NBC News 3/20/24: New health warning issued about the dangers of water bead toys
“The absorbent polymer beads are often marketed as colorful, slimy, sensory items for kids to play with. They can be as small as a stud earring — little enough to swallow — but grow to the size of a marble or even a golf ball when immersed in water. Once inside a child’s body, they can cause gastrointestinal blockages. The CPSC (Consumer Product Safety Commission) recorded nearly 7,000 water bead-related ingestion injuries in emergency rooms between 2018 and 2022.”

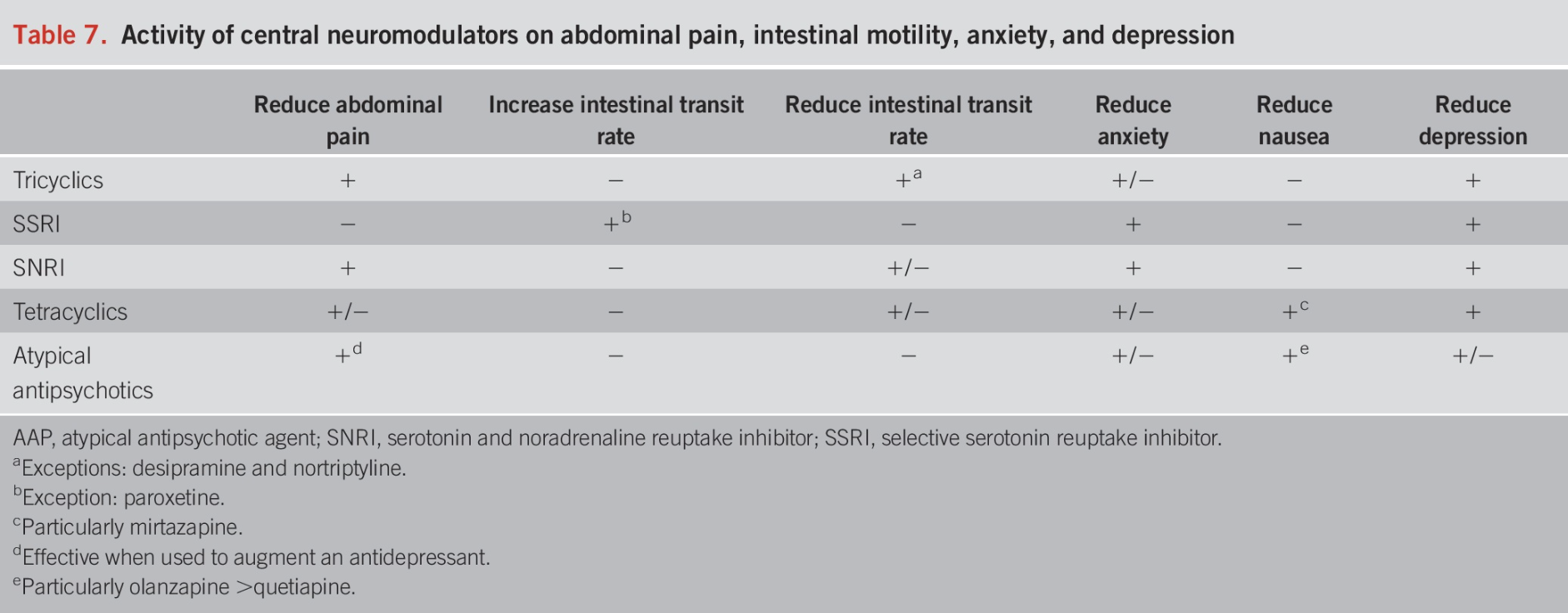
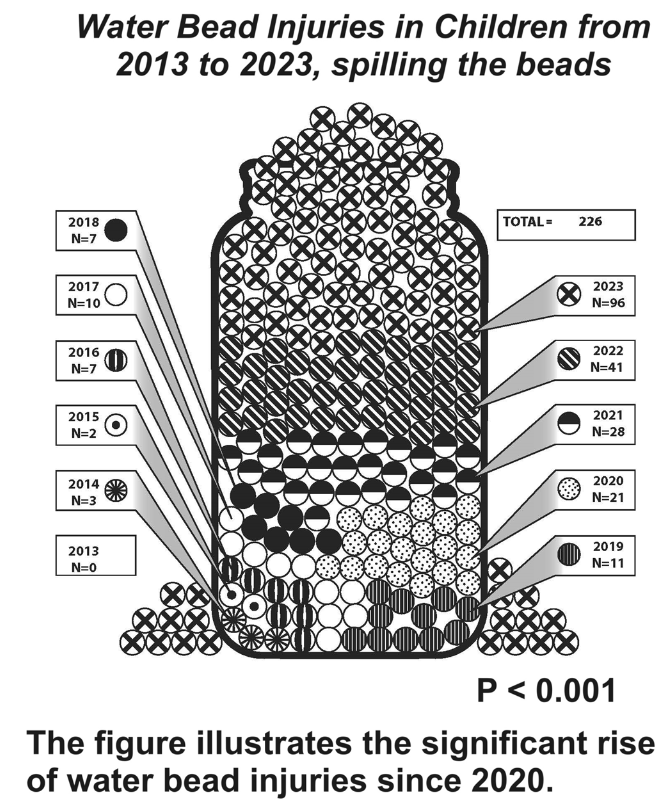
EA Pasman, MA Khan, NT Kolasinski, PT Reeves. JPGN 2024;79:752–757. Water bead injuries by children presenting to emergency departments 2013−2023: An expanding issue
CPSC issued a recall of more than 50,000 Chuckle & Roar Water Beads Activity Kits in 2023 after a 10-month-old child reportedly swallowed one of the water beads and died. (Ref: AAP News (American Academy of Pediatrics). Water bead toy kits recalled following death of 10-month-old child. Accessed Sept 21, 2024)
Methods: The authors used the National Electronic Injury Surveillance System (NEISS) to identify water bead injuries from 2013 to 2023. The nationally representative NEISS database catalogs ED encounters for injuries related to consumer products over a nationwide census and captures 500,000 injury-related encounters annually. The authors used more stringent criteria than CPSC; thus the numbers of injuries from water beads in their study are less than those reported by CPSC.
Key findings:
- Children under age 2 years comprised 29% of injuries.
- There was a significant uptrend in water bead injury frequency after 2020.
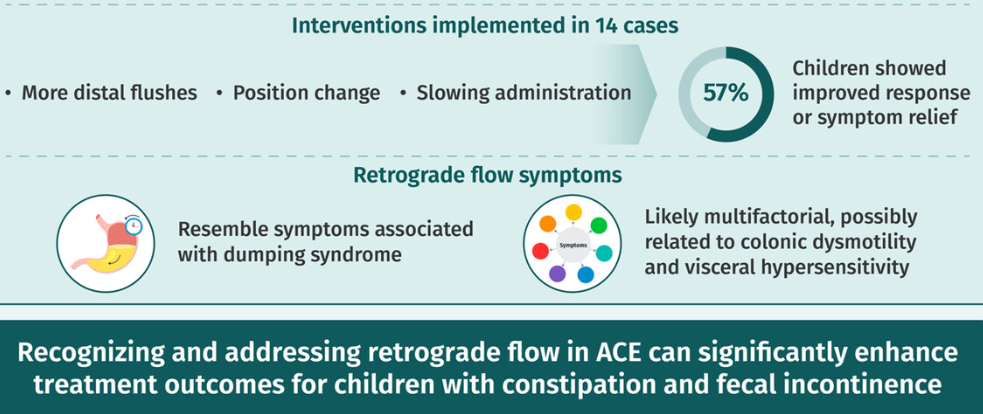
Discussion: Published NASPGHAN recommendations include “‘urgent’ endoscopy (<24 h from presentation, following usual NPO guidelines) for any absorptive object ingested and found to be in the stomach or small bowel. The report recommends emergent upper endoscopy for any absorptive object impacted in the esophagus causing sialorrhea.”
My take: The database captures only a fraction of these ingestions. These objects, even if they do not cause acute injury, could pose long-term harms due to potential carcinogenicity.
Related blog post: Foreign Bodies in Children -Expert Guidance