In this cross-over randomized controlled study with 50 children (median age 3.5 yrs), the authors assessed whether music therapy (MT) is effective to reduce pain during daily personal hygiene care (DPHC). The primary outcome was variation of the Face Legs Activity Cry Consolability (FLACC) score (range, 0-10). Key findings:
FLACC score was 0.0 (0.0-3.0) at baseline and 3.0 (1.0-5.5) during DPHC. With MT, these values were, respectively, 0.0 (0.0-1.0) and 2.0 (0.5-4.0).
Rates of FLACC scores of >4 during DPHC, which indicates severe pain, were 42% in standard conditions and 17% with MT (P = .013).
In their background, the authors note that MT “provides feelings of well-being and relaxation and acts as a distractor, leading to the inhibition of pain perception.”
My take: This study reinforces the importance of distraction to reduce pain. Life is better and less painful with music.
It used to be fairly easy to dismiss Florida’s surgeon general, Dr. Joseph A. Ladapo, as a clownish anti-vaccine quackposing a danger mostly to residents of his home state…Ladapo has moved from promoting useless treatments for COVID-19, such as the drugs hydroxychloroquine and ivermectin, to waging an ever-expanding fact-free campaign against the leading COVID vaccines…
That brings us to Ladapo’s latest adventure in medical quackery, his claim that no one should take the mRNA vaccines….Ladapo’s advice is based on what he says is research that the Pfizer and Moderna mRNA COVID vaccines contain fragments of DNA that are injected into human cells, which they can contaminate and turn into cancer cells…
The human cell has a panoply of mechanisms to destroy foreign DNA. Even if the fragments managed to penetrate the cell nucleus, which can’t happen, they would have to cut up the existing DNA, which would require a mechanism the fragments don’t have.
“So the chancethatDNA could affect yourDNA is zero,” Offit said..
Ladapo’s words and actions have surely contributed to his state’s pathetic performance in getting its citizens vaccinated against COVID. With 11.6% of its population fully vaccinated with a booster as of last May, Florida had a rate among the lowest in the nation. (California’s rate was 20.6%.) Among those 65 and older — purportedly the population that Florida strives to protect — only 31.2% were fully vaccinated. (California: 48.3%.)
Florida’s death rate from COVID of 375 per 100,000 people is among the worst in the country. (California: 283.) You can ignore the defense that the difference is due to Florida’s relatively older population; states with even older median ages have done much better: Vermont (170), New Hampshire (245) and Maine (252). The difference is the indifference of Ladapo and DeSantis to their own residents’ health.
The authors retrospectively utilized the University of Manitoba IBD Epidemiology Database includes all Manitobans diagnosed with IBD between 1984 and 2018 (n=5920). Key findings:
Rates of PPI use in control subjects increased gradually from 1.5% to 6.5% over 15 years
Persons with IBD had a higher rate of PPI use, peaking up to 17% within 1 year of IBD diagnosis with a rate ratio (RR) of 3.1
The authors noted an abrupt increase in PPI use within 6 months of an IBD diagnosis which could indicate that IBD-related symptoms are being mistakenly treated with a PPI or that IBD may increase reflux-related symptoms. Given the higher rate of PPI use in pre-IBD diagnosis patients, compared to controls, the authors note that “it is possible that their [PPI] use enhances the likelihood of an IBD diagnosis by their role in altering the gut microbiota.” In addition, they note that “a case-control study found that PPIs were associated with an increased risk of pediatric IBD” (NR Schwartz et al. J Pediatr Pharmacol Ther 2019; 24: 489-496).
My take: PPIs are being used more frequently. Whether PPIs are detrimental before or after a diagnosis with IBD is not clear.
This was a multicenter, randomized, placebo-controlled trial to compare the efficacy and safety of thiopurine-allopurinol versus thiopurine with placebo for adults commencing a thiopurine for IBD in 102 patients. Allopurinol was dosed at 100 mg. Key findings:
A higher proportion achieved the primary outcome (improved clinical score and fecal calprotectin <150) in the thiopurine-allopurinol group (50% vs 35%, p = 0.14) and fewer participants stopped their allocated therapy due to adverse events (11% vs 29%, p = 0.02
Medication exposure and disease outcomes were compared between 3 diagnostic periods: 1988 to 1993 (period [P] 1; pre-IS era), 1994 to 2000 (P2; pre-anti-TNF era), and 2001 to 2011 (P3; anti-TNF era).
Key finding: The risk of colectomy at 5 years decreased significantly over time (P1, 17%; P2, 19%; and P3, 9%; P = 0.045, P-trend = 0.027) and between the pre-anti-TNF era (P1 + P2, 18%) and the anti-TNF era (P3, 9%) (P = 0.013).
In this systematic review, the authors identified 8 eligible articles with 526 pediatric patients with IBD. Key finding: “There is no significant association between preoperative anti-TNF-α therapy and postoperative complications in children with IBD after intestinal resection.”
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
This was a retrospective case-control study with 33 patients who were off immunosuppression for at least 1 year. The median age at LT was 0.7 years. The median IS withdrawal time was 9 years after LT.
Key findings:
No differences in allograft rejection rates, IS complications, or c-IO [composite ideal outcome] prevalence were seen between SPLIT patients off IS and age- and sex-matched controls remaining on IS.
This is a highly-selected group representing ~0.5% of pediatric liver transplants (1996-2015).
My take: In this small sample size, patients off IS had similar outcomes as patients who continued on IS. Understanding this group better could help extend this approach to more patients.
This retrospective study compared the findings of children with probable autism (ASD) to age- and gender-matched controls with developmental delay (DD) or with typical development (TD), (n= 526 ASD, 526 DD, 1052 TD). Key findings:
Children with ASD had higher rates of abnormal esophageal histology (ASD 38.4%; DD 33.4%; TD 30.4%, P = .008)
Stomach findings did not differ significantly among the groups: histologic inflammation was identified in ASD 13.3%, DD 18.5%, and TD 22.4% (P=.10).
In the duodenum, histologic abnormalities were observed with lower frequency in ASD (ASD 17.0%; DD 20.1%; TD 24.2%, P = .005).
The authors emphasize the importance of the esophageal findings (increased rates of esophagitis). However, there are some important caveats that are not discussed in the paper:
At baseline (prior to study), it was known that the ASD and DD groups had higher rates of eosinophilic esophagitis: ASD 9.1%, DD 9.5%, and TD 7.4% (Table 1). In addition, both of these groups had higher rates of gastroesophageal reflux at baseline: ASD 7.6%, DD 8.0%, and TD 6.5%. This selection bias is likely to negate much of the esophageal differences observed in their study. Also, the ASD group had much higher numbers receiving H2 blockers at time of procedure: ASD 11.4%, DD 10.3%, and TD 6.4%.
In addition, the TD group had a much higher rate of abdominal pain as the indication for endoscopy (TD 26.6%, ASD 17.5%, and DD 20.2%). It is well-recognized that isolated abdominal pain has a low yield on endoscopy.
The authors do not discuss the elephant in the room. What is the significance of microscopic esophagitis (or microscopic gastritis or microscopic duodenitis)? Previous authors have noted that “15% of healthy individuals may have microscopic esophagitis” (Gastroenterology 2018 (volume 154; pages 263-451 -see page 291). When we were looking at the variation of diagnostic yield for endoscopy, we decided to focus on colonoscopy because of the high rates of microscopic inflammation in the upper GI tract (related blog post: Our Study: Provider Level Variability in Colonoscopy Yield)
My take: In their discussion, the authors state that this study represents “significant progress in the understanding of gastrointestinal pathophysiology in children with ASD…suggest a unique fingerprint of findings in children with ASD.” In my view, the authors showed similar yield of EGD histologic abnormalities in all three groups and these microscopic findings are of uncertain significance.
The study, published in JAMA on Tuesday, found that, in the three years after a private equity fund bought a hospital [51 hospitals in study], adverse events including surgical infections and bed sores rose by 25 percent among Medicare patients when compared with similar hospitals that were not bought by such investors. The researchers reported a nearly 38 percent increase in central line infections, a dangerous kind of infection that medical authorities say should never happen, and a 27 percent increase in falls by patients while staying in the hospital…
Although the researchers found a significant rise in medical errors, they also saw a slight decrease (of nearly 5 percent) in the rate of patients who died during their hospital stay. The researchers believe other changes, like a shift toward healthier patients admitted to the hospitals, could explain that decline. And by 30 days after patients were discharged, there was no significant difference in the death rates between hospitals…
The researchers said the most likely explanation for the increased errors was fewer hospital employees, an effect that has been measured in other studies of private equity.
My take: Private equity (PE) investment is likely to result in a lower quality of care in most circumstances. The primary driver of PE is profits not people. In order for PE to achieve their goals, it necessitates either driving up costs (higher profit margin) or reducing costs/staffing.
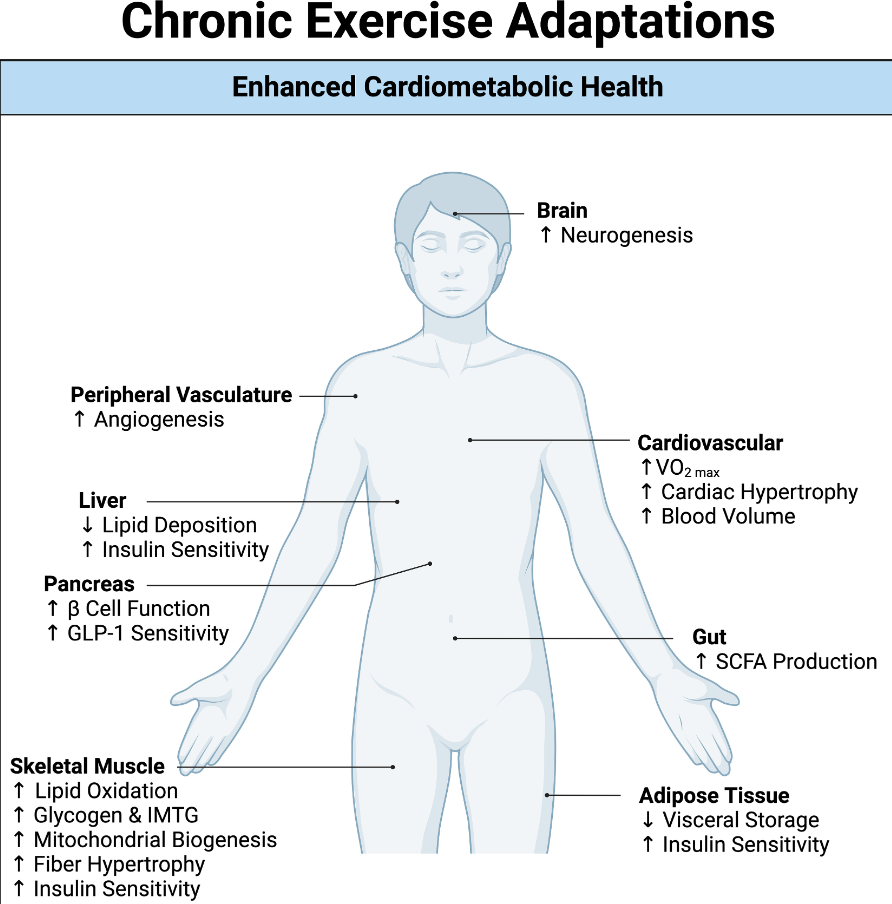
“The risk associated with multiple cancers, cardiovascular disease, diabetes, and all-cause mortality is decreased in individuals who meet the current recommendations for physical activity…Over time, the associated metabolic stress of each individual exercise bout provides the basis for long-term adaptations across tissues, including the cardiovascular system, skeletal muscle, adipose tissue, liver, pancreas, gut, and brain. Therefore, regular exercise is associated with a plethora of benefits throughout the whole body, including improved cardiorespiratory fitness, physical function, and glycemic control. Overall, we summarize the exercise-induced adaptations that occur within multiple tissues and how they converge to ultimately improve cardiometabolic health.”
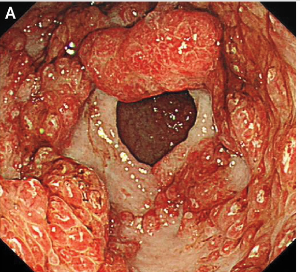
JCT Lai et al. NEJM 2023; 389: 2377-2385. Case 39-2023: A 43-Year-Old Woman with Chronic Diarrhea, Hair Loss, and Nail and Skin Changes
This case presents a polyposis disorder seen in adults and provides a useful differential diagnosis: autoimmune disorders including IBD, vasculitis, and celiac, primary adrenal insufficiency, heavy metal poisoning, amyloidosis, and cancer. This rare disorder has a reported “5-year mortality of 55%, mostly due to complications such as sepsis and gastrointestinal bleeding”
A few of the images from Figure 2:
Numerous sessile polyps in colonFrom Stomach
ChatGPT’s explanation of Cronkhite-Canada Syndrome:
Cronkhite-Canada syndrome (CCS) is a rare, noninherited, sporadic gastrointestinal polyposis syndrome that affects various parts of the digestive system. It is characterized by the presence of multiple polyps in the stomach and colon, as well as other distinctive features.
Epidemiology: Cronkhite-Canada syndrome is a very rare disorder, with only a few hundred cases reported worldwide. It typically affects older adults, with an average age of onset around 60 years, and there is no known genetic predisposition.
Clinical Presentation: Patients with Cronkhite-Canada syndrome often present with a combination of gastrointestinal and dermatological symptoms. The gastrointestinal manifestations include diarrhea, abdominal pain, weight loss, and protein-losing enteropathy. The dermatological symptoms consist of characteristic changes such as nail atrophy, hyperpigmentation, alopecia (hair loss), and skin hyperpigmentation.
Gastrointestinal Findings:
Polyposis: Multiple [hamartomotous] polyps are found in the stomach and colon. These polyps can vary in size and number.
Diarrhea and Abdominal Pain: Chronic diarrhea and abdominal pain are common symptoms due to the involvement of the digestive tract.
Dermatological Findings:
Nail Changes: Nail atrophy, ridges, and splitting are commonly observed.
Skin Changes: Hyperpigmentation of the skin, especially on the palms and soles, is a distinctive feature.
Alopecia: Hair loss is often present.
Laboratory Findings: Patients with Cronkhite-Canada syndrome may exhibit laboratory abnormalities, including hypoalbuminemia (low levels of albumin in the blood), hypoproteinemia, and electrolyte imbalances due to protein loss in the gastrointestinal tract.
Diagnosis: Diagnosis is based on a combination of clinical presentation, endoscopic findings, and pathology results from biopsies of the affected gastrointestinal tissue.
Treatment: Management of Cronkhite-Canada syndrome involves a multidisciplinary approach. Nutritional support is essential, and patients may require supplementation of protein and nutrients. Corticosteroids are often used to suppress inflammation, and immunosuppressive agents may be considered in refractory cases. Regular surveillance endoscopy is necessary to monitor polyp growth and assess response to treatment.
This study analyzed “pH impedance testing in the NICU in 516 infants with symptoms of arching and irritability. A nurse was assigned to document episodes of arching and irritability during the study.”
Key findings:
Acid reflux and impedance bolus characteristics were not significantly different between infants with >72 and ≤72 arching/irritability events (P ≥ .05)
Arching/irritability events had an 8% sensitivity for reflux (3062/39,962). The specificity of arching/irritability for NOT being reflux was 94% (246,462/262,534)
Oral feeding was associated with more arching and irritability than tube feeding
“The study found that <10% of the clinical episodes were associated with acid reflux but episodes of arching and irritability were more common in infants with preterm birth, neurologic injury, or chronic lung disease.”
My take (in part, borrowed from authors): “Acid GER disease is unlikely the primary cause of arching/irritability and empiric treatment should not be used when arching/irritability is present.” Unfortunately, getting physicians to curtail the use of ineffective acid blockers in infants is a not making headway (Unfavorable Trends in Reflux Management of Infants) There is definitely enough material with reflux to devote a whole MythBusters show.
In addition to not being the main reason for arching,
Reflux is not a frequent reason for BRUEs
Reflux cannot be reliably-identified by ENTs. Red airway appearance is NOT indicative of reflux (poor specificity, poor sensitivity)
Reflux in infants does not improve with PPIs (more than placebo)
Fundoplication does not result in fewer hospitalizations or improve pulmonary outcomes
Treating reflux does not improve asthma and probably does not help throat symptoms either
Many kids (and adults) with “reflux” don’t have reflux