A Simard et al. J Pediatr Gastroenterol Nutr. 2024;79:800–806. Role of ileal diversion in pediatric inflammatory bowel disease
Indications:
Severe, medically refractory colitis
Complex and medically refractory perianal disease
In combination with bowel resection for irreversible bowel damage (e.g., fistulae, abscesses, or strictures)
Diversion “provides the opportunity to reduce steroid use, improve growth and observe the natural history of the disease in a more controlled manner. It may also enhance quality of life”
My take: This is a handy article when considering ileal diversion in a patient with medically-refractory inflammatory bowel disease.
MR Smetak, LJ Wilcox. N Engl J Med 2024;391:1139. Button-Battery Ingestion
An excerpt:
A previously healthy 11-month-old girl presented to the emergency department with a 2-week history of progressively worsening dysphagia and cough..A chest radiograph showed a foreign body with a “halo” or “double-ring” sign. Approximately 10 hours after endoscopic removal, “torrential hematemesis and hemorrhagic shock developed. During emergency surgical exploration, no source of bleeding was initially identified, but intraoperative angiography revealed a fistula between the esophagus, which was dilated, and the left common carotid artery (Panel B, arrow). The artery was ligated, and hemostasis was achieved.” The patient was discharged 32 days after admission without neurologic or functional deficits.
My take: Even in children in the hospital, massive bleeding due to a coronary artery to esophagus fistula carries an extremely high mortality rate.
Foreign Bodies in Children -Expert Guidance Even with “spent” batteries, there is enough residual charge to cause injury and all ingestions (even if asymptomatic) into the esophagus require emergent removal. If these batteries are in the stomach & asymptomatic, urgent removal is recommended if age < 5 years and BB ≥20 mm.
Mitigation Efforts for Button Batteries (also includes case report of aorto-esophageal fistula and emergency surgery 25 days after ingestion of a button battery)
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
All patients received IV PPI treatment prior to endoscopy. Key finding from this multicenter randomized open-label adult trial:
The 30-day rebleeding rates in vonoprazan and PPI groups were 7.1% (7 of 98) and 10.4% (10 of 96), respectively
There were similar outcomes with regard to safety and secondary outcomes
My take: This study shows that oral vonoprazan is not inferior to IV PPI treatment for high-risk peptic bleeding ulcers. Perhaps, a study with more participants would show superiority of vonoprazan given the absolute lower rebleeding rates in this study.
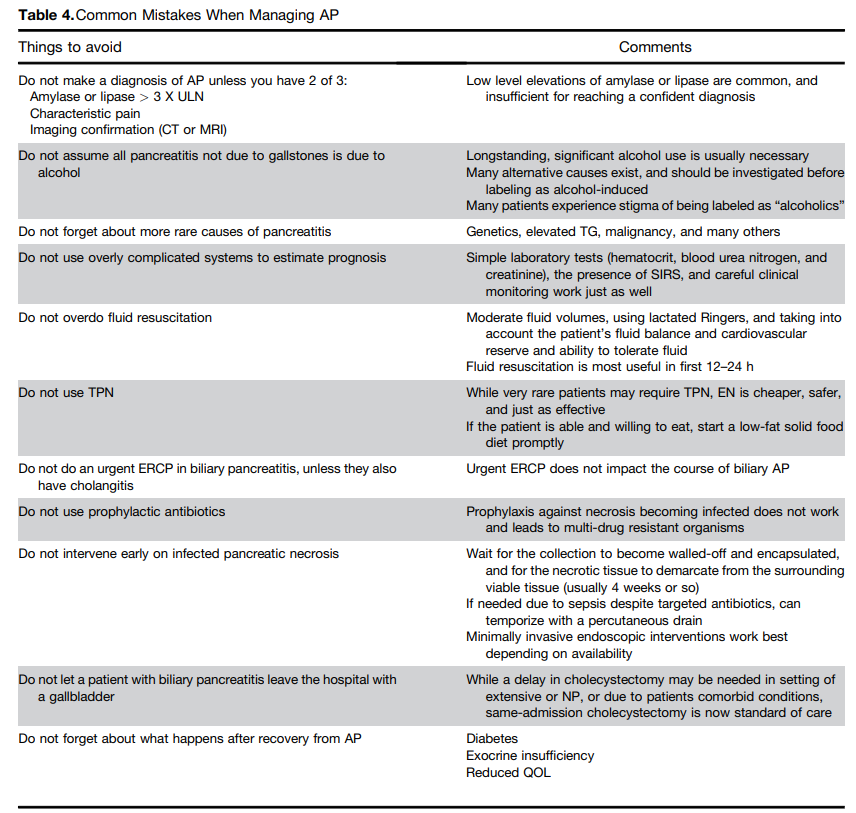
While this review focuses on acute pancreatitis in adults, there are areas of overlap with pediatric patients who have acute pancreatitis. Many of the points in this article were reviewed in the lecture by Dr. Freeman (summarized earlier this week).
A couple of details regarding these recommendations:
Nutrition: “Current guidelines recommend initiating early (as soon as tolerated) oral feeding with solid (low-fat) diet in patients with predicted mild AP and this approach reduces length of hospitalization. Patients with severe AP or NP may be intolerant to oral diet…studies noted that the pancreas is largely insensitive to meal stimulation during AP. Early enteral nutrition (EN) was shown to have a beneficial trophic effect in preserving gut mucosal integrity and reducing gut bacterial translocation. EN was compared with TPN in AP in several RCTs and the results were statistically aggregated in several meta-analyses to establish the superiority of EN in mortality, multiorgan failure, and rate of infection.”
TPN: “Given the cost burden, risk of catheter-related sepsis, electrolyte and metabolic derangement, and gut barrier failure, currently use of TPN is reserved for patients for whom EN is not possible or is not able to meet the minimum calorie requirements. It should be noted that although all guidelines advise avoiding TPN, it continues to be used.”
Antibiotics: “Current guidelines do not recommend prophylactic antibiotics in predicted severe AP or sterile necrosis because this practice is associated with the development of multidrug-resistant bacteria and fungal superinfection. It can be difficult in severe pancreatitis to know if clinical deterioration is due to ongoing pancreatitis with SIRS, or due to a new infection. Procalcitonin is useful in distinguishing SIRS from bacterial sepsis. The PROCAP randomized trial used procalcitonin testing at 0, 4, and 7 days and weekly thereafter with a threshold of 1.0 ng/mL to guide initiation, continuation, and discontinuation of antibiotics. The procalcitonin based algorithm decreased the probability of being prescribed an antibiotic and the number of days on antibiotics without increasing infection or harm in patients with AP.”
Progression to Chronic Pancreatitis: “A systematic review and meta-analysis of progression showed that 10% of patients with first episode of AP and 36% of patients with recurrent AP develop CP, with risk being highest among smokers, alcoholic patients, and men.”
Risk of Diabetes: “A prior systematic review and meta-analysis of patients with an index attack of AP found that newly diagnosed diabetes occurred in 15% of individuals within 12 months, and risk increased 2-fold for diabetes after 5 years. The development of diabetes was not significantly associated with the severity of pancreatitis, etiology of disease, patient age, or gender.”
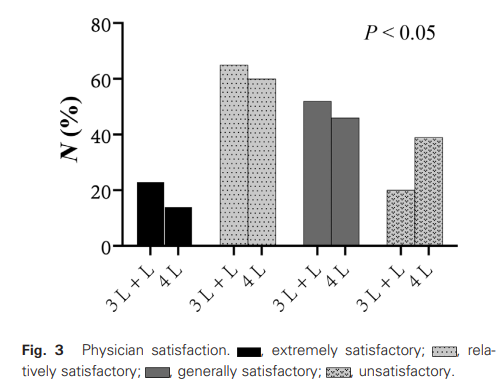
Methods: In this prospective, single-center, randomized controlled trial, 322 participants (18-75 yrs) were divided into two groups: a 3-L PEG + 870-μg linaclotide group (administered as a single dose for 3 days) and a 4-L PEG group. All enrolled patients had constipation as defined by the Rome IV criteria (fewer than three bowel movements per week with associated symptoms such as straining and hard or lumpy stools).
Linaclotide dosing: One 290-μg linaclotide capsule 30 min before the first meal for 3 days leading up to the colonoscopy, but not on the day of the procedure itself
Key findings:
The 3-L PEG + linaclotide group showed significantly higher rates of adequate and excellent bowel preparation than the 4-L PEG group (89.4% vs 73.6% and 37.5% vs 25.3%, respectively; P < 0.05).
Boston Bowel Preparation Scale (BBPS) score in the linaclotide group was significantly higher than that in the 4-L PEG group.
Adverse effects like nausea and vomiting were less common in the linaclotide group compared to the 4-L PEG group. Nausea was noted in 10% of linaclotide group compared to 24.5% in the 4-L PEG group. vomiting occurred in 5% and 19.5% respectively. Overall, adverse effects were 24.4% compared to 41.5% respectively.
The cecal intubation rate was 87.5% in the linaclotide group and 81.8% in the 4-L PEG group, which indicated a higher trend in the linaclotide group. Both groups had a lower cecal intubation rate than the 90% benchmark rate and could be related to the underlying constipation.
My take: In patients with constipation, linaclotide with 3L PEG resulted in a better cleanout than a standard 4L PEG prep. Combination laxatives as part of the prep should be considered in those with underlying constipation.
This study would be hard to replicate in children as very few children with constipation need a colonoscopy. It is possible that the addition of linaclotide would improve cleanouts even in children without constipation. Other studies showing linaclotide can help with cleanouts in the general population include the following:
Zhang M, et al. Eur. J. Gastroenterol. Hepatol. 2021; 33: e625–33.
We had a great pancreas update lecture from Dr. Jay Freeman. In my view, a great lecture involves a well-delivered informative lecture that likely leads to an improvement in clinical practice. My notes below may contain errors in transcription and in omission. Along with my notes, I have included many of his slides.
Currently there are NO recommendations for medications that can prevent progression of chronic pancreatitis
Use of neuromodulators (eg. TCAs, Gabapentin) are often given to reduce pain
Cognitive behavioral therapy has been used in chronic pancreatitis with significant improvement
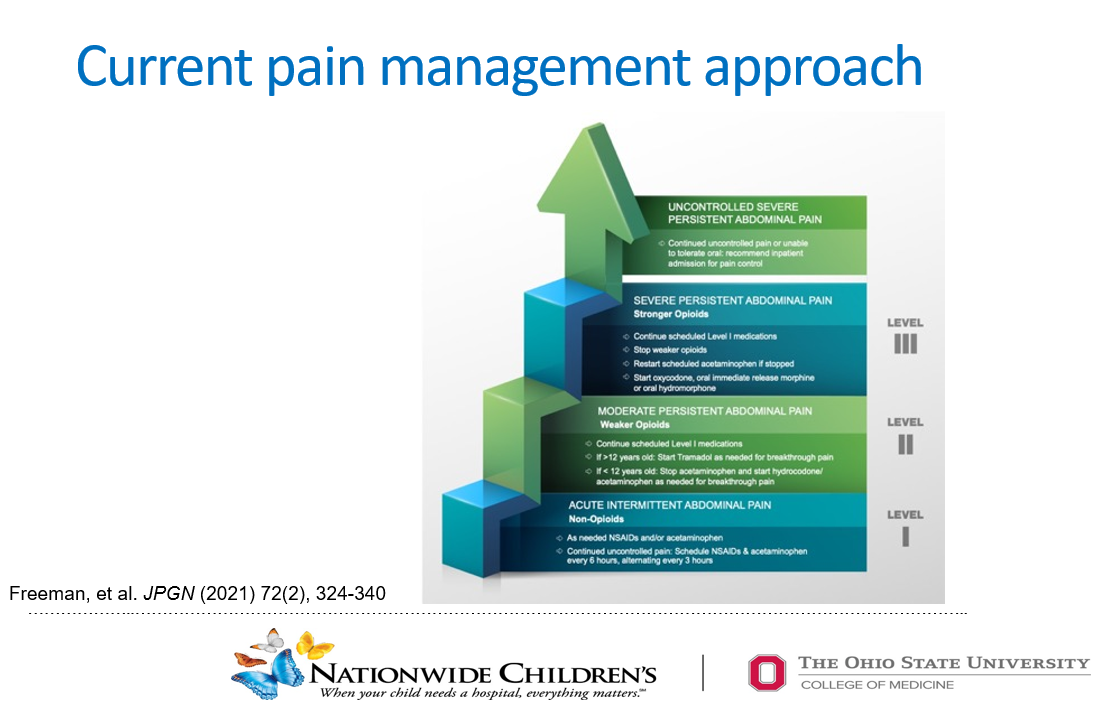
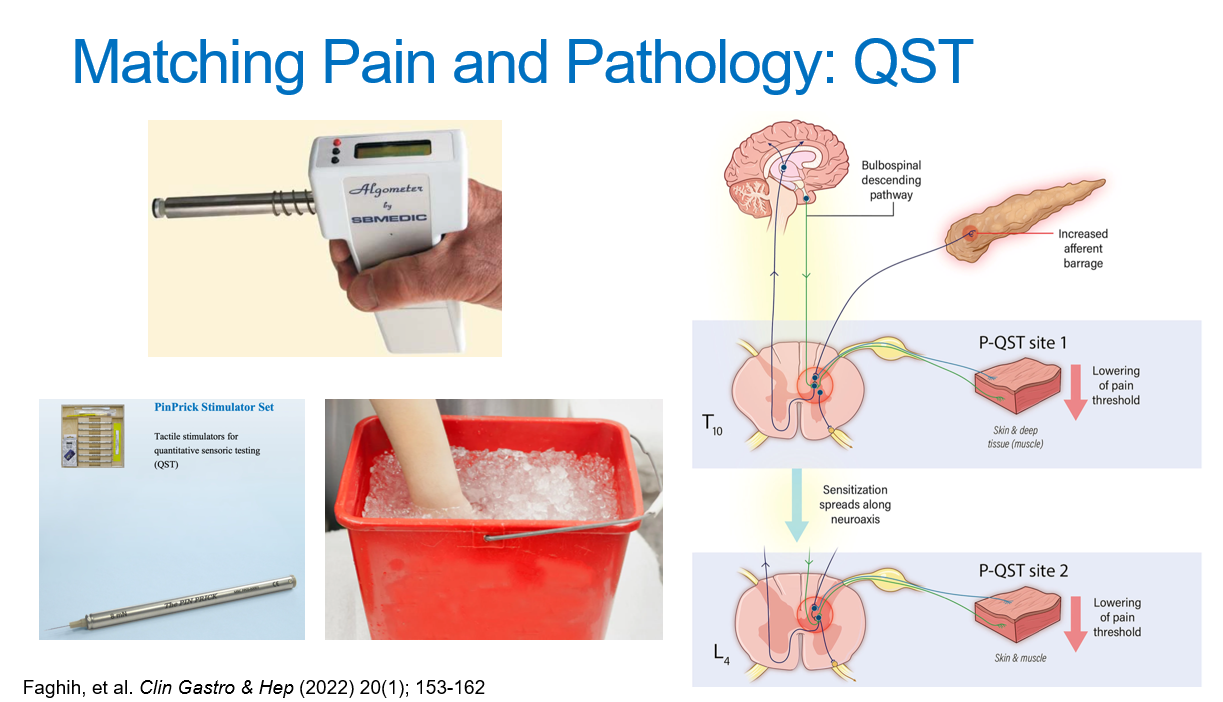
Pain management is working towards objective pain markers
Changes in pancreatic function are associated with risk of pancreatitis
CF drugs have changed pancreatic function in the CF population and may be helpful in other populations
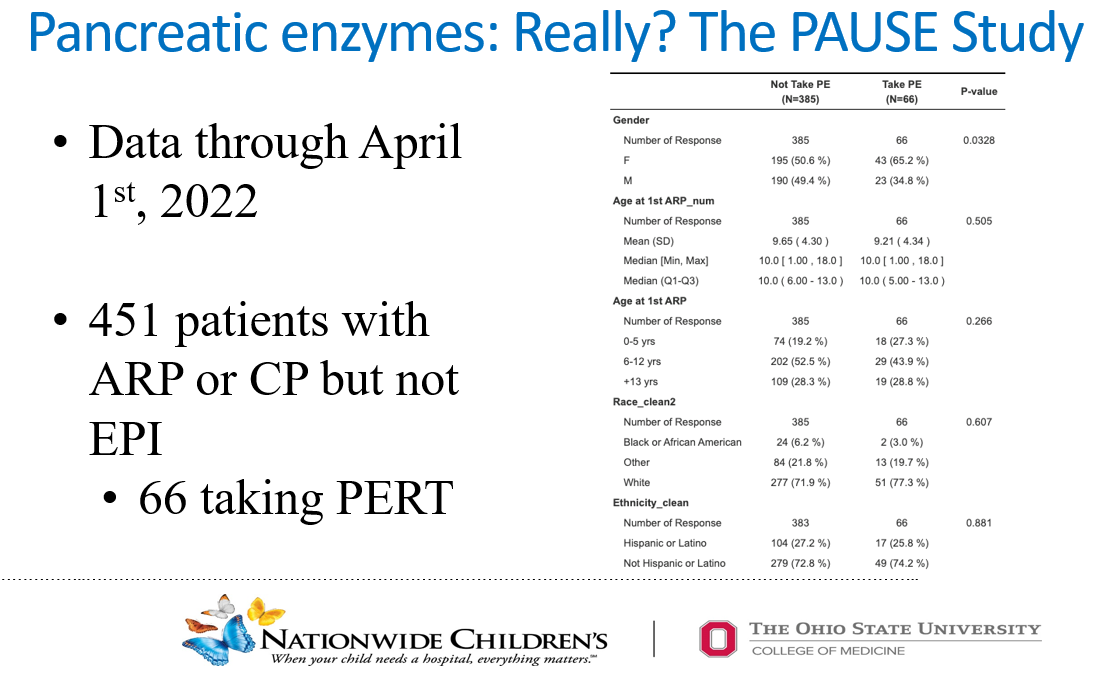
Pancreatic enzymes (PERT) may decrease the risk of pancreatitis. Based on the PAUSE study, a double-blind study is needed to determine if PERT can reduce pancreatitis with ARP or CP
From Nationwide Children’s Summary: “The researchers found that nearly 17% of children with pancreatic-sufficient ARP and CP were treated with pancreatic enzymes. Children started on pancreatic enzyme therapy experienced fewer AP episodes annually, and approximately 40% of children on pancreatic enzyme therapy had no additional AP episodes [during a mean 2.1 years of follow-up] over approximately two years of follow-up. Children with a SPINK1 mutation and those with ARP (compared with CP) were less likely to have an AP episode after initiating pancreatic enzyme therapy… a randomized, placebo-controlled clinical trial is necessary to evaluate the true impact of pancreatic enzymes for these patients.” Freeman AJ, et al. American Journal of Gastroenterology. 2024 Apr 18. DOI: 10.14309/ajg.0000000000002772. Epub ahead of print.Open Access!Pancreatic Enzyme Use Reduces Pancreatitis Frequency in Children With Acute Recurrent or Chronic Pancreatitis: A Report From INSPPIRE. “After initiation of PERT, the mean AP annual incidence rate decreased from 3.14 down to 0.71 ( P < 0.001).”
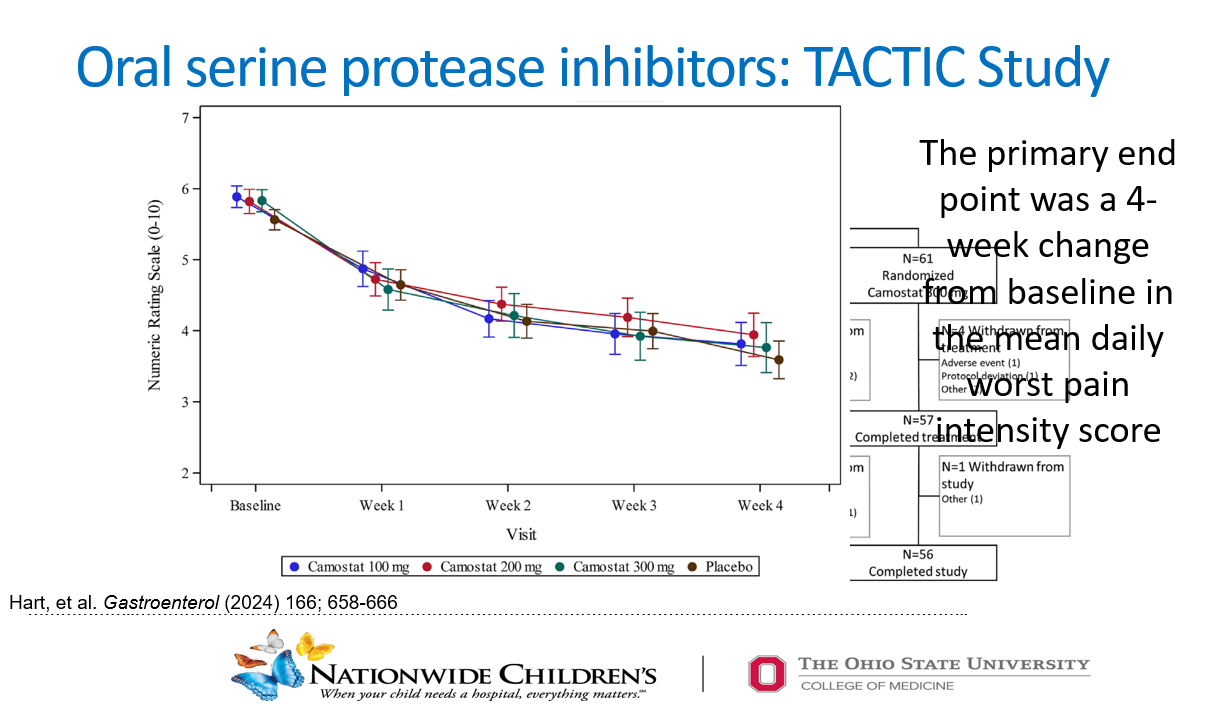
The TACTIC study showed that an oral serine protease inhibitor reduced daily pain; however, the 4-week change was similar to placebo. This study shows why placebo-controlled studies are needed
There are other treatment approaches that are being studied in adults including antifibrotics, simvastatin, and paracalcitol
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
We had a great pancreas update lecture from Dr. Jay Freeman. In my view, a great lecture involves a well-delivered informative lecture that likely leads to an improvement in clinical practice. My notes below may contain errors in transcription and in omission. Along with my notes, I have included many of his slides.
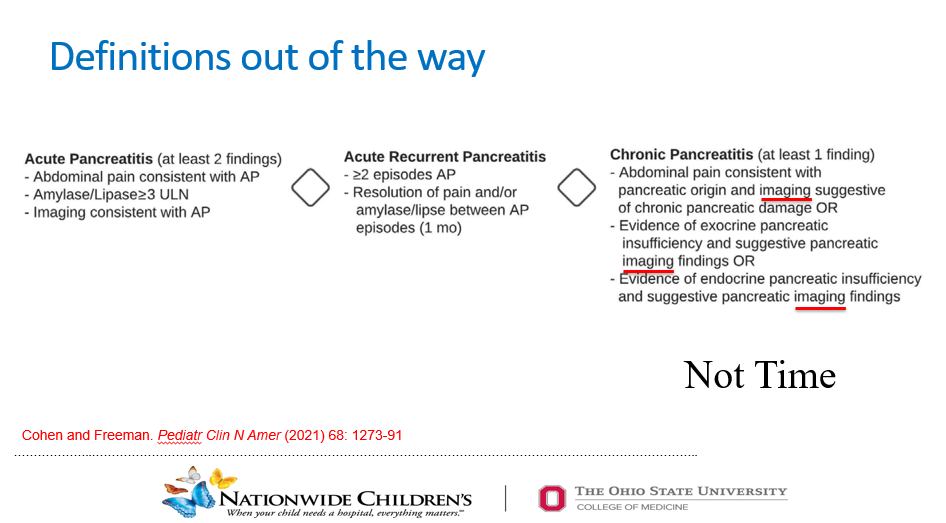
About 10% of patients with acute pancreatitis already have damage indicating chronicity
Severe pancreatitis is often defined by degree of organ dysfunction (eg. cardiac, pulmonary, renal). A practical definition of severe pancreatitis in children is whether the patient requires admission to an ICU
The term “position paper” is typically used instead of “guidelines” due to lack of definitive data and reliance on expert opinion
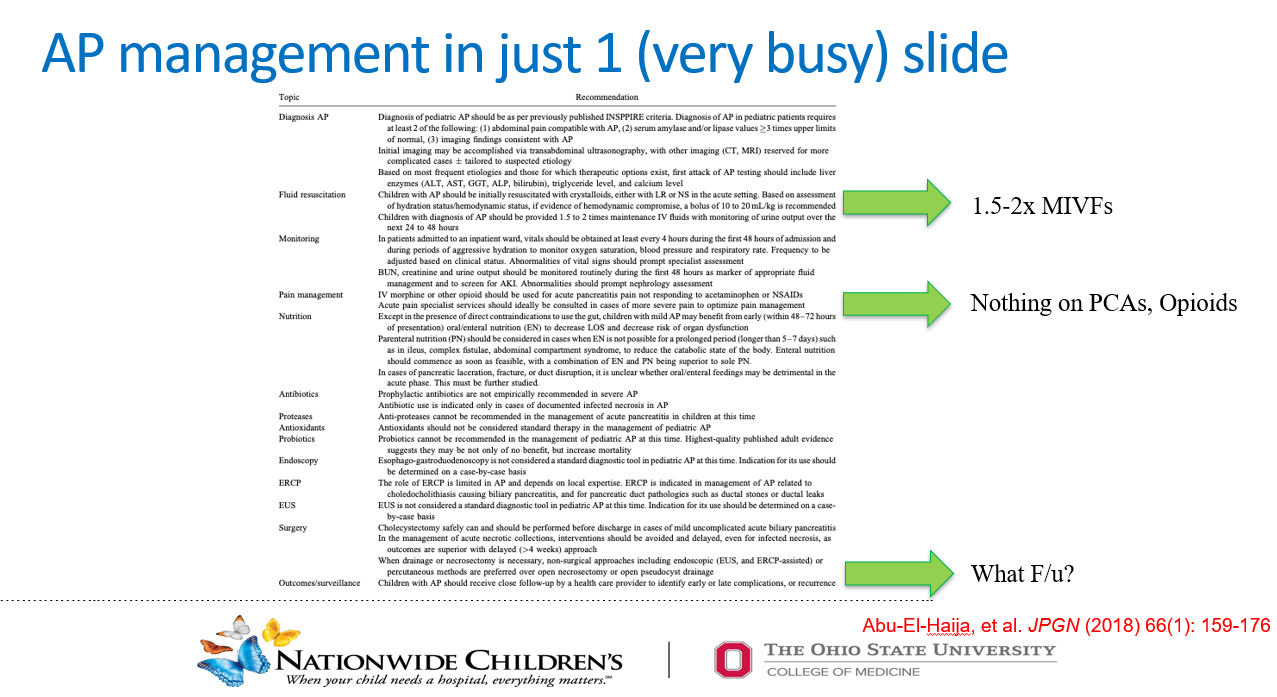
While the guidelines suggest 1.5-2.0 x maintenance fluid volumes, the benefit of this additional IVFs is not clear. Dr. Freeman’s clinical practice is often to start with 1.5 x maintenance rate and to try to transition to enteral diet
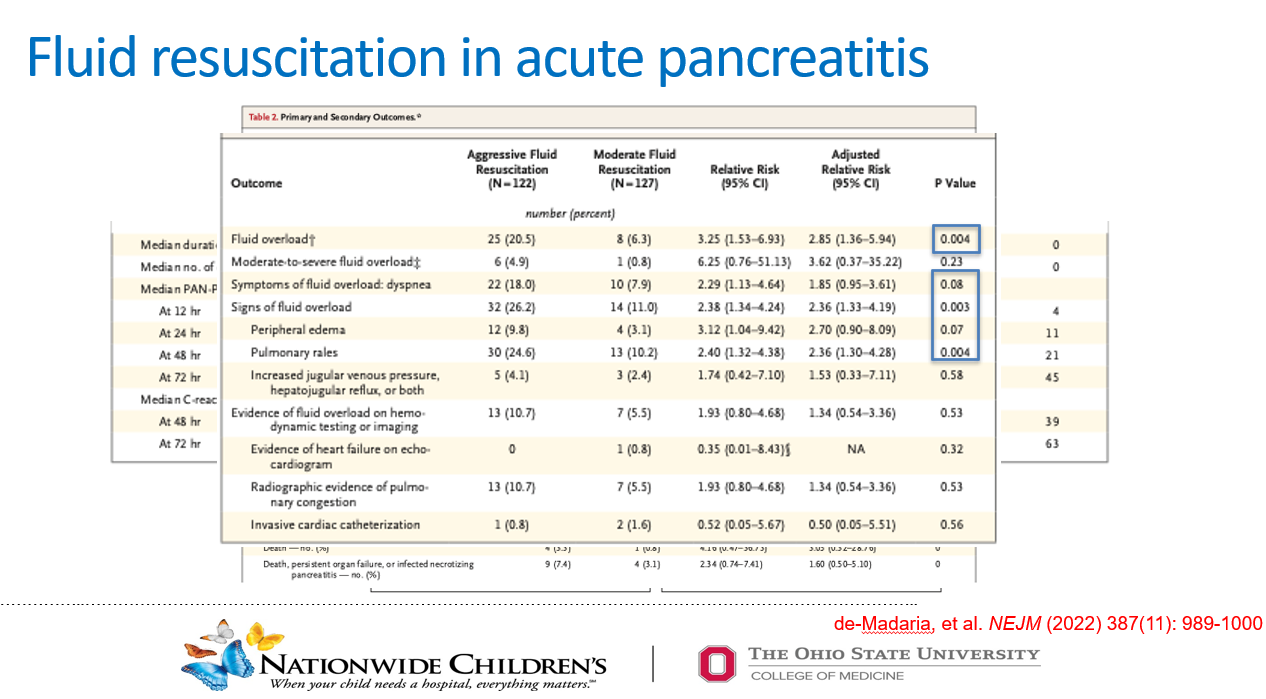
Aggressive fluid resuscitation of acute pancreatitis in adults is associated with increased risk of fluid overload. Lactated ringer’s is generally fluid of choice.
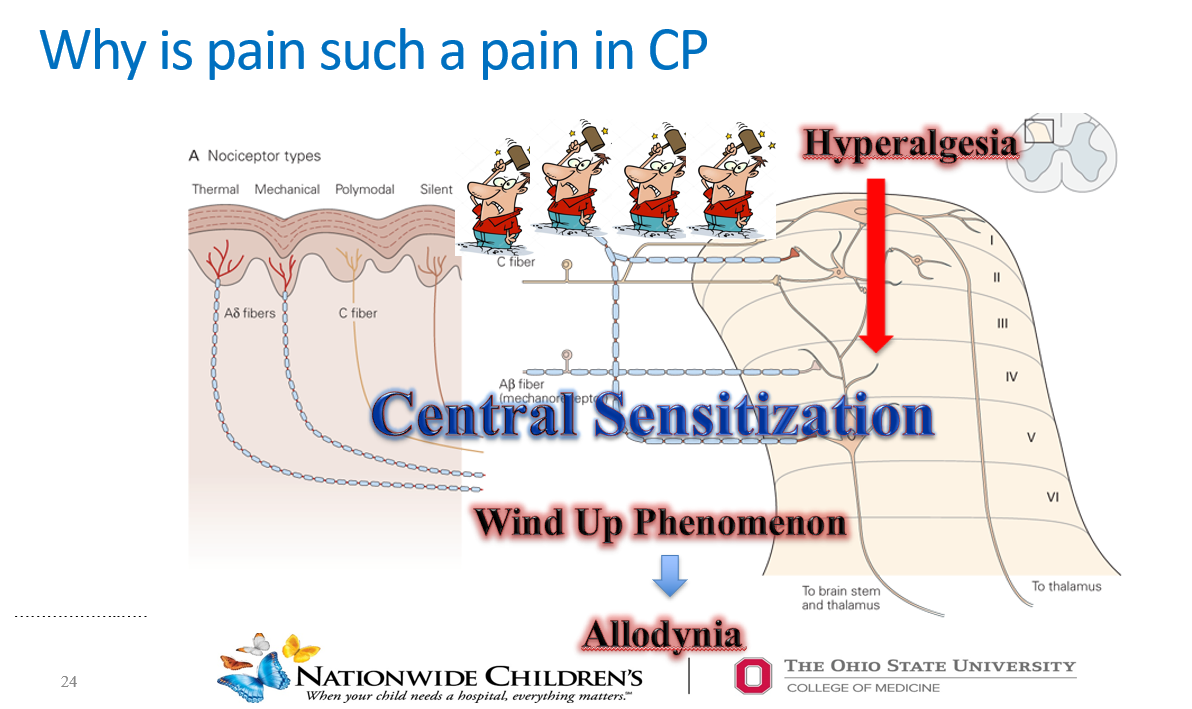
In this study with 211 pediatric patients, starting with a narcotic increases the likelihood of continuing with narcotics. Many patients can respond to acetaminophen and NSAIDs. Using narcotics, may increase the risk of sensitization to pain (lowering pain threshold)
In this study with adults (Not Randomized), use of PCA was associated with longer hospitalizations, slower start to enteral nutrition and increased narcotic use at discharge
A single episode of acute pancreatitis, even mild cases, is associated with long-term risks including risk of exocrine pancreatic insufficiency (often transient), increased risk of diabetes mellitus and even pancreatic cancer.
Restricting fat in the diet for 1-2 weeks after an episode may reduce some symptoms
Because of risk of complications, Dr. Freeman recommends follow up after hospitalization (after a few months) and for up to 5 years (at least for 2 years)
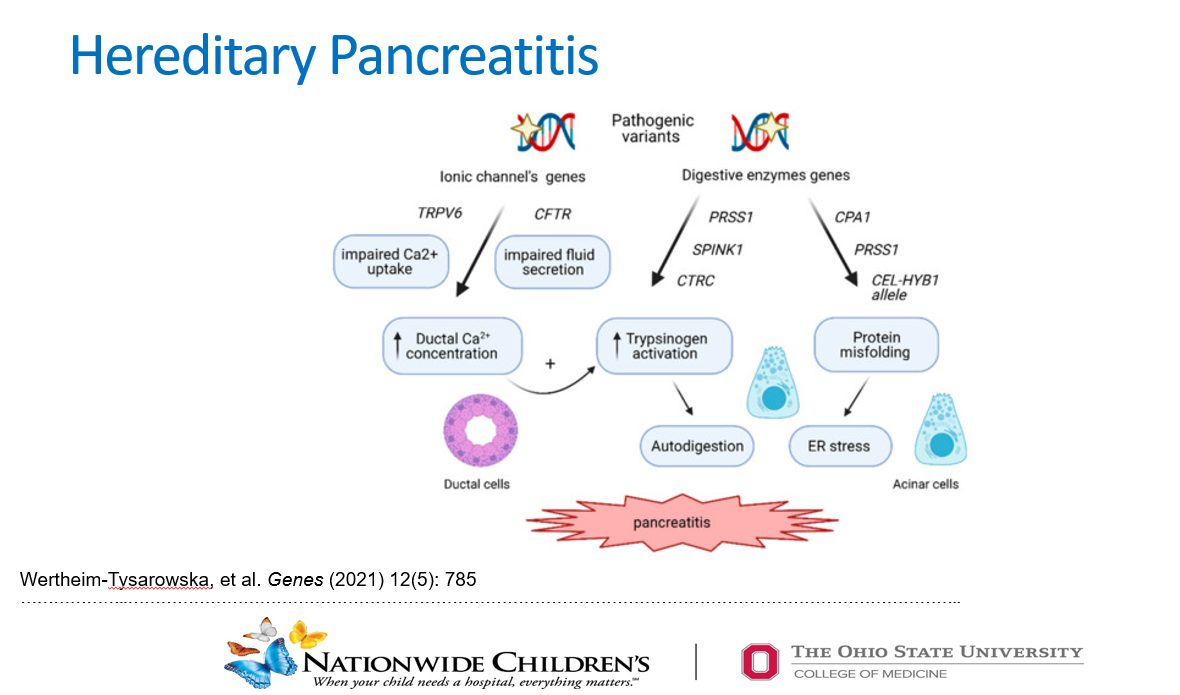
Dr. Freeman indicated that he recommends checking genetic tests for pancreatitis if a patient has had more than one episode. If a patient is less than 5 years of age or has a significant family history, checking for genetic predisposition should be considered with the first bout of pancreatitis.
Key points: Even patients with acute pancreatitis need follow-up. Consider using non-narcotic medicines as the first line, especially in patients who have not ‘failed’ these medications.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
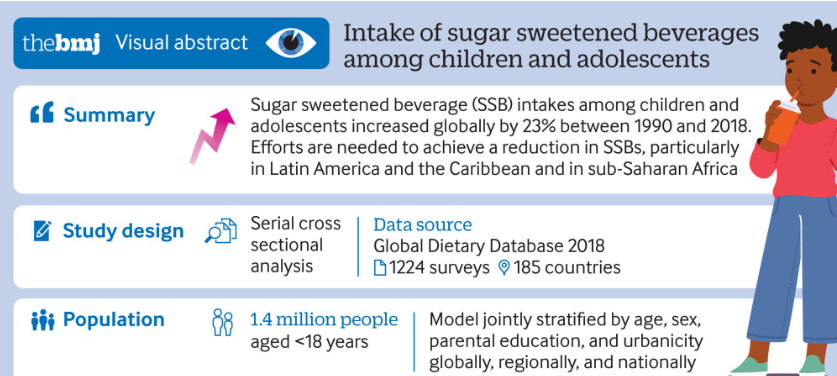
Intakes of SSBs among children and adolescents aged 3-19 years in 185 countries increased by 23% (0.68 servings/week (0.54 to 0.85)) from 1990 to 2018, parallel to the rise in prevalence of obesity among this population globally
High income countries experienced an overall decrease in intakes of SSBs from 2005 to 2018. This might be explained by the increasing scientific and public health attention on the harms of SSBs as well as obesity in these nations during this period, which may have led to increased media and public awareness about the harms to health associated with SSBs
National mean intakes of SSBs (standardized 248 g (8 oz) serving/week for this analysis) in children and adolescents aged 3-19 years across 185 countries in 2018. SSBs were defined as any beverage with added sugars and ≥209 kJ (50 kcal) per 237 g serving, including commercial or homemade beverages, soft drinks, energy drinks, fruit drinks, punch, lemonade, and aguas frescas. This definition excludes 100% fruit and vegetable juices, non-caloric artificially sweetened drinks, and sweetened milk
My take: Despite the knowledge that sugary beverages are detrimental, consumption continues to increase.
16 programs met the criteria for inclusion. None of these programs were in the Western U.S. Among feeding programs that were not included, there were 16 programs excluded due to lack of an intensive day program and 1 program excluded as admissions were on hold due to transition in leadership. .
“Results suggest current treatment capacity of <1000 slots per year.”
Estimates place pediatric feeding disorders as between 1 in 23 and 1 in 37 children under the age of 5 years. Thus, if 5% needed intensive care, this would equate to ~45,000 children under age 5 yrs. This estimate does not include children >5 yrs.
The discrepancy in need (~45,000) and availability (~1000) explains why wait times can be 12 months or longer.
My take: There is a huge mismatch between supply of intensive feeding therapy programs and demand. The potential barriers include training of sufficient numbers of qualified professionals, institutional support, and reimbursement,
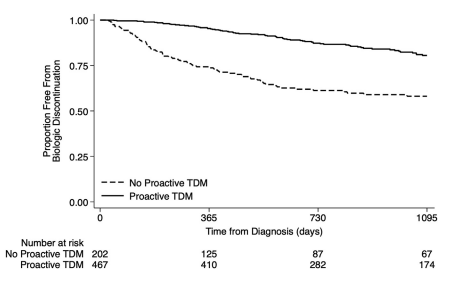
S Ali et al. Clinical Gastroenterology and Hepatology, Volume 22, Issue 10, 2075 – 2083.e1. Characterization of Biologic Discontinuation Among Pediatric Patients With Crohn’s Disease
Methods: Prospective ImproveCareNow registry data (n=823, from 7 centers) were supplemented with medical record abstraction.
Treatment/Monitoring:
86% started biologics (78% infliximab, 21% adalimumab, <1% others)
Twenty-six percent used concomitant immunomodulators for ≥12 months
Most (85%) measured TDM including 47% induction, 69% proactive, and 24% reactive
Key findings:
Twenty-nine percent discontinued their first biologic after median 793 days because of inefficacy (34%), anti-drug antibodies (8%), adverse events (8%), or non-adherence (12%)
Proactive TDM and concomitant immunomodulators were associated with 60% and 32% reduced biologic discontinuation
Half of patients discontinued biologics without trial of high-dose therapy and 14% without any evaluation
Among patients started with infliximab therapy, 62% of patients started at a dose of <6 mg/kg, 18% stared at a dose >8 mg/kg. 67% of patients underwent dose escalation. This is agreement with other studies indicating that as many as 80% of children need doses in excess of ‘standard’ dosing (5 mg/kg every 8 weeks)
In patients with anti-TNF medication inefficacy with TDM availability, 36% had infliximab or adalimumab levels below 5 mcg/mL. and 20% had levels between 6-8 mcg/mL.
Among patients who discontinued anti-TNF medications, 60% had serum trough levels less than 10 mcg/mL.
The rate of biologic durability was lower for those (n=61) receiving a 2nd biologic who had rates of remaining on agent of 56% at 1 yr, 28% at 2 yrs, and 10% at 4 yrs. In contrast, the first biologic had durability of 90% at 1 year, 79% at 2 years, and 66% at 4 yrs.
My take: This study strongly supports the use of proactive therapeutic drug monitoring. In addition, the authors make a compelling argument to optimize a therapy and evaluate carefully before switching to a new medication/biologic. Finally, the use of concomitant immunomodulators can improve medication durability; it is particularly important if needing to switch from one anti-TNF agent to another due to anti-drug antibodies.