants (5.4%) with SCD and 1/28 participant (3.6%) with MD (P = .68).
Conclusions
SCD was not superior to MD to achieve symptomatic remission, FC response and CRP response. CRP response was uncommon. Given these results, the greater ease of following the MD, and other health benefits associated with MD, the MD may be preferred to the SCD for most patients with CD with mild to moderate symptoms.
Related blog post:
- Trial by Diet Approach for Crohn’s disease in children (this blog post has link to 16 other dietary therapy posts)