E Shah et al. JPGN 2024; 78: 608–613. Percutaneous electrical nerve field stimulation for adolescents with irritable bowel syndrome: Cost‐benefit and cost‐minimization analysis
Background: “Despite its favorable efficacy and safety profile, access to PENFS and other modalities in IBS can be limited by insurance coverage.”
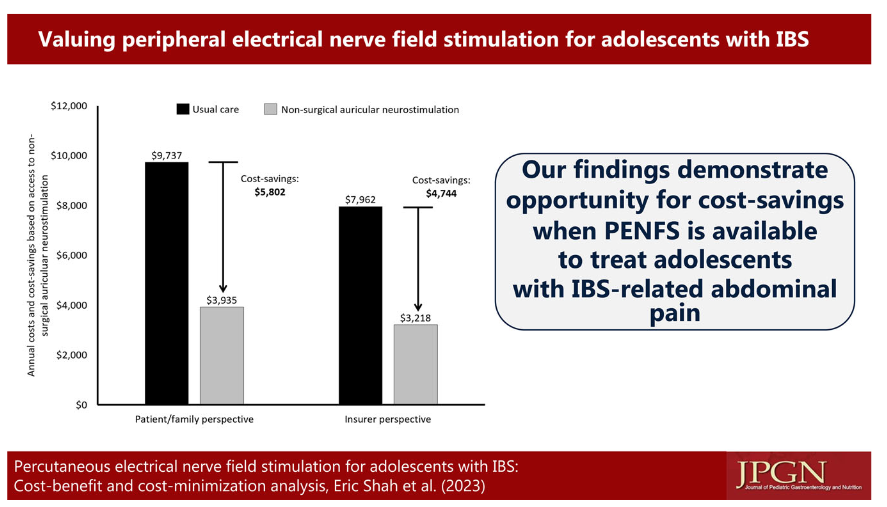
Methods: The authors performed an economic analysis to estimate cost‐savings for patients’ families and healthcare insurance, and health outcomes, based on abdominal pain improvement with percutaneous electrical nerve field stimulation (PENFS) with IB‐Stim® (Neuraxis). The authors created a a Markov model.
Key findings:
- PENFS was associated with 18 added healthy days over 1 year of follow‐up, increased annual parental wages of $5,802 due to fewer missed work days to care for the child, and $4744 in cost‐savings to insurance
- Important Limitation: The economic benefits that derive from the clinical improvements used in this analysis are based on a small prospective cohort study of 20 patients with up to 1 year of follow‐up
My take: It appears that auricular stimulation should be positioned earlier in treatment algorithms for adolescents with IBS based on safety, and efficacy, especially if cost is not prohibitive.
Related blog posts:
- Auricular Stimulation Associated with Less Pain, Less Disability, and Better Sleep
- Jose Garza: What’s New in Motility (Part 2)
- IB-Stim (Neuro-Stim) for Adolescents with Irritable Bowel
- Neuro-Stim for Refractory Cyclic Vomiting?