M Najem, E Dong. N Engl J Med 2024;390: e47. Esophageal Varices, White-Nipple Sign, and Portal Hypertensive Gastropathy
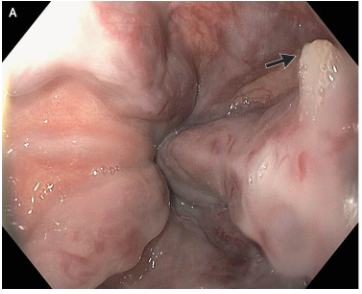
This case reported on a 66 year old with cirrhosis and variceal bleeding. “One varix had a “white-nipple sign” (Panel A, arrow), which indicates recent variceal hemorrhage and results from the formation of a fibrin plug at the site of a resolved thrombus.”
Related article: N Khan, A Shapiro. Case Rep Gastroenterol. 2011 May-Aug; 5(2): 386–390. The White Nipple Sign: Please Do Not Disturb
“Though not widely mentioned as a stigma of recent variceal hemorrhage, this finding was first reported by Chung and Lewis in 1984 [4]. They described it as a white nipple on top of a varix protruding into the lumen and noted its presence in up to 5% of cases of variceal bleeding. It was thought to represent a platelet-fibrin plug at the site of recent variceal rupture. They noted that dislodgement would be accompanied by jet-like bleeding and called it ‘Mount St. Helens’ sign’ due its volcanic-like eruption…As Chung and Lewis [4] initially suggested, it should ‘alert the endoscopist to take urgent measures to avert a disaster’. Recognizing it as such, attempts to dislodge the lesion must be avoided and endoscopic therapy should be undertaken.”
Related blog posts:
- New Paradigm in Treating Varices and Cirrhosis Management (in Adults)
- Why Carvedilol Is Considered Best Pharmaceutical Agent to Prevent Variceal Bleeding (in Adults)
- #NASPGHAN19 Liver Symposium (excellent presentation by Dr. Romero on varices in children and portal hypertension)
- Time to Adjust the Knowledge Doubling Curve in Hepatology For Platelets in the setting of cirrhosis: “Given the low risk of bleeding of many common procedures, potential risks of platelet transfusion, lack of evidence that elevating the platelet count reduces bleeding risk, and ability to use effective interventions, including transfusion and hemostasis if bleeding occurs, it is reasonable to perform both low‐ and high‐risk procedures without prophylactically correcting the platelet count...An individualized approach to patients with severe thrombocytopenia before procedures is recommended because of the lack of definitive evidence for safety and efficacy of interventions intended to increase platelet counts in patients with cirrhosis.” The authors note in Table 4, that the AASLD does not have a specific threshold for platelets, whereas other societies have used values of >30 or >50.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.