C Liu et al. J Pediatr Gastroenterol Nutr. 2024;79:1124–1133. Open Access! Impact of acid blocker therapy on growth, gut microbiome, and lung disease in young children with cystic fibrosis
Background: Historically, acid suppression has been given as adjuvant therapy to optimize PERT and thereby improve growth and nutritional needs in CF
Methods: This was a prospective cohort of 145 infants followed in 6 CF centers. This was a retrospective study examining the effects of acid blocker therapy and outcomes at 3 years of life in children with cystic fibrosis.
Key findings:
- Acid blocker therapy (ABT) use before age 3 years was frequent, with 81 (56%) of patients on H2 receptor antagonist (H2RA) or proton pump inhibitor (PPI), and higher among pancreatic insufficient (60%) versus pancreatic sufficient (26%) children.
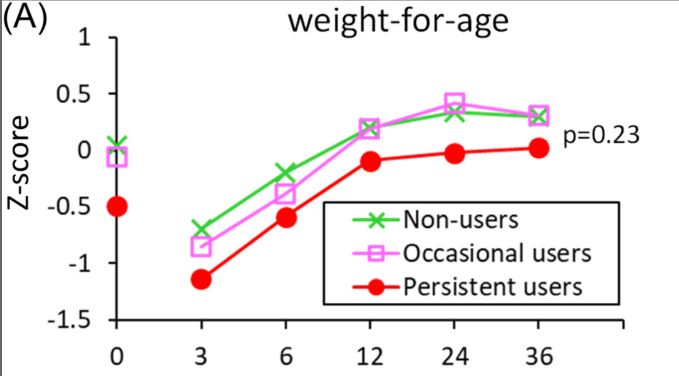
- Growth improvements were not significantly greater.
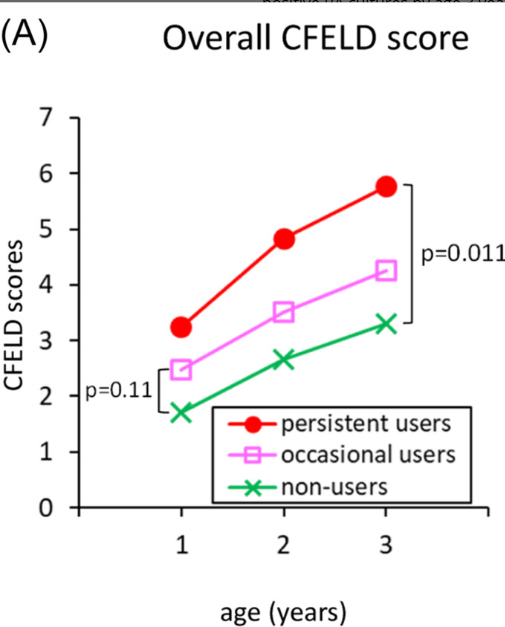
- Early-onset lung disease was more severe, in persistent ABT users compared to nonusers of ABT.
- ABT was associated with reduced gut microbiome diversity
Discussion:
- “Results from our FIRST cohort of infants and toddlers with CF showed that prolonged ABT was not associated with significant improvements in growth but instead significant negative alterations to the GM and progression of early-onset lung disease. Evidence from our study is in line with the growing body of literature advocating for more judicious PPI therapy as it has been associated with adverse outcomes such as pulmonary infections, fractures, and anemia.22–24“
- One limitation, which was NOT discussed in the article, was selection bias. Since there was not randomization of PPI use, it could be that PPI prescription was more common in children with more severe disease.
My take (borrowed in part from authors): Despite the potential for selection bias, it is clear that “acid blockers are not benign.” Given the potential for worse outcomes, PPI prescription should be restricted to those with a clear indication.
Related blog posts:
- Thanks: Updated Long-Term PPI Use Smartphrase
- Why Observational Studies Are Misleading & PPI Association with Kidney Stones
- Austin Bradford Hill, PPIs and IBD
- Long-term Effects on Bone Health of PPIs in Infancy?
- Study: PPIs Did Not Cause Dementia in Older Adults
- PPIs: Good News on Safety (Part 2)
- PPIs: Good News on Safety
- AGA Blog: What are the complications of PPI Therapy?