Background: “Measles is a highly contagious disease and, despite the availability of a safe and effective vaccine, remains still an important cause of childhood death worldwide [1,2]. The risk of severe illness in measles-naive individuals is particularly high in immunocompromised patients with inflammatory bowel disease (IBD) or after liver transplantation (LT) [3]…Ideally, vaccination with live attenuated vaccines (LAVVs) should be completed four weeks before organ transplantation or the initiation of immunosuppressive therapy (IST) to allow for the live vaccine’s incubation period and minimize the risk of vaccine-associated disease…LAVVs are considered contraindicated during IST due to safety concerns and limited experience.”
Methods: “In this prospective multicenter observational study (DRKS00014569) 22 children and adolescents with incomplete MMR vaccination status were identified… with stable immunosuppressive therapy in the last three months with no evidence of underlying disease activity…Sixteen patients were vaccinated against MMR, eleven after liver transplantation and five with inflammatory bowel disease. At the time of vaccination, four patients were receiving moderate (e.g., tacrolimus drug level below 5 ng/ml), eleven were receiving high-intensity immunosuppression (e.g. anti-tumor-necrosis factor agents, mycophenolate mofetil) and one child had previously discontinued immunosuppressive treatment.”
Immediately prior to the references, the authors provide a downloadable document detailing how they chose to categorize the degree of immunosuppression and their precise protocol, including immunologic pretesting and drug contraindications as noted below.
Key findings:
There were no serious adverse events or complications related to the vaccination
In children receiving immunosuppressive medications, the seroconversion rate for measles after the first MMR vaccination was 73.3 % (11/15) and after the second vaccination 80 % (12/15)
My take: In carefully-selected immunocompromised pediatric patients, the MMR vaccine may be safe. However, given the small numbers receiving vaccination in this study, the absolute safety is unclear. Even infrequent adverse effects would be problematic. This study’s protocol could be helpful for those considering vaccination in immunocompromised populations with a measles epidemic. For now, the most important approach is improving vaccination rates in those (especially family members) without contraindications.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
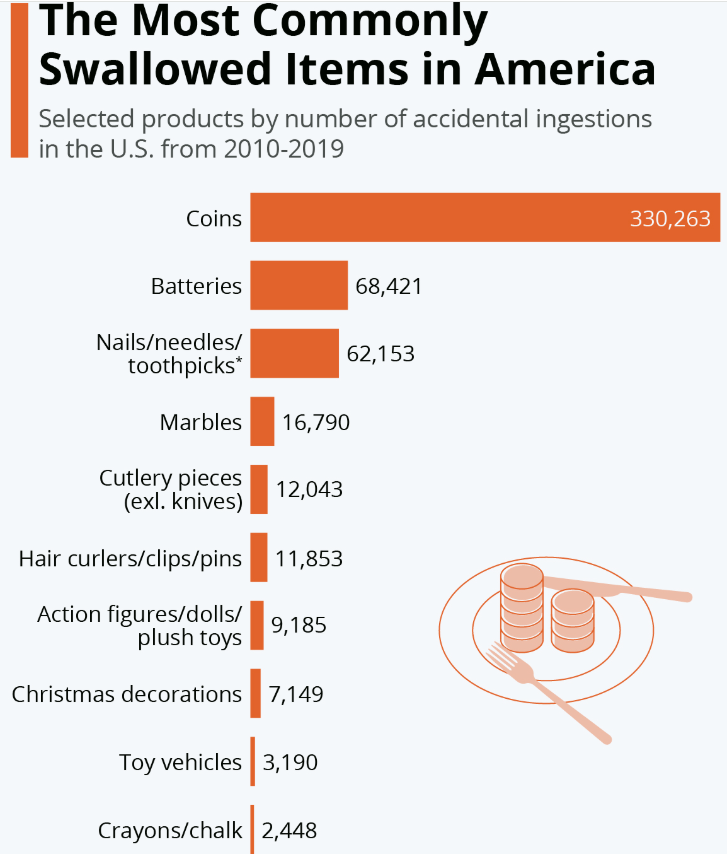
As I noted in a blog in 2012, I had advocated for removal of the penny due to frequent ingestions (starting more than 20 years ago) (link: “Watch for change in the stools”). Now it appears I will finally get my wish.
In recent weeks, Republican and Democratic lawmakers introduced separate bills in the House of Representatives and the Senate calling for an end to penny production. The change means that businesses will have to start rounding the prices of cash transactions up or down to the nearest five-cent nickel as the number of pennies in circulation dwindles.
The Treasury’s penny phase-out plan was first reported by the Wall Street Journal…The cost of producing the penny has risen from 1.3 cents per coin to 3.69 cents over the past 10 years, according to the Treasury. It said stopping production will lead to immediate annual savings of $56 million.The penny was first issued by the government in 1793
The following statistic will delight fans of obscure facts and overbearing bureaucracy: According to the U.S. Consumer Product Safety Commission, more than 850,000 accidental ingestions of everyday objects were recorded in the U.S. between 2010 and 2019. ..Coins topped the list of accidental ingestions, with around 33,000 being recorded each year (more might go unreported).
My take: While this is a step in the right direction, there are still 114 billion pennies currently in circulation in the U.S. according to the Reuters article. Perhaps, other coins will be ingested less in the coming years too as so many business transactions are via smartphones and credit cards.
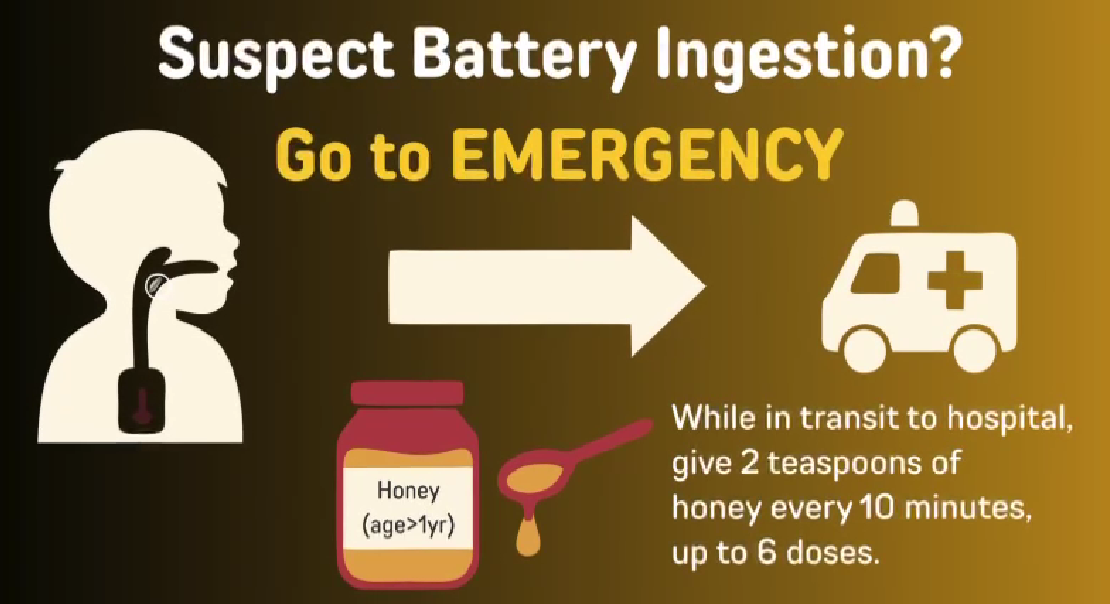
Button batteries are a much more serious ingestion than a coin. For World Button Battery Day, here’s a link to a 3 minute video from FISPGHAN. FISPGHAN Button Battery Video
The video provides a simple explanation of the problem though at times it is not certain who the target audience is. Particularly the first part feels like a video for kids rather than for parents. Thanks to Ben Gold for sharing this link.
Mitigation Efforts for Button Batteries (also includes case report of aorto-esophageal fistula and emergency surgery 25 days after ingestion of a button battery)
Background: “Current guidelines recommend treating all children aged 3 years or older with DAAs (direct-acting antivirals). These treatments achieve cure in more than 98% of HCV cases and reduce risks for cirrhosis, hepatocellular carcinoma (HCC), and liver-related mortality. Despite availability of DAAs, only 62% of adults with HCV have linked to care, 39% initiated treatment, and 26% attained cure (sustained virologic response) as of 2023.”
Methods: This retrospective cohort analysis included children born between 2000 and 2018 who were diagnosed with HCV between the ages of 0 and 18 years. The study analyzed TriNetX Research Network data, a US national electronic health records network with more than 87 million individuals within the U.S.
Key findings:
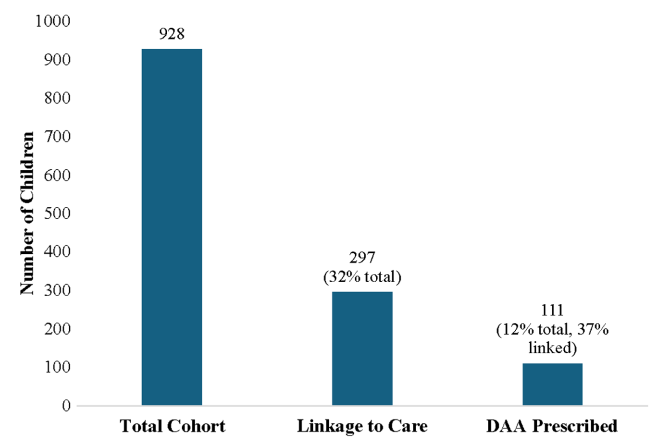
Among 928 children with HCV, 297 (32.0%) linked to HCV care and 111 (12.0%) were prescribed a DAA (direct-acting antiviral). Thus only 1 in 8 children with HCV were prescribed DAAs
Of 928 children with HCV, 35.9% of children were diagnosed with HCV perinatally (by 3 years old), 44.5% during childhood (between 4 and 12 years old), and 19.6% in adolescence (between 13 and 18 years old)
White and Hispanic/Latinx children were much more likely than black children to receive a DAA prescription with OR of 3.44 and 2.20 respectively
Children in Midwest, North, and West had higher rights of DAA prescription compared to the South with OR of 2.40, 1.50, and 4.19 respectively
Discussion points:
Potential barriers to treatment:
DAAs were only approved for children aged 3 years or older in 2019 for some genotypes and not until 2021 for all genotypes.
Some parents choose to wait to treat young children because of difficulty administering medications at the ages of 3 and 4 years old
Insurance: “The cause of low uptake of treatment is likely multifactorial: Medicaid and commercial insurers implemented restrictions based on degree of liver fibrosis, active or recent substance use, or specialty prescribing because of the very high initial cost of DAAs. Although most of these restrictions have now been removed, some still remain, and some insurance plans have varying criteria for pregnant or pediatric members.”
New CDC Recommendations: “In light of the new Centers for Disease Control and Prevention perinatal HCV testing recommendations and universal HCV screening recommended in pregnancy, more young children with HCV will be identified”
Limitations: Retrospective study relies on data from a database
My take: Being able to cure HCV with DAAs has been an incredible medical achievement. However, efforts to eradicate HCV have not gotten very far and had a severe setback with the opioid epidemic which increased rates of HCV. This study shows that very few children with HCV actually receive curative treatment. Advancing the goal of HCV elimination will require sustained efforts to get those identified with HCV to treatment, both in children and adults.
“The prevalence of HCV in pregnant people jumped 16-fold between 1998 and 2018 to 5.3 cases per every 1000 pregnancies, and these patients can transmit the disease perinatally. Many people are unaware they are infected.”
“More than half of children clear the infection on their own by age 3, the age at which treatment can also begin”
Health Secretary Robert F. Kennedy Jr. on Monday removed every member of a scientific committee that advises the Centers for Disease Control and Prevention on how to use vaccines and pledged to replace them with his own picks.
Major physicians and public health groups criticized the move to oust all 17 members of the Advisory Committee on Immunization Practices… Kennedy wrote in a Wall Street Journal opinion piece. “A clean sweep is needed to re-establish public confidence in vaccine science…”
Kennedy is going against what he told lawmakers and the public…Kennedy’s move, coupled with declining vaccination rates across the country, will help drive an increase in vaccine-preventable diseases…
Republican Sen. Bill Cassidy of Louisiana, a doctor who had expressed reservations about Kennedy’s nomination but voted to install him as the nation’s health secretary nonetheless, said he had spoken with Kennedy moments after the announcement.
“Of course, now the fear is that the ACIP will be filled up with people who know nothing about vaccines except suspicion,” Cassidy said in a social media post. “I’ve just spoken with Secretary Kennedy, and I’ll continue to talk with him to ensure this is not the case.”
RFK Jr alleges ACIP committee members are laden with conflicts of interest as the rationale for this move; however, his editorial lists little evidence of this. Just last month, HHS leaders announced that COVID vaccination was no longer recommend for pregnant women; these women and their infants in the first 6 months of life are at increased risk of COIVD deaths and complications. The pattern of undermining expertise in utilizing vaccines will have far-reaching repercussions. Unfortunately, the trajectory for public health is even more worrisome. It is likely that there will be more measures to limit vaccine availability. Though, it will be a while until the full body count will be determined.
My take: Senator Cassidy, a physician, allowed RFK Jr to lead HHS despite misgivings; this was due to political considerations rather than qualifications. This decision and his lack of action to hold him accountable are a true betrayal of his constituents and to the principle of ‘Do No Harm.’
It is funny that the city of Roswell highlights an award for excellence in park and recreation management on a trashcan. This type of honor, though, could be replicated for the work of the current HHS secretary.
Background: “Hemangiomas remain the most common tumor of the liver in newborns and infants…A subtype classification system for hepatic hemangioma (HH) was first proposed based on our Liver Hemangioma Registry in 2007, delineating focal, multifocal, and diffuse HH…Focal hepatic lesions correspond to congenital hemangiomas whereas multifocal and diffuse lesions represent infantile hemangiomas.”
Methods: This was a retrospective review of 96 infants over an 18 year period (2004-2022). Patients with infantile HH were excluded.
Key Findings:
32% were diagnosed prenatally, 23% developed heart failure, and 23% developed respiratory failure
There was a balanced sex distribution (50% for each gender)
Common clinical features included transient anemia (n = 23/48, 48%) and thrombocytopenia (n = 30/53, 57%).
On average, patients demonstrated 43% residual HH volume at 12 months and 16% residual volume at 24 months
No difference in time to 50% HH volume reduction between patients with and without medical therapy was observed
Larger hemangioma volumes were associated with an increased risk of anemia (P = .005) and thrombocytopenia (P < .001)
There was not a significant association between HH volume and congestive heart failure (CHF) or cardiomegaly. For example, the HH volume was 824 mL vs 579 mL (P=0.689) in those with and without CHF, respectively
Discussion Points:
“Congenital HH is present at birth and typically does not undergo postnatal growth”
“Congenital HH occurs equally in males and females and is immunonegative for GLUT-1. This stands in contrast to infantile hepatic and cutaneous hemangioma, which exhibits an early proliferative phase followed by gradual involution”
“HH size at diagnosis was associated with respiratory failure but not with the development of cardiomegaly or CHF, suggesting intralesional shunting may not be related to absolute tumor volume. Hence, all HH regardless of size should be assessed for shunting by doppler US”
“We advocate consideration of cross-sectional imaging and/or biopsy if patients with presumed congenital HH do not follow the expected clinical behavior of early signs of involution”
“Although corticosteroids and propranolol have proven benefit for infantile HH, we demonstrate that there was no significant difference in the rate of congenital HH involution between patients who had received medical therapy and those that did not”
“Medical therapy does have a role in the medical management of high-output heart failure occurring secondary to shunting. If refractory to pharmacologic therapy, these patients should undergo embolization of symptomatic intrahepatic shunts”
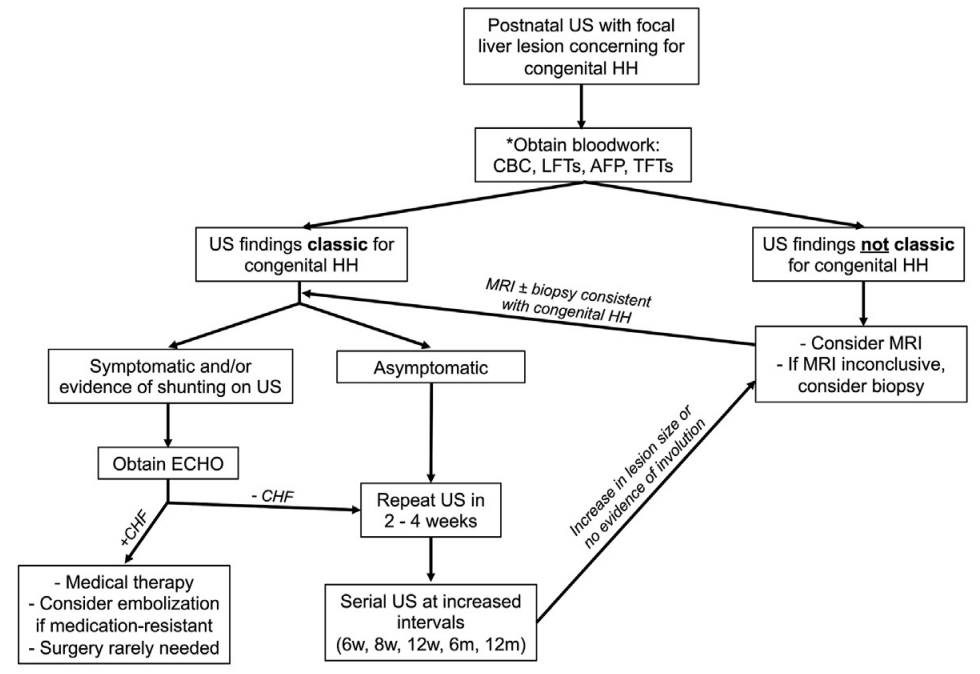
The practice algorithm for evaluation and management of congenital HH suggested by the authors. *Obtain baseline labs and repeat as needed. Repeat CBC if lesion increases in size during monitoring period and there is concern for intralesional bleeding. Repeat AFP as necessary to rule out hepatoblastoma. TFTs indicated if unclear whether congenital HH or infantile HH .
My take: This is a very useful study. It is important to distinguish congenital HH from infantile HH. Even in those with congenital HH, “a subset of patients develop life-threatening complications including respiratory failure and CHF that warrant directed medical management.”
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Methods: U-ACTIVATE is an ongoing, 288-week, phase 3, long-term extension study that enrolled patients (n=369) aged 16–75 years with a confirmed diagnosis of moderately to severely active ulcerative colitis; patients who had a clinical response in the induction studies were eligible to enter the U-ACHIEVE maintenance study. Patients not in clinical remission originally randomly assigned to upadacitinib 15 mg were eligible to escalate to upadacitinib 30 mg, those originally randomly assigned to upadacitinib 30 mg continued on upadacitinib 30 mg, and those originally assigned to placebo were eligible to escalate to upadacitinib 15 mg in a masked way
Key findings:
In the as-observed population, 84 (71%) of 118 patients receiving upadacitinib 15 mg were in clinical remission at week 48, as were 130 (67%) of 193 receiving upadacitinib 30 mg
By week 96, 69 (76%) of 91 patients receiving upadacitinib 15 mg and 104 (74%) of 141 of those receiving upadacitinib 30 mg were in clinical remission
The most common adverse events of special interest were hepatic disorder, lymphopenia, creatine phosphokinase elevation, serious infection, neutropenia, and herpes zoster
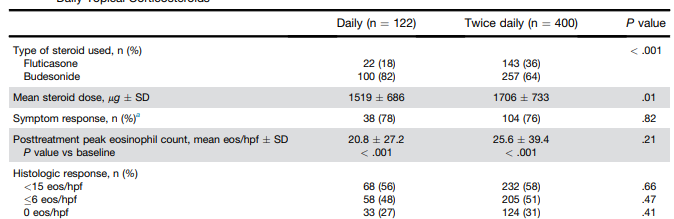
Methods: This was a retrospective cohort study using the UNC EoE Clinicopathologic Database of newly diagnosed patients with EoE treated with a tCS who had a follow-up endoscopy with biopsy. In total, there were 522 patients, including 195 pediatric patients (<18 yr). 122 patients received once daily dosing and 400 patients received twice daily dosing.
At our center, patients are typically treated on a clinical basis with either oral viscous budesonide or fluticasone from a multidose inhaler, with daily doses ranging from 1–2 mg for budesonide and 440–1760 μg for fluticasone based on patient size and at the discretion of the provider.
Key findings:
Global symptomatic response (78% vs 76%; P = .82), posttreatment eosinophil count (20.8 vs 25.6; P = .21), posttreatment EoE Endoscopic Reference Score (2.2 vs 2.2; P = .92), and histologic response (<15 eos/hpf; 56% vs 58%; P = .66) did not differ by dosing frequency
Candida was less frequent with daily dosing (2% vs 8%; P = .04)
My take: This study suggests that once daily dosing can be as effective as twice daily dosing. It may be that the total dose administered may be more important than the frequency. More studies are needed to confirm these results.
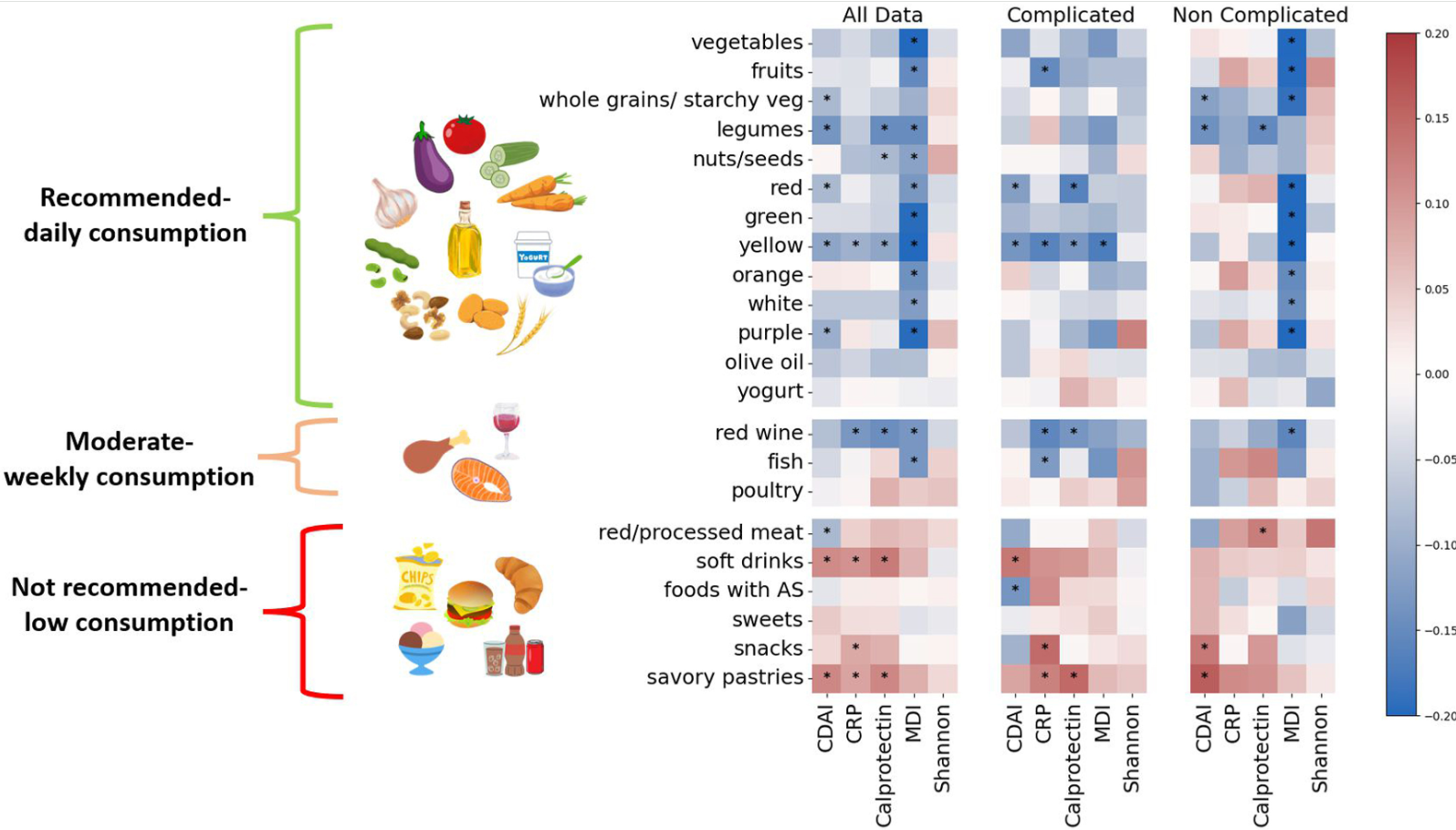
Methods: In this prospective cohort study, consecutive adults (n=271) from 2 large IBD centers in Israel with newly diagnosed CD were recruited and followed prospectively. MED adherence was assessed by repeated food frequency questionnaires (FFQs) using a predefined inflammatory bowel disease Mediterranean diet score (IBDMED score), alongside validated MED adherence screeners. Crohn’s disease activity index (CDAI), C-reactive protein, fecal calprotectin, and microbial composition (16S-ribosomal RNA sequencing) were assessed each visit. Baseline serum and fecal samples were analyzed for targeted quantitative metabolomics.
Demographic/Clinical data indicate 68% received biologics and 40% receiving immunomodulators. 32% received 5-ASA medications (despite lack of proven efficacy)
Key findings:
Adherence to MED was associated with a noncomplicated CD course, and inversely correlated with CDAI, fecal calprotectin, C-reactive protein, and microbial dysbiosis index (all P < .05)
Increasing adherence to MED over time correlated with reduced CDAI and inflammatory markers (P < .05)
Adherence to MED correlated with a beneficial microbial cluster of commensals and short-chain fatty acid producers including Faecalibacterium, and with plant metabolites, vitamin derivatives, and amino acids
Adherence to MED in the cohort group was comparable to the general non-IBD population in Israel
Limitations: This was an observational study rather than an interventional study with a control group. Thus, the results could be influenced by reverse causality
In the associated commentary by Abreu et al, it is noted that in Israel, “MED is more commonplace than in the US and other Western countries…Godny et al found that IBD patients had an average MED adherence score of 7.8, which is similar to that of the general non-IBD population in Israel; in contrast, the average MED adherence score in the US is 4–5.Godny et al’s CD patients consumed an average of 21 g of fiber per day; in a study we just completed, American CD patients consumed less than half that amount.13 Indeed, the baseline diets of American IBD patients are characterized by high amounts of saturated animal fat and almost no fresh fruits and vegetables…Another difference between the Israeli population and the typical American population is body mass index (BMI). The average BMI of patients in this study was 21.9 kg/m2 (interquartile range 20–25.3 kg/m2). This contrasts with the average BMI of the general US population of 30 kg/m2.”
My take: This study shows an association between MED diet and better outcomes/less complications in adults with Crohn’s disease. Eating a good diet is an important part of treatment.
Additional notes on dietary scores: “The IBDMED screener positively scored high consumption of MED-recommended dietary components such as fruits, vegetables, olive oil, legumes, nuts and seeds, and fish. It also positively scored low consumption of MED non-recommended dietary components such as red and processed meat, soft drinks, and sweets. To this we added several dietary features based on previous data associated with microbial composition and function. These included a positive score for plant diversity27 by scoring for different colors in the diet, consumption of fermented foods28 (specifically yogurt), and inclusion of starchy vegetables like potato in the whole grain category to promote diversity in the carbohydrate-rich food group, as well as support butyrate producers as we had previously shown.29 In addition, we aimed to positively score for relatively low UPF intake. To this end, we evaluated the average intake of sweets, snacks, sweet and savory pastries, soft drinks, and foods and drinks containing artificial sweeteners.”
Also, from Kim Beall, Cofounder and Managing Director of Nutritional Therapy for IBD:
“If you haven’t been to the website recently, we have expanded the recipe database to over 1,000 recipes with many filterable aspects and we’ve just released a new nutrition tool, the IBD Nutrition Navigator to facilitate nutrition conversations between providers and patients to find the right nutritional starting point. This is a project led by Dr. Ananthakrishnan and a dedicated team of pediatric and adult medical advisors in a two year long development process. Many have told us this is a useful tool particularly for those less familiar with nutrition in IBD. We’re excited about it’s potential to integrate nutrition in practice, with “an option for every patient”. We appreciate your support in sharing our information, tools, and resources to advance IBD nutrition care.” Here’s the link to their website: