From NBC News: EpiPen Prices Rocket Along With Drugmaker Executive’s Pay

Also, this story has been discussed in NY Times (Epipen & Health Care System Dysfucntion) and USA Today (see below)

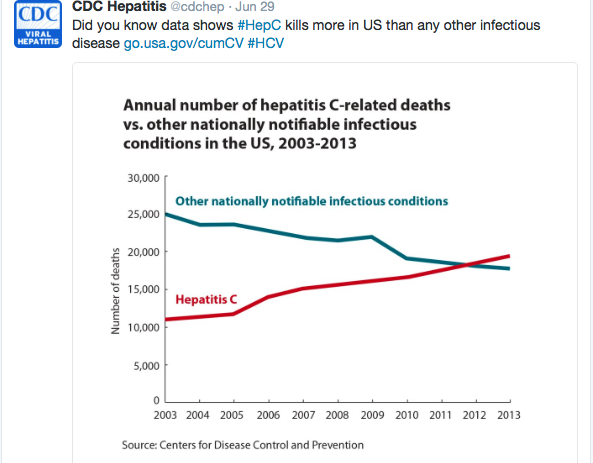
Also, from KT Park’s twitter feed:


From NBC News: EpiPen Prices Rocket Along With Drugmaker Executive’s Pay
Also, this story has been discussed in NY Times (Epipen & Health Care System Dysfucntion) and USA Today (see below)
Also, from KT Park’s twitter feed:
While Primary Biliary Cholangitis (PBC) (previously called primary biliary cirrhosis) is seen mainly in adult hepatology practices, a new treatment may be emerging and this same medication is likely to be considered for several liver conditions.
Reference: F Nevens et al. NEJM 2016; 375: 631-43.
This 12 month, double-blind, placebo-controlled phase 3 “POISE” trial with 217 patients examined the use of obeticholic acid with or without ursodeoxycholic acid. Surrogate markers of PBC were followed & the treatment groups improved compared to placebo. However, adverse effects, particularly itching, were more common in the obeticholic acid groups; serious adverse effects were 11-16% in the treatment groups compared with 4% in the placebo group.
Results below:

My take: It will be nice when important clinical endpoints can be assessed for this therapy like progression to cirrhosis. For now, the cost of this treatment is ~$70,000 yearly.
Related blog post:
“The petaloid cataract is classically seen in patients who have had blunt trauma to the eye.” NEJM: Petaloid Cataract

L Laine, A Nagar. Am J Gastroenterol 2016; 111: 913-15.
This reference explains how these clinicians discuss the long-term use of proton-pump inhibitors with their adult patients. Thanks to Ben Gold for this reference. Here are a couple pointers:
WHAT WE TELL PATIENTS: “Because of inherent risk of bias and low effect sizes we cannot conclude that associations of PPIs and adverse outcomes such as dementia and CKD in recent observational studies are vailid…Nevertheless, we cannot conclude that risks do not exist…we need to ensure that benefits outweigh potential risk. If PPIs are indicated, using the lowest effective dose and, if possible, intermittent rather than daily therapy..should decrease the risk of potential side effects.”
On the same topic, Paul Moayyedi (in Gastroenterology and Endoscopy News, August 2016): “Every study has shown that sicker patients tend to be prescribed PPIs…Sick patients tend to develop other illnesses so PPIs will be associated with about any disease you can imagine in a database.” As such, he asserts that weak associations (OR <2) are usually due to cofounding factors. “The only benefit [these studies]..have is that it is another opportunity to discuss with the patients about stopping their PPI therapy, as there are a significant proportion…on these drugs unnecessarily.”

The August issue of Hepatology had several articles on Hepatitis C confirming the efficacy of newer agents:
Also in Hepatology:
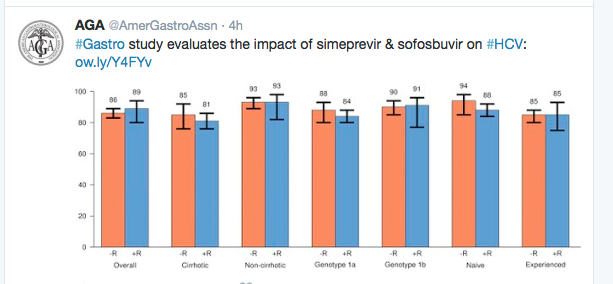
From earlier study of “real-world” treatment of Genotype 1. Gastroenterol 2016; 150: 419-29. (Full text link)
From NPR: Children Missing Out on Hepatitis C Treatment
An excerpt:
A study by the Philadelphia Department of Health points to what Wen and others in the medical profession see as a worrisome trend: Children with hepatitis C may be unaware of their diagnosis and the potential need for treatments down the road in order to prevent long-term liver damage.
Using city surveillance data, the study found that as many as 8 in 10 children at high risk for hepatitis C exposure in Philadelphia were never screened for the condition. More specifically, of the approximately 500 moms-to-be who were registered as having hepatitis C between 2011 and 2013, only 84 of their newborns, or about 16 percent, were tested for the virus by 20 months of age.
My take: As the article discusses, with the advent of better treatments, which will be available for children (?next 1-2 years), identifying Hepatitis C acquired prenatally is becoming important.
Related blog posts:
A recent study of 23 children (8-14 yrs) correlated functional MRI results with watching commercials.
Full text: The Influence of Televised Food Commercials on Children’s Food Choices
Key finding: The ventromedial prefrontal cortex, a reward valuation brain region, showed increased activity during food choices after watching food commercials compared with after watching nonfood commercials.
Author’s conclusion: Overall, our results suggest watching food commercials before making food choices may bias children’s decisions based solely on taste, and that food marketing may systematically alter the psychological and neurobiologic mechanisms of children’s food decisions.
My take: When is the last time you saw a commercial for broccoli? While food companies may not fully understand how their marketing affects kids’ brains, I’m certain they understand how it affects their bottom line.

Lake McDonald, Glacier Natl Park
The widespread use of anti-TNF therapy for inflammatory bowel disease has improved clinical outcomes including fewer surgeries, hospitalizations, and complications. One consequence of this usage has been the exposure of infants to biologics due to their usage by their mothers during pregnancy. A recent study (M Julsgaard et al. Gastroenterol 2016; 151: 110-19) explores this topic further.
In this study, the authors prospectively followed 80 pregnant women: 36 received adalimumab & 44 infliximab. In addition, 39 received concomitant thiopurine therapy.
Key findings:
The authors recommend avoidance of live virus vaccines in biologically-exposed infants for up to 1 year unless drug clearance has been documented. Currently, this would affect only rotavirus vaccination.
My take (borrowed from editorial pgs 25-26): “For now, the sum of evidence seems to support continued use of anti-TNF therapy in pregnancy when clinically indicated and, despite measureable levels in offspring, there does not seem to be a significant clinical consequence.”
Related study: “Adverse Pregnancy Outcomes among women with inflammatory bowel disease: a population-basd study from England” Inflamm Bowel Dis 2016; 22: 1621-30. The authors identified 1969 pregnancies from a total of 364,363 singleton pregnancies. Women with Crohn’s had increased preterm births with an Odd ratio of 1.42, babies with low birth weight (OR 1.39); women with ulcerative colitis had only a small increase risk in preterm birth (absolute risk <2.7%).
Related blog posts:

Art at Big Creek Greenway, Alpharetta
A recent review (ME Cogswell et al. NEJM 2016; 375: 580-5) helps sort out some of the confusion regarding sodium intake and cardiovascular disease. In brief, the authors point out the excessive sodium intake is clearly linked to heart disease, stroke and death. The importance has been questioned by some due to a few studies suggesting that low sodium intake could also increase the risk of cardiovascular disease.
The authors note that these studies have shown only weak associations & were likely a matter of reverse causation due to the low sodium group having increased numbers of participants with numerous health issues (eg diabetes, hypertension, chronic illness and cardiovascular disease).
By looking at these results based on “Hill’s Criteria” to assess whether an association is causal, the authors show that the association of low sodium intake and cardiovascular disease indicates that this association is NOT causal.
Hill’s criteria:
The authors note that population exposure to sodium correlates better than individual exposure, perhaps due to measurement issues. Key points:
My take: If we are to take advantage of the science to reduce cardiovascular deaths, we need to convince manufacturers and restaurants to reduce sodium.
Related blog posts:

Highline Trail, Glacier Nat’l park
IN 1862, Maurice Raynaud described a 26-year-old female patient: “Under the influence of a very moderate cold…she sees her fingers become ex-sanguine, completely insensible, and of a whitish-yellow color. This phenomenon …lasts a variable time, and terminates by a period of very painful reaction, during which the circulation is re-established…and recurs to the normal state.”
An updated review on Raynaud’s: FM Wigley, NA Flavahan. NEJM 2016; 375: 556-65.
This review highlights treatments and the differential diagnosis of primary Raynaud’s phenomenon form secondary causes (eg scleroderma, SLE, dermatomyositis, Sjogren’s and others).

A) Pallor phase B) Cyanotic phase C) Normal nailfold capillaries (primary phenomenon) D) Abnormal nailfold capillaries typical of microvascular disease
