These charts show measles data through April 7th. Some additional data through Apirl 11th is listed below.
For those interested in a deeper dive into the measles numbers, you can follow Caitlin Rivers substack. From her notes on April 11:
“Since my last update on Tuesday, Arkansas and Hawaii reported cases for the first time this year. At least five states have reported ten or more cases, which is very unusual. Texas continues to register the most cases, with 541 to date.”
“According to the CDC, 712 cases have been reported so far this year. 1 in 3 (32%) are under the age of 5, and 1 in 10 (11%) have been hospitalized.”
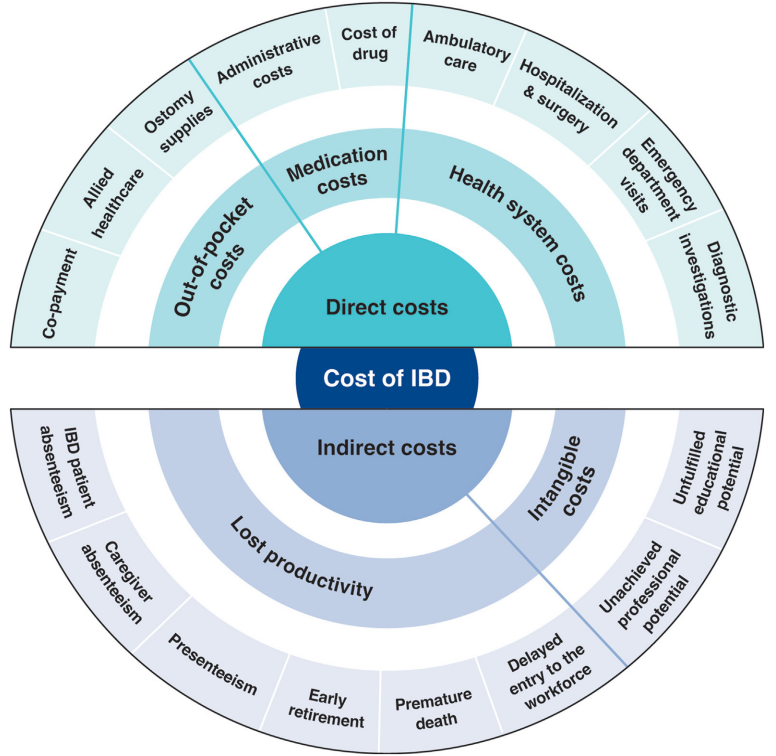
This article is a terrific review of care cost drivers in inflammatory bowel disease (IBD) but it does not actually have useful information on how to make the costs of care sustainable.
Key points:
The most recent data from the United States (U.S.) estimated that the prevalence of IBD was 0.7% of the population, representing 2.39 million individuals living with IBD…the annual cost of IBD in the U.S. approximates $50 billion
All studies demonstrated a shift over time from costs associated with hospitalizations to costs of medications
The costs of prescription drugs for IBD vary significantly worldwide… A particular outlier among high-income countries is the U.S., where manufacturers set prices freely. The lack of nationwide price regulation, coupled with the fragmentation of the U.S. health care system and prolonged market exclusivity periods, result in U.S. drug prices that exceed, on average, international prices by several-fold…Even when insurers are successful at negotiating discounts, patients seldom benefit, as costsharing paid at the point-of-sale is based on the full, non-discounted price
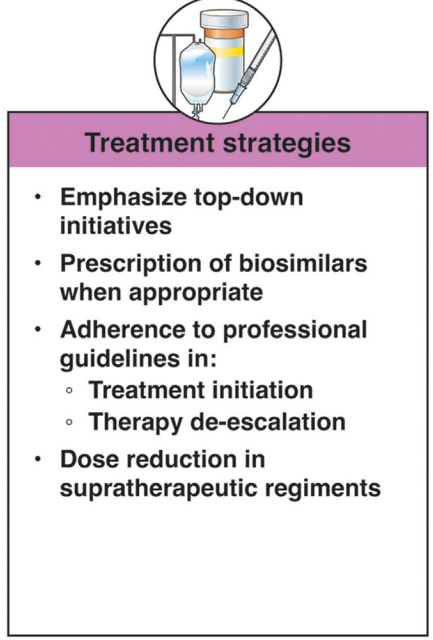
Using a “top-down” clinical paradigm, guidelines suggest starting biologic medications early to induce remission of moderate-to-severe IBD, thereby reducing risk of complications, surgeries, and hospitalizations and improving quality of life.55,58 A randomized controlled trial demonstrated a clear benefit in steroid-free and surgery-free remission among patients randomized to top-down vs step-up care (79% vs 15%; P < .0001) [PROFILE study]
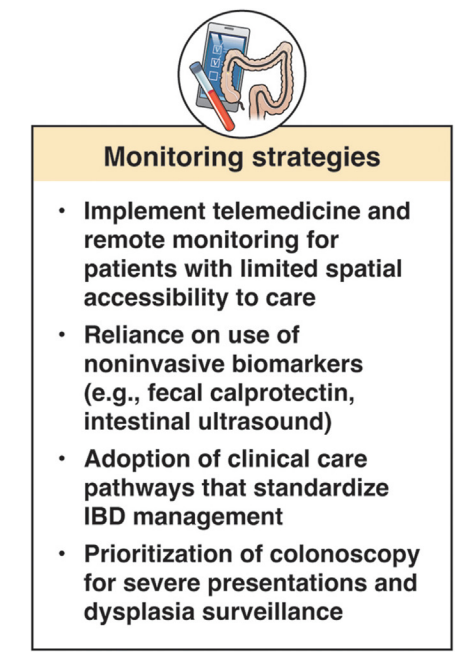
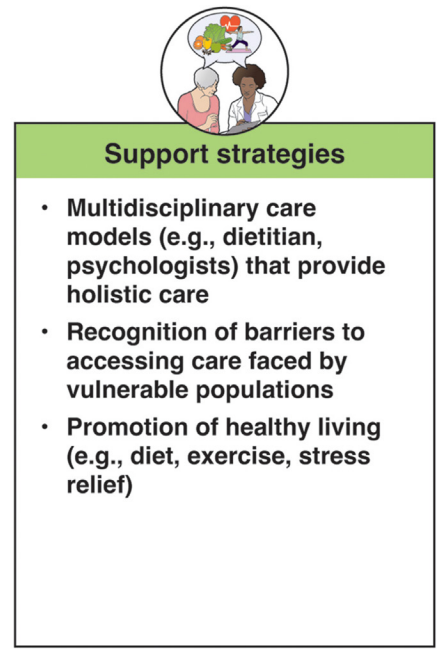
In terms of improving cost sustainability, here is what the authors propose “Strategies for cost reduction in the clinical treatment of IBD”:
My take: This article highlights the cost drivers in IBD but does not identify a path that appears to help address affordability.
This article is one of 11 articles in special issue discussing the future of IBD care.
This retrospective study reviewed adults with Crohn’s disease (CD) who underwent dose intensification of maintenance from 360 mg every 8 weeks to every 6 weeks (n=11) or every 4 weeks (n=11).
Key findings:
Median time to first intensified dose was 228 days
Harvey Bradshaw Index (HBI) improved from a mean of 7.1 to 4.3 after 8 to 16 weeks
There was also improvement (not statistically significant) in mean CRP (1.64–>0.42 mg/dL) and mean calprotectin (774 –>650 mcg/g)
At 8 to 16 weeks, 64% (14 of 22) had a clinical response, 45% (10 of 22) achieved steroid free clinical remission
My take: This small study suggests that the majority of patients with a loss of response to standard dosing can be recaptured with dose intensification.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
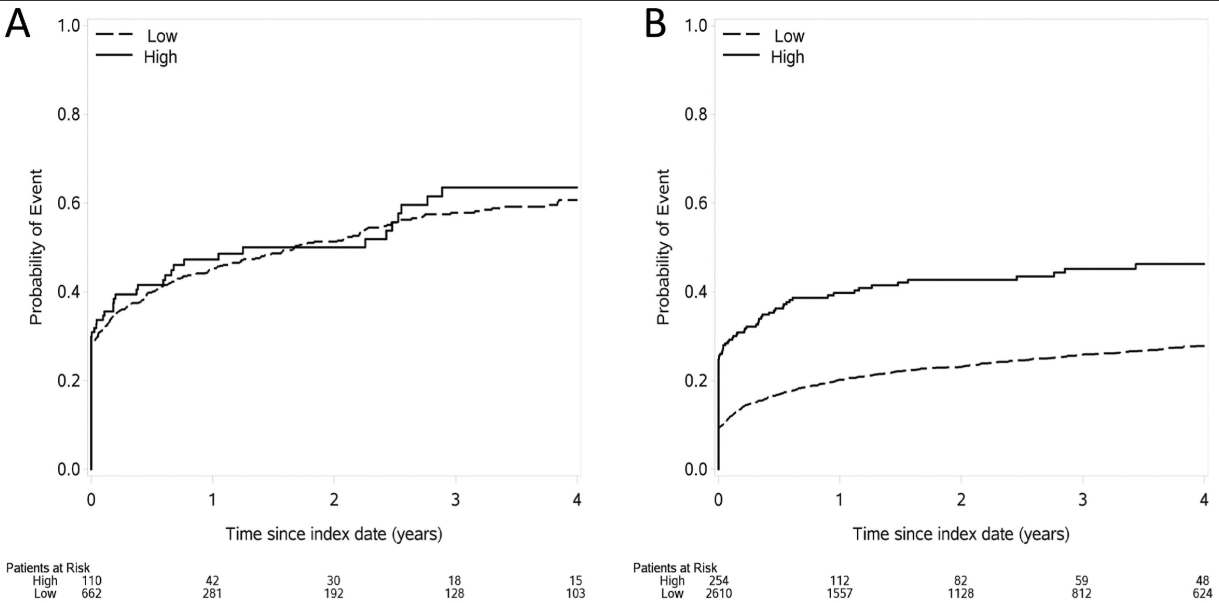
Methods: This was a retrospective cohort of newly diagnosed patients with IBD using data from Optum’s deidentified Clinformatics Data Mart Database (2000–2020). The study included 772 children treated by 493 providers and 2864 adults treated by 2076 providers.
Key findings:
In adults, care from an IBD-focused provider was associated with more use of biologics, combination therapy, and imaging and endoscopy, and less mesalamine use for Crohn’s disease (P < .05 for all comparisons)
In children, none of the associations between provider focus and process or outcome measures were significant. Although not statistically significant among children, the OR for mesalamine use was 0.64, suggesting a similar association as that seen among adults
Time to first dispensing of a biologic therapy in (A) children and (B) adults
My take: This study indicates significant treatment disparities between IBD-focused care providers and providers without an IBD focus in the care for adults, but not in the care of children. This could be related to improved collaboration among pediatric care providers, better training, and parental involvement.
In addition, this study focused on patients with newly-diagnosed disease. Treatment is more complicated in patients who have not responded to initial treatments; as such, IBD-focused providers may be more important in this population.
This was a retrospective study from Vancouver with 332 new diagnosis of eosinophilic esophagitis (EoE).
Key findings:
The incidence of EoE in patients less than 15 years old was 5.4 per 100,000 person‐years
Of the 332 new diagnoses, 40 (12.0%) had endoscopically-identified esophageal narrowing at diagnosis
During follow-up of 1-4 years, 11 (27.5% of narrowed cohort) patients underwent mechanical esophageal dilation
“Our most surprising result was the high number of cases of esophageal narrowing that resolved on follow‐up scope after initiating medical/dietary therapy, without need for mechanical dilation.” The rates of resolution were 1 with 1 (100%) on systemic steroids, 7 out of 13 (54%) with topical steroids, 3 out of 4 (75%) with dietary therapy, and 4 out of 12 (33%) with PPI therapy
My take: This study was a little confusing in how the results are presented. Through most of the article, there are 40 (of 332) children with newly-diagnosed EoE who had narrowing identified. However, there is also discussion of a 65 children subset who had follow-up endoscopy and this is the group in which esophageal narrowing treatment response is reported.
Despite the confusion, the clear take-home message is that esophageal narrowing often responds to medical treatment; only a subset of children with esophageal strictures need mechanical dilatation.
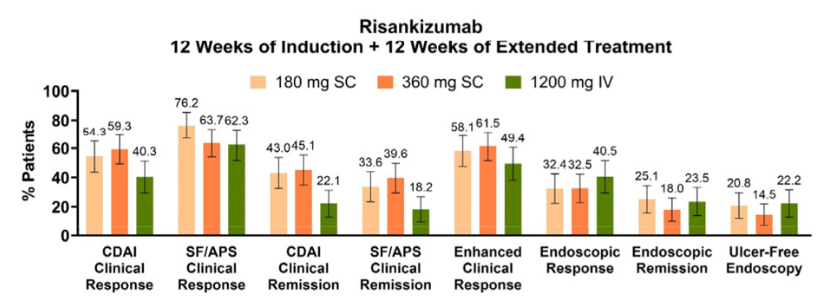
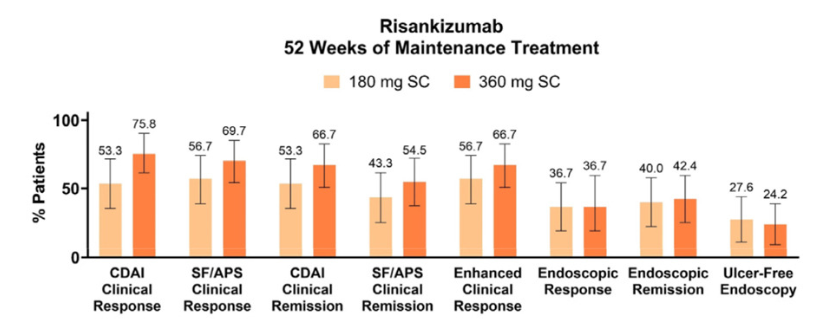
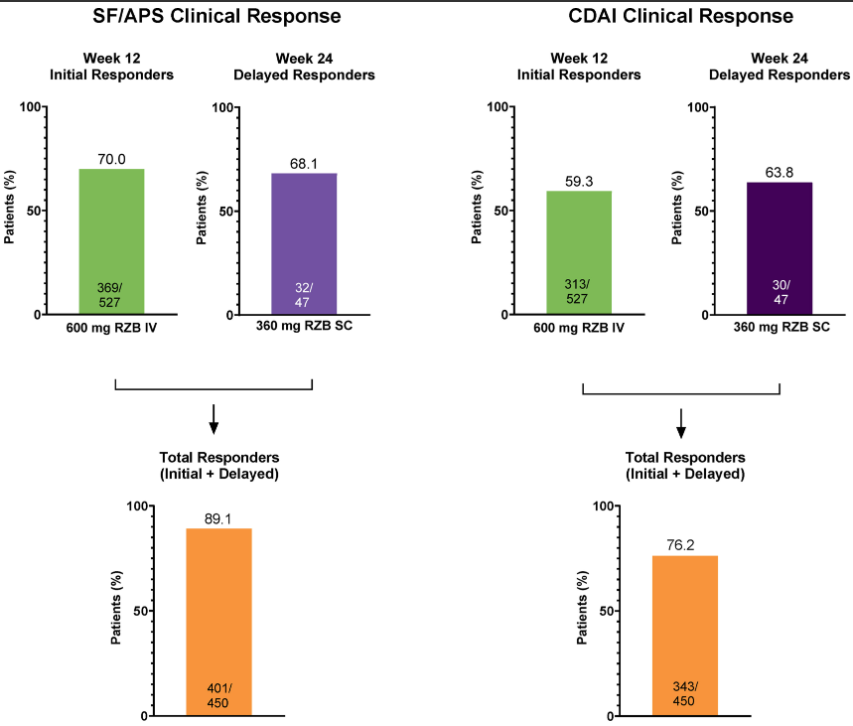
Methods: Per the study design, patients who did not achieve SF/APS clinical response following induction could receive 12 weeks of extended treatment with RZB, either via administration of the higher (1200 mg) IV RZB dose evaluated in ADVANCE and MOTIVATE or by initiation of SC RZB at doses (180 mg and 360 mg) used in FORTIFY maintenance therapy.
Key findings:
Over 60% of initial nonresponders achieved clinical response with extended RZB treatment. These patients also demonstrated improved clinical and endoscopic outcomes during the extended treatment period, which were sustained or continued to improve during maintenance.
My take: While there is a very good response with initial risankizumab therapy in Crohn’s disease, it looks like judgment on response needs to wait until 24 weeks as there are many who do not respond at 12 weeks who will subsequently respond to treatment.
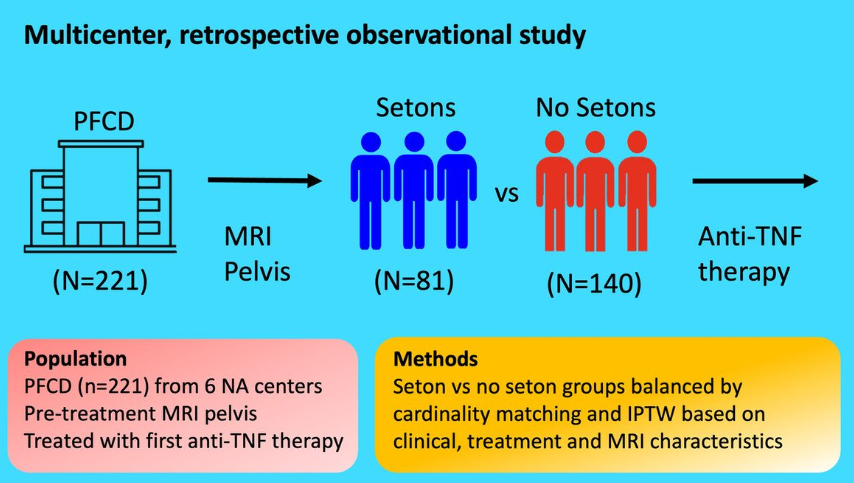
This study included 221 patients — 81 with setons and 140 without setons. Patients were treated with their first anti-TNF therapy for perianal fistulizing Crohn’s disease (PFCD) after undergoing a pelvic MRI between 2005 and 2022 from 6 North American centers. Our primary outcome was major adverse fistula outcome (MAFO), a composite of repeat local surgical intervention, hospitalization, or fecal diversion for PFCD.
Key findings:
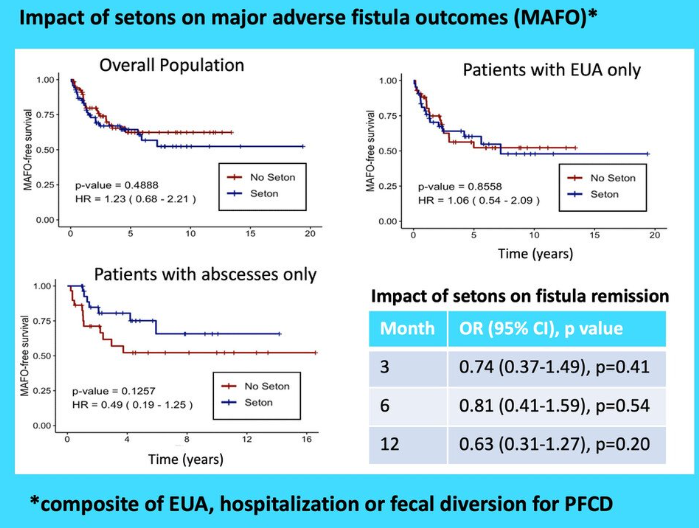
Patients with setons had similar rates of MAFO (HR 1.23; 95% CI, 0.68–2.21) and fistula remission at 6 months (OR, 0.81; 95% CI, 0.41–1.59) and 12 months (OR, 0.63; 95% CI, 0.31–1.27) compared to patients without setons
In patients with abscesses, there were lower rates of MAFO (HR, 0.49; 95% CI, 0.19–1.25) but not statistically significant in patients with setons
My take: This study indicates that seton placement may not be needed in patients who are starting anti-TNF therapy with fistulizing disease, especially if there is not an abscess present.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Of >105,000 participants with 30-year follow-up, only 9.3% achieved healthy aging (age 70, w/o any chronic diseases). Their diet was significantly associated with this outcome
A Mediterranean type diet high in fruits, vegetables, legumes, nuts, whole grains, low fat dairy products, plant-based foods, and a diet with reduced sodium, trans fats, animal-based foods, sugary beverages, ultra- processed foods was the optimal pattern
These are the specific foods that were linked with healthy aging and other outcomes. Green-favorable; Red-unfavorable
Eric Topol has provided an excellent commentary on this article for those interested in a deeper analysis: Our Diet and Healthy Aging
Dr. Topol notes that there has been a decline in interest in plant-based foods. “In The Atlantic magazine this week [among other big Signal things ;-)] there was an article (←gift link) on the loss of appeal of plant-based eating…” He also previews his new book Super Agers.
Background: The Council of Pediatric Subspecialties (CoPS) created a list of 3 to 5 learning objectives that each subspecialty believes are the most important practical skills for the general pediatrician and recommends be included in general pediatrics, medicine-pediatrics, and other combined residency program curricula… The Subspecialty Perspectives on (pediatrics) Training (SPoT) action team within CoPS asked each subspecialty representative, most of whom were fellowship program directors at the time, in collaboration with their subspecialty colleagues, to provide a list of 3 to 5 practical learning objectives that should be expected of graduating pediatric residents and practicing general pediatricians in the evaluation and management of conditions related to their subspecialty.
Recommendations for Pediatric Gastroenterology:
My take: This article identifies four of the most important areas in pediatric gastroenterology. If I were to add a fifth, given the wide variety of problems in our field, it would be to know how to quickly reach out to a pediatric gastroenterologist when you need advice.
This article is worth a quick look to see if you have the essential knowledge in all pediatric subspecialty fields (Table 1). One of the most important that relates to pediatric gastroenterology is in the allergy section: “Identify the importance of avoiding indiscriminate testing for food allergy without an appropriate clinical history concerning for IgE mediated food allergy.”
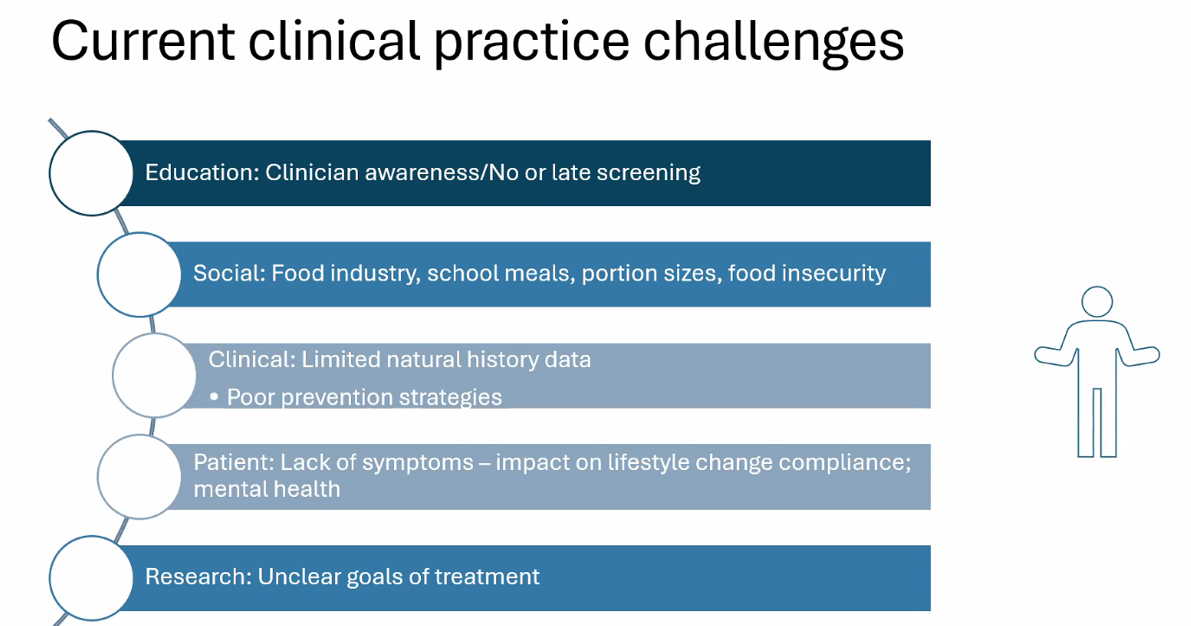
Dr. Marialena Mouzaki recently gave an excellent ground rounds at Children’s Healthcare of Atlanta. My notes below may contain errors in transcription and in omission. Along with my notes, I have included many of her slides (with permission).
Key points:
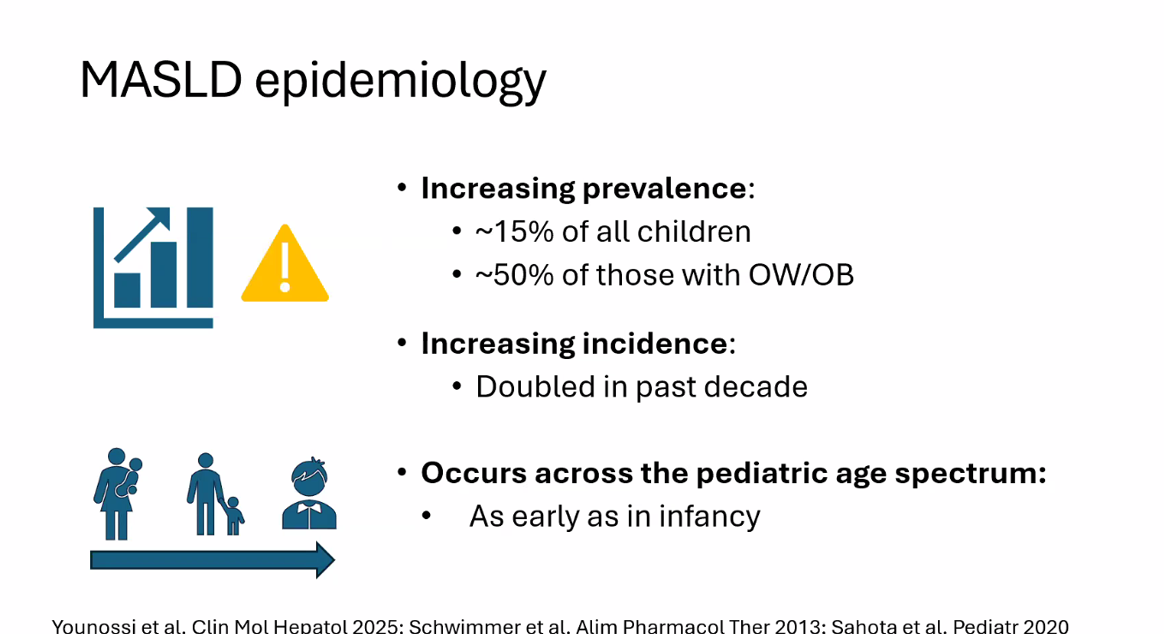
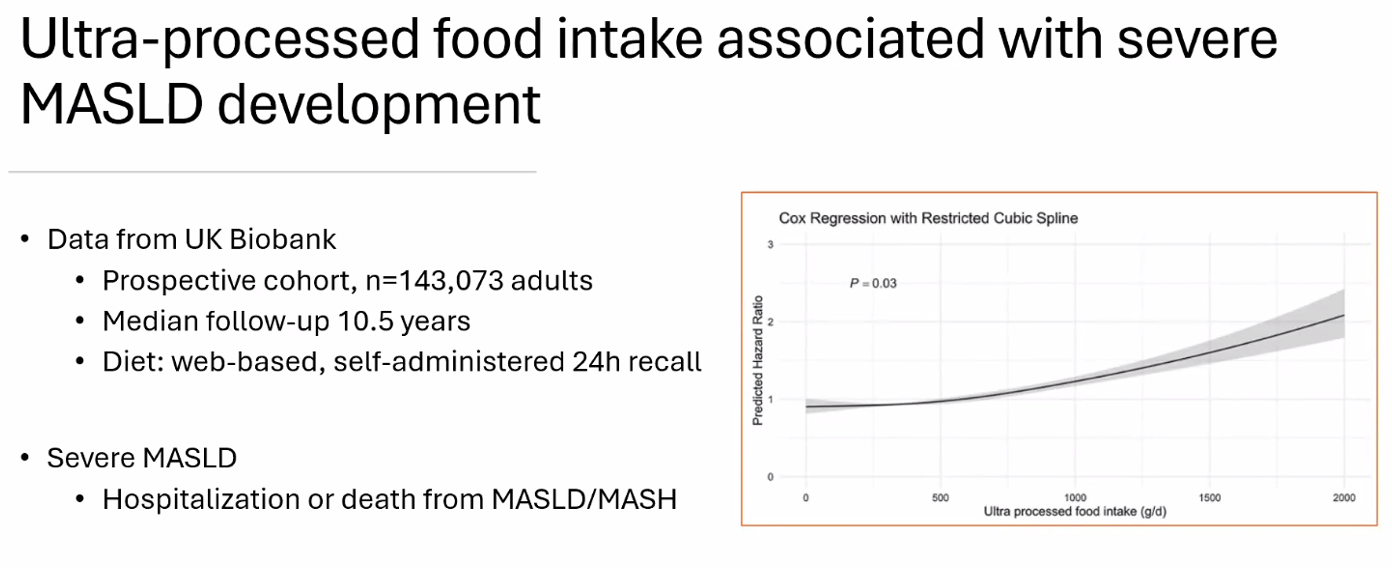
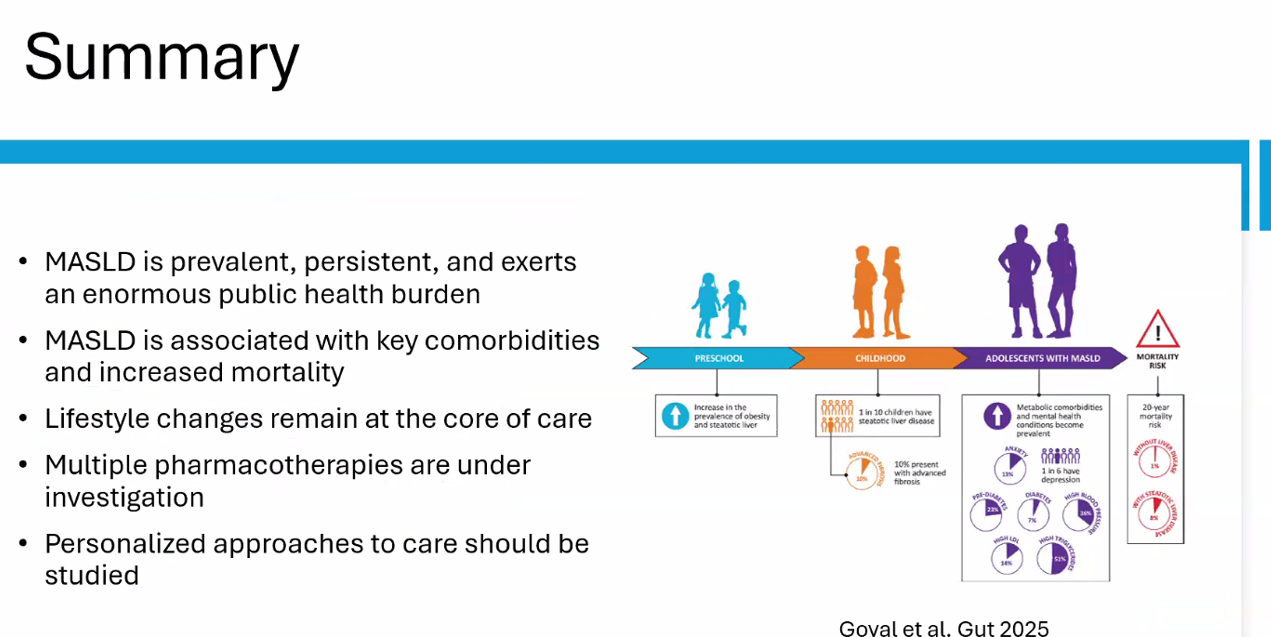
Epidemiology: Metabolic associated steatotic liver disease (MASLD) is very common and increasing in prevalence
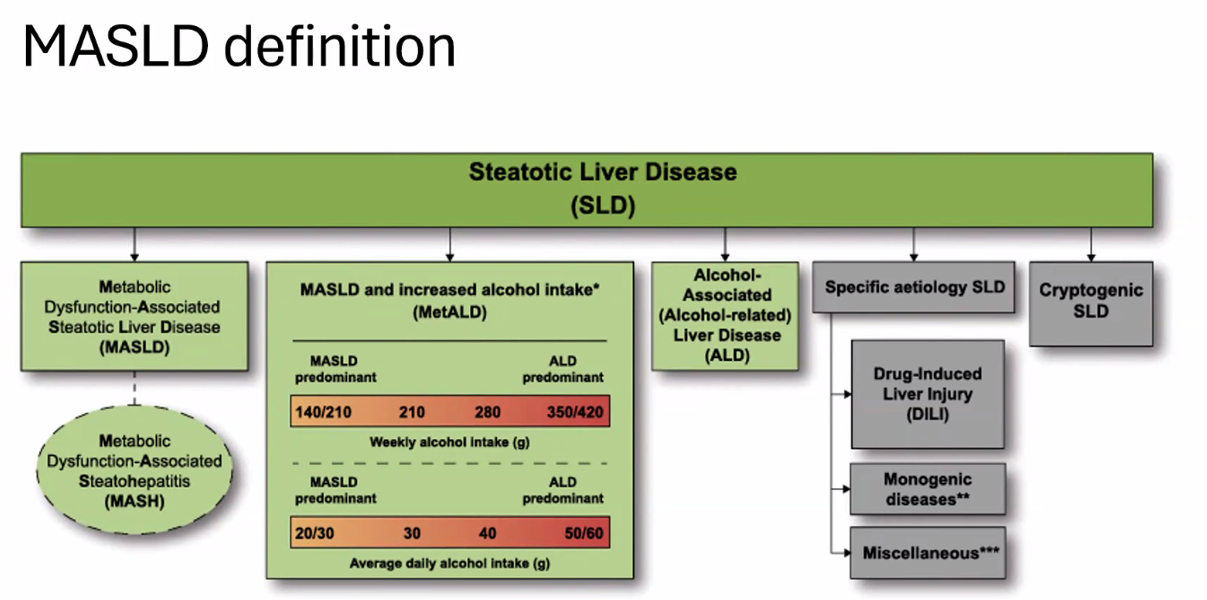
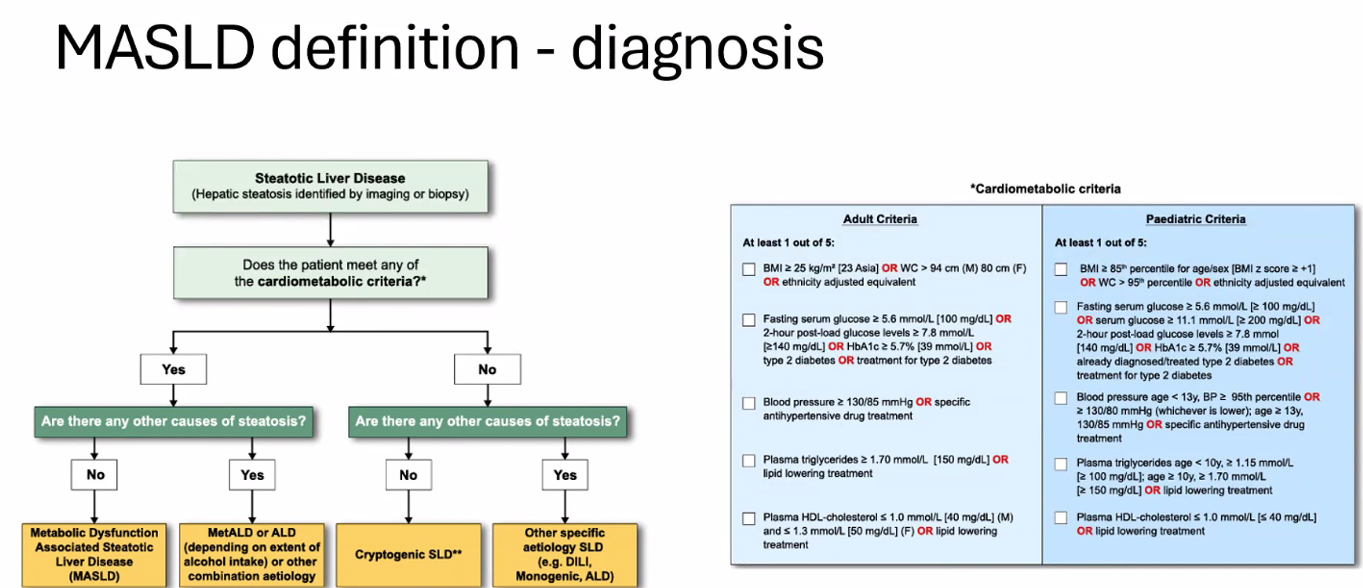
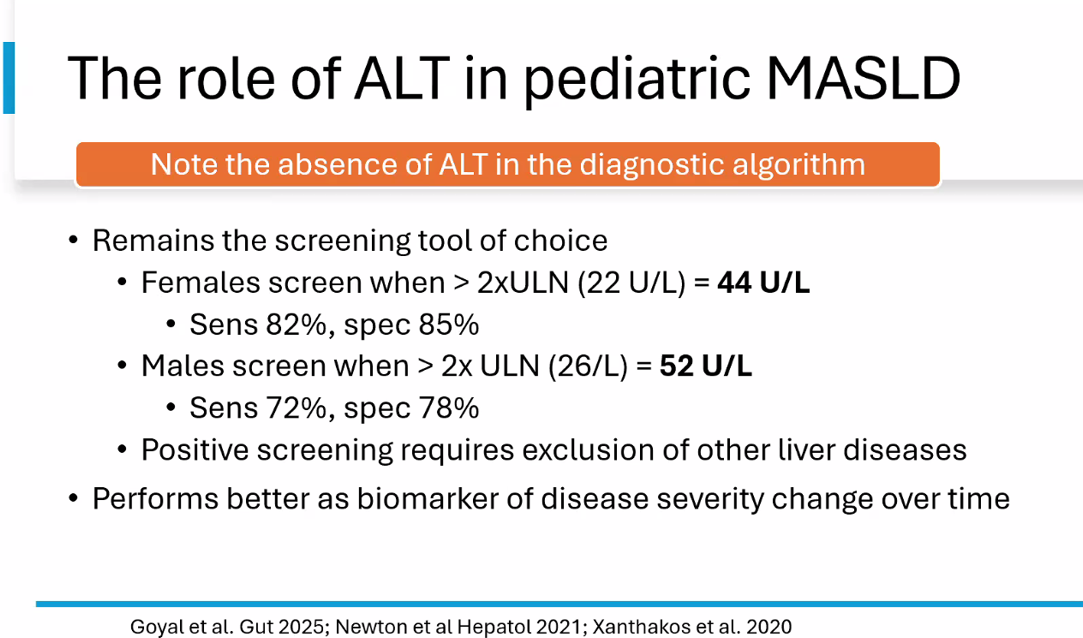
There is new terminology and new diagnostic thresholds
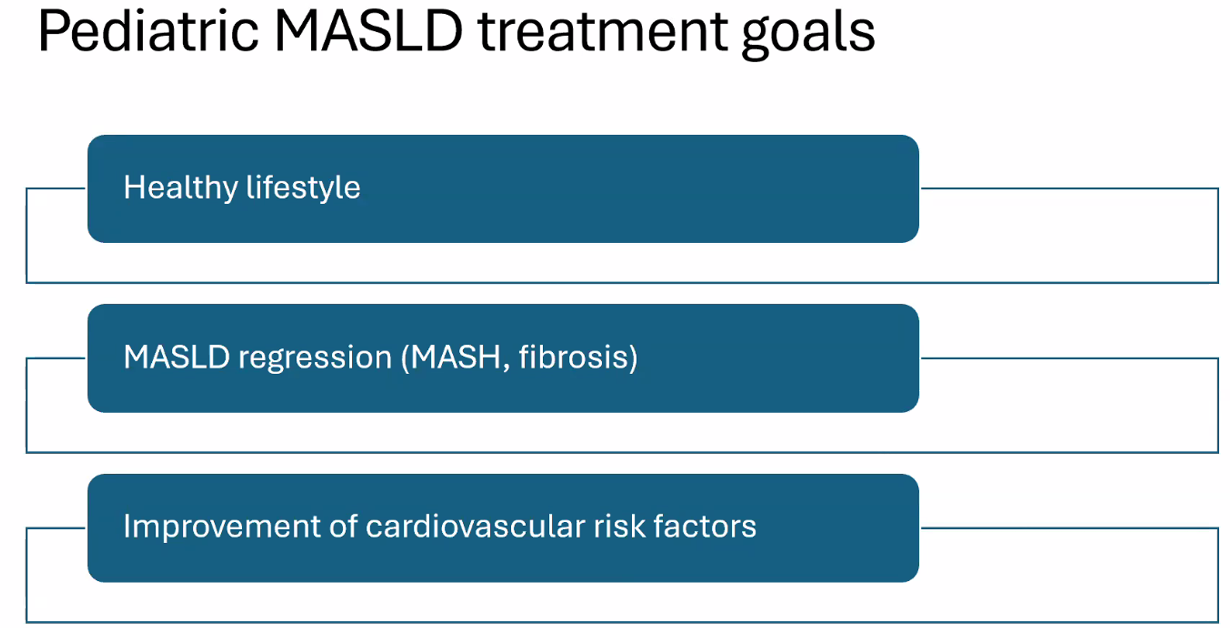
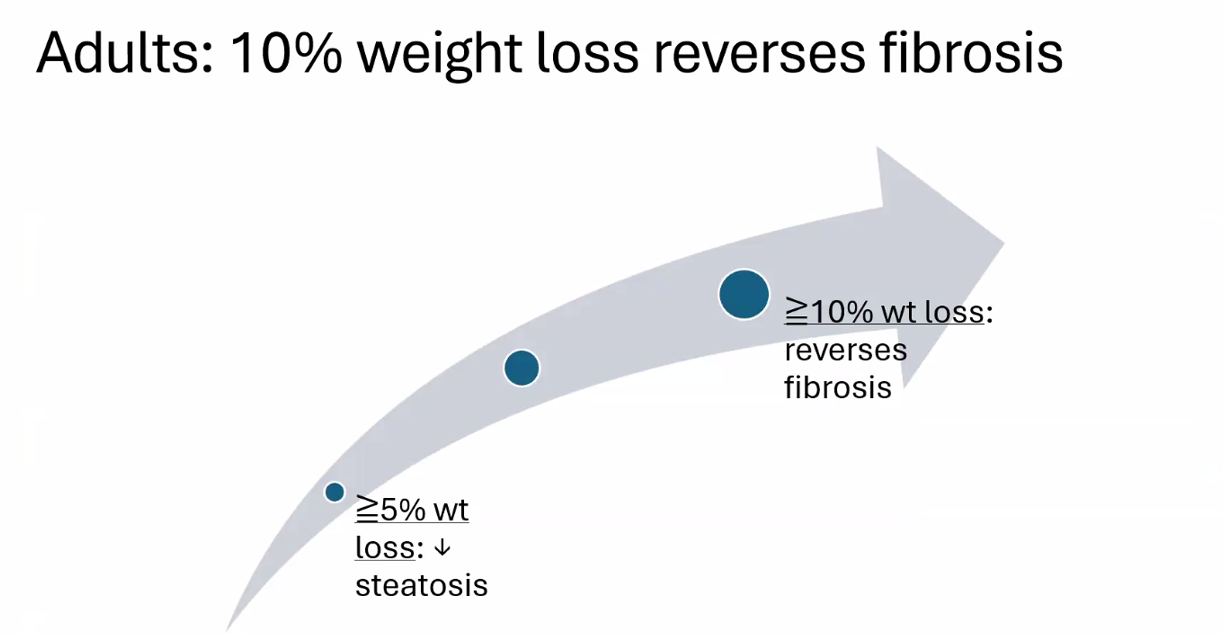
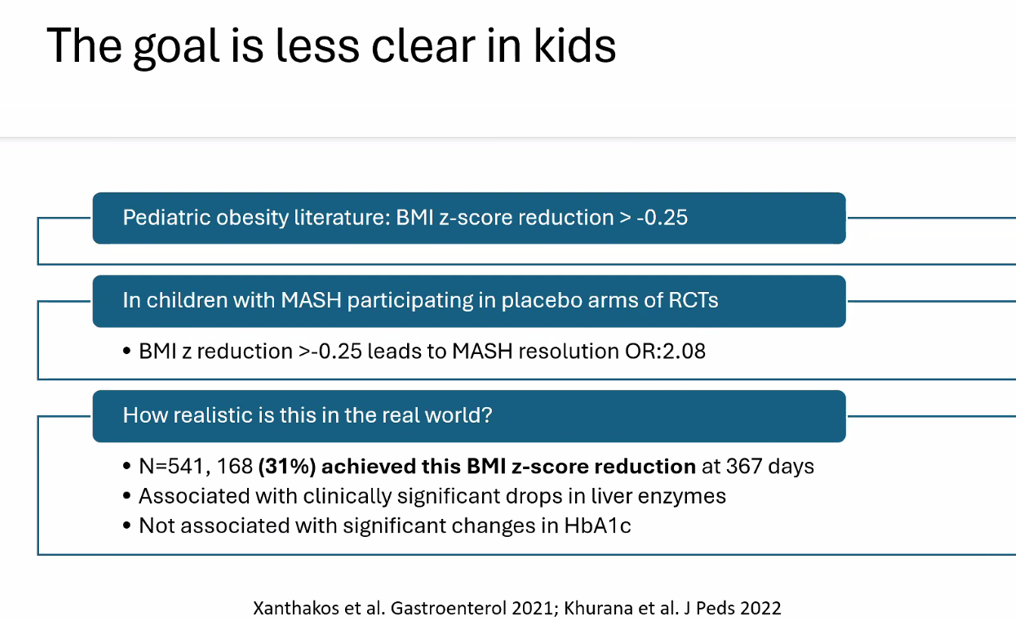
Treatment cornerstone relies on lifestyle changes including diet modifications and exercise. Small weight reductions (10 lbs in adults)/improvement in BMI (z reduction of >0.25) can be beneficial
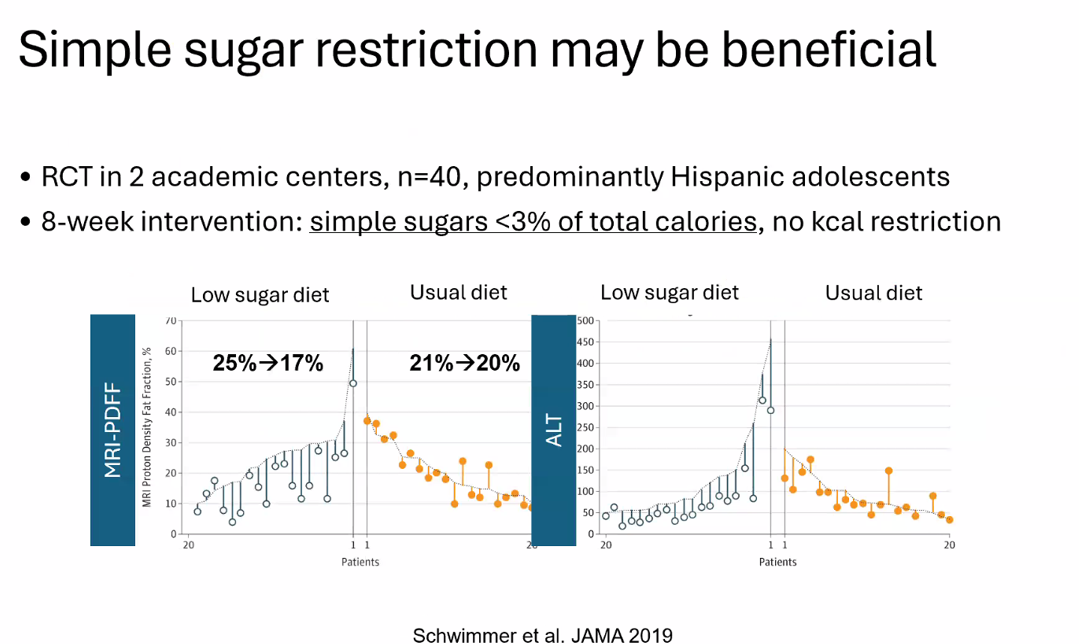
Diet: No specific diet has proven more effective than others (eg. low carb, Mediterranean). Avoiding simple sugars is helpful
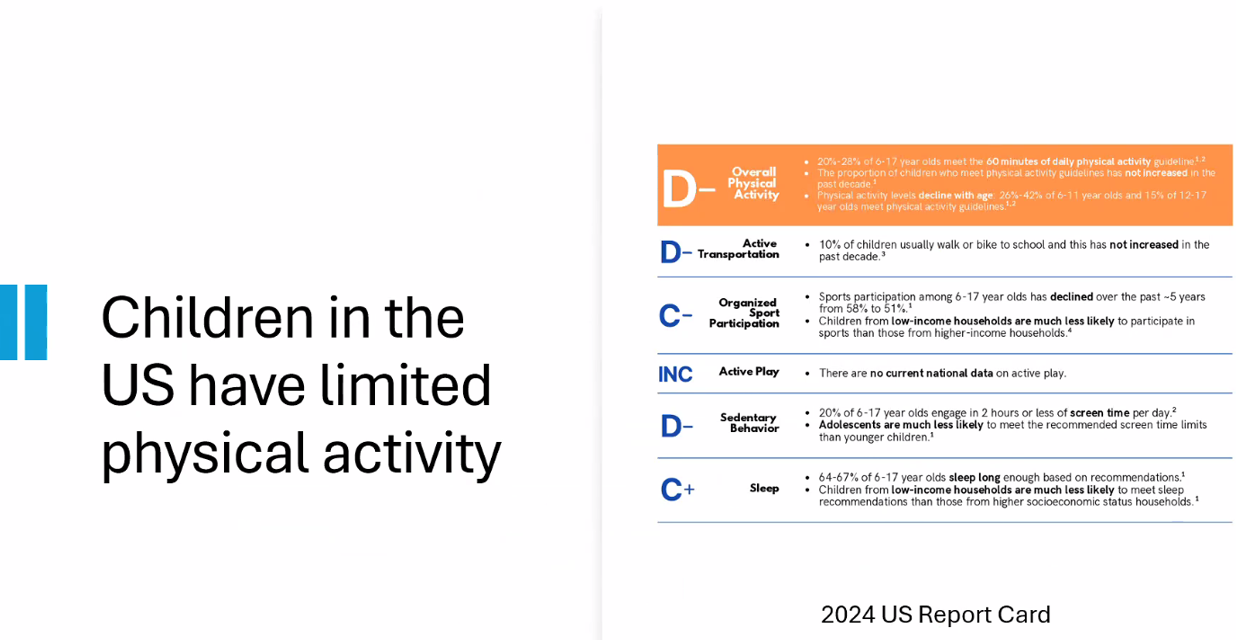
Exercise: US children do not get enough physical activity (goal 1 hour daily). Exercise has not been studied well for pediatric MASLD but it has been proven to reduce cardiovascular disease and premature death
Medications: Medications are not part of routine care for pediatric MASLD in 2025 When they are available, use without lifestyle changes could be detrimental (eg. sarcopenia, worse cardiometabolic profile, nutritional deficiencies)
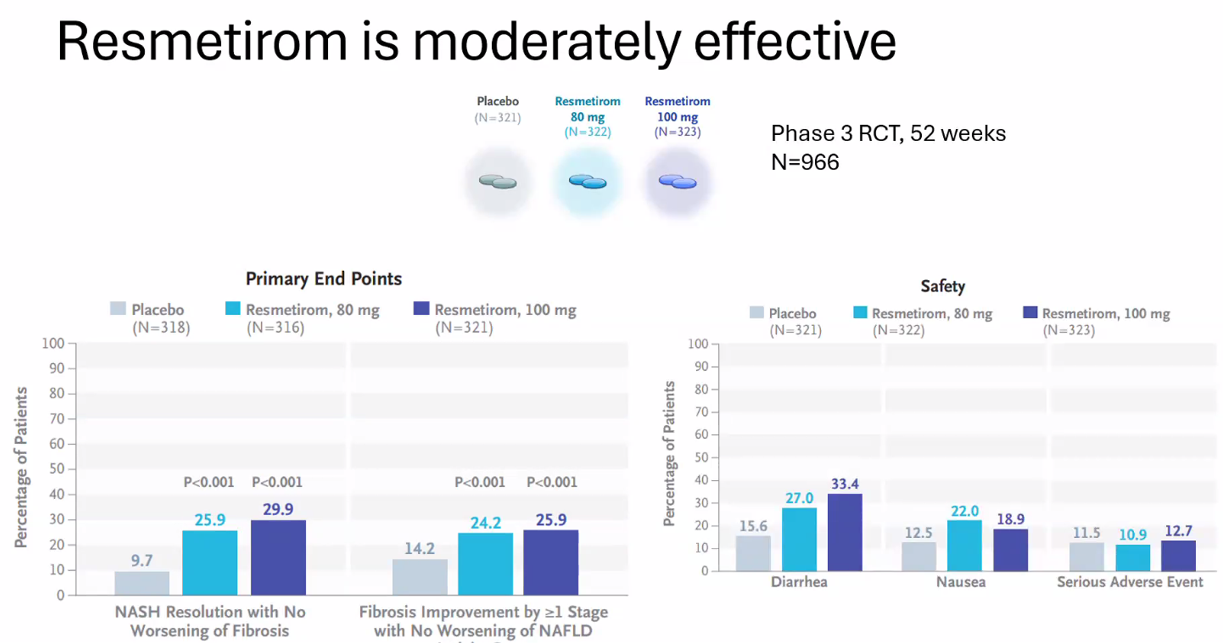
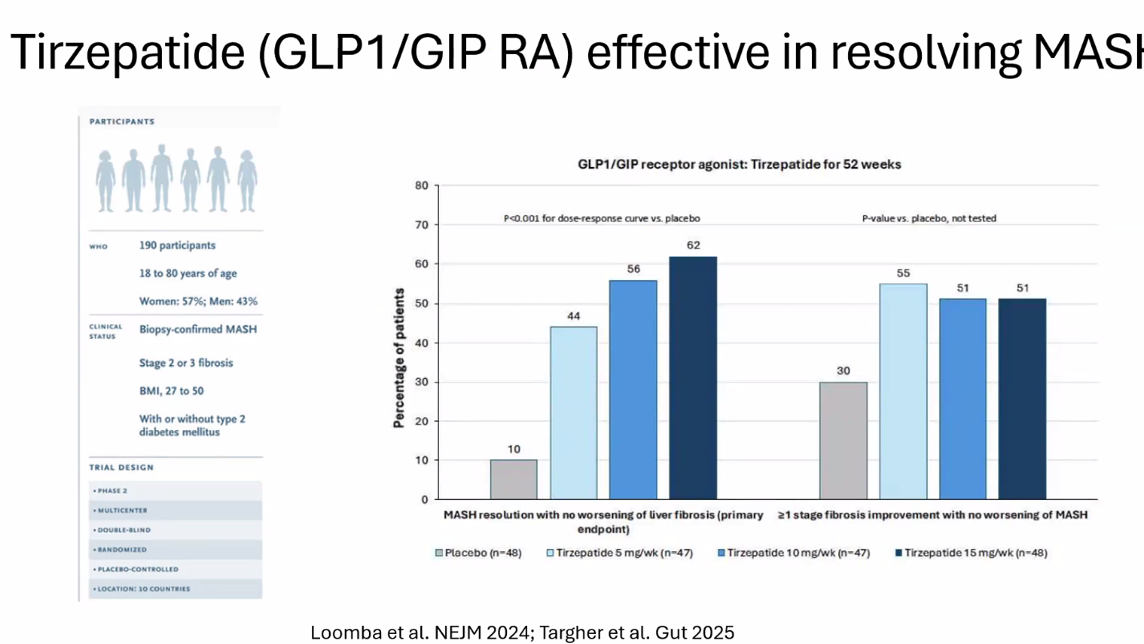
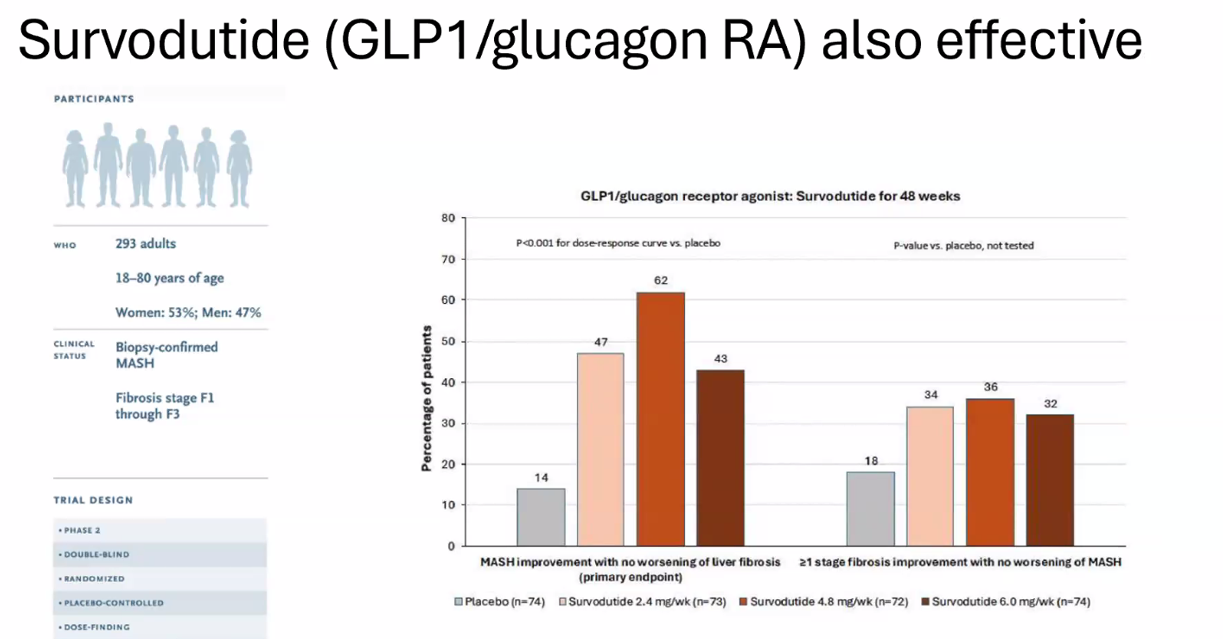
Multiple GLP-1 RA-containing agents appear promising (Semaglutide, tirzepatide, survodutide). Resmetirom is FDA approved for the treatment of MASLD with stage 2-3 fibrosis in adults.
Treat comorbidities like diabetes, obstructive sleep apnea (OSA), dyslipidemia and hypertension. Treatment of OSA may help MASLD
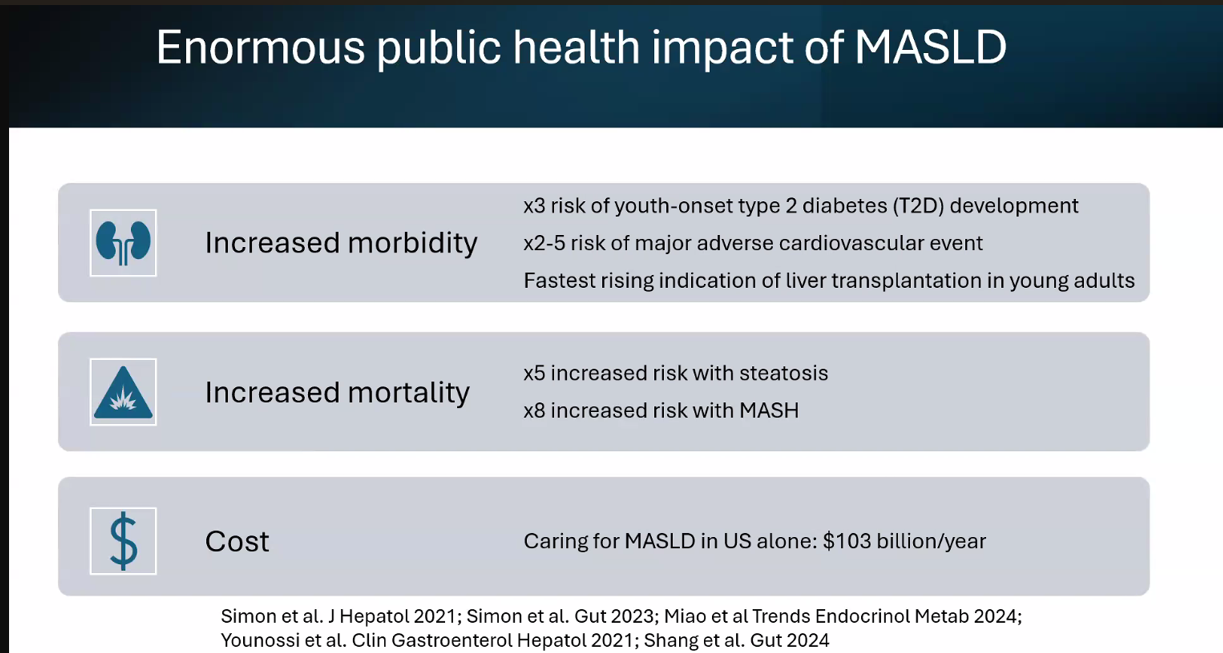
The leading cause of mortality in adults with MASLD is due to cardiovascular disease