
Also -some tweets from IBD meeting:


Also -some tweets from IBD meeting:
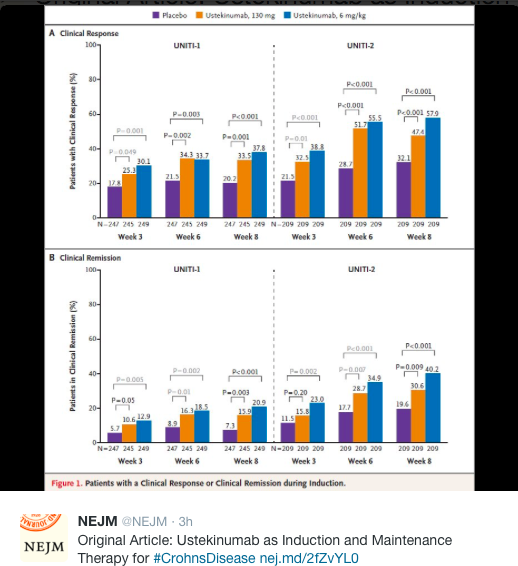
A recent study (BG Feagan, WJ Sandborn et al NEJM 2016; 375: 1946-60) provides extensive data regarding the effectiveness of ustekinumab for Crohn’s disease.
This publication combines three trials (industry-sponsored): UNITI-1, UNITI-2, and IM UNITI. The first two trials with 741 and 628 patients respectively examined intravenous ustekinumab for induction. Patients (18 years or older with Crohn’s disease) received either 130 mg, 6 mg/kg or placebo. UNITI-1 were patients with primary or secondary nonresponse to TNF antagonists. UNITI-2 were patients in whom conventional therapy failed or in which unacceptable side effects developed. The majority of UNITI-2 patients had not received a TNF antagonist.
IM UNITI with 397 patients followed patients who completed the first two trials for maintenance (90 mg SC every 8 weeks or every 12 weeks). For this study, the primary end point was remission at week 44 (CDAI score <150).
The IM UNITI study involved 260 sites in 27 countries.
Key findings:
When looking at more objective results, both UNITI-1 and UNITI-2 showed significant drops in calprotectin and CRP values; both of these objective markers favored 6 mg/kg over 130 mg fixed induction dose.
Safety:
Extensive safety data are reported and more than 60% of all patients, including placebo-treated patients reported potential adverse effects. Adverse effects and serious adverse effects were similar in treatment and control groups. During 1 year of therapy, there were no deaths or instances of the reversible posterior leukoencephalopathy syndrome.
Other points:
My take: These data support the use of ustekinumab for Crohn’s disease, particularly in patients who have not responded to other therapies.
Here’s a link summarizing FDA approval: Medscape: FDA Clears Ustekinumab (Stelara) for Crohn’s Disease
An excerpt:
The US Food and Drug Administration (FDA) has approved ustekinumab (Stelara, Janssen Biotech, Inc) for the treatment of moderately to severely active Crohn’s disease in patients aged 18 years or older.
Specifically, the interleukin-12/23 inhibitor is indicated for Crohn’s patients who have failed or were intolerant to immunomodulator or corticosteroid therapy but who never failed treatment with a tumor necrosis factor (TNF) blocker or who failed or were intolerant to treatment with one or more TNF blockers, according to a company news release.
Ustekinumab is already approved in the United States for treatment of patients with plaque psoriasis and psoriatic arthritis…The clinical development program for ustekinumab for Crohn’s disease included more than 1300 patients across three pivotal phase 3 studies, which served as the primary basis for FDA approval.
In clinical studies of patients who were either new to, experienced with, or failed anti-TNF therapy, between 34% and 56% of patients experienced symptom relief in the 6 weeks after receiving a one-time intravenous induction dose of ustekinumab. “Noticeable improvement was observed as early as 3 weeks,” the company said.
Most patients who responded to induction dosing and who continued ustekinumab treatment with subcutaneous maintenance doses every 8 weeks were in remission at the end of 44 weeks (52 weeks from initiation of the induction dose), the company said.
Full prescribing information and a medication guide are available online.
G Wahbeh et al. JPGN 2016; 63: 348-51. This retrospective case series with 4 children (aged 12-17 years) indicated that 2 had a ‘clinical response’ to ustekinumab therapy, though one of these had ongoing elevation of CRP. The dosing may have been too low: 90 mg at week 0 and 4, then every 8 weeks. My take: This study shows that ustekinumab’s use in pediatric IBD seems to be a ‘shot in the dark’ given the lack of coherent data.
Related posts:
L Zimmerman et al. JPGN 2016; 63: 352-56. Among a cohort of 123 children who had underwent a bowel resection, from 1977-2011, the overall postoperative complication rate was 13%. This included 3 of 24 who had prior infliximab and 9 of 99 who had not received infliximab. It is noteworthy that the infliximab group had more corticosteroid exposure. The authors concluded that preoperative infliximab was not associated with increased complications but noted that their sample size was small. My take: Studies of adults with Crohn’s disease have yielded conflicting results on whether preoperative infliximab increases the risk of complications. This study shows that children likely have a lower rate of postsurgical complications and more pediatric specific data are needed.
Related post:
From KT Park’s Twitter Feed:


More data emerging that indicates that subcutaneous ustekinumab will be useful for refractory Crohn’s disease: S Khorrami et al. Inflamm Bowel Dis 2016; 22: 1662-69.
Another strategy for managing inflammatory bowel disease is using allopurinol which can help low-dose azathioprine achieve therapeutic levels. In the largest cohort to date, Pavlidis et al (Inflamm Bowel Dis 2016; 22: 1639-46) showed that at the end of followup (median 19 months after treatment initiation) 113/164 (69%) of patients with Crohn’s disease and 83/136 (61%) with ulcerative/unclassified colitis had a clinical response; 52% and 54% respectively were in remission. The azathioprine dose was 25% of weight-based monotherapy dose adjusted based on TPMT status; thus, for normal/high TPMT activity, azathioprine was dosed at 0.5 mg/kg whereas for heterozygous/intermediate activity, azathioprine was dosed at 0.25 mg/kg.
Related blog posts:
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications/diets (along with potential adverse effects) should be confirmed by prescribing physician/nutritionist. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.

Vickery Creek, Sandy Springs
This blog entry has abbreviated/summarized this terrific presentation; most of the material has been covered in this blog in prior entries (can use search function to find additional relevant material) but still this was a useful review. Though not intentional, some important material is likely to have been omitted; in addition, transcription errors are possible as well.
Emerging Therapies in IBD –Dr. Gary Lichtenstein
Background: This lecture started with a review of current therapies. We have learned how to use our current therapies better. There still remain a large number of patients that face surgery with IBD; though there has been improvement (?50% reduction).
Issues with thiopurines were reviewed. May take 2-6 months to take effect, though monotherapy with thiopurines are fairly ineffective for Crohn’s disease as initial therapy.
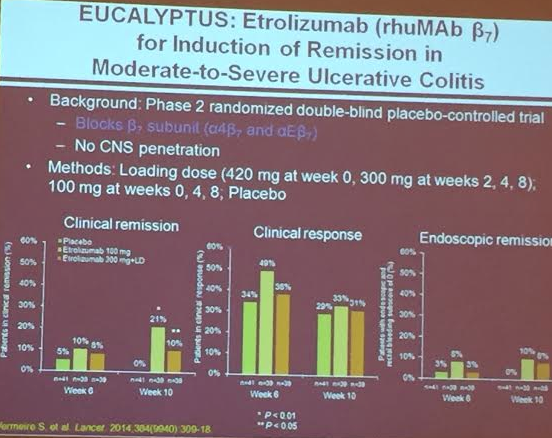
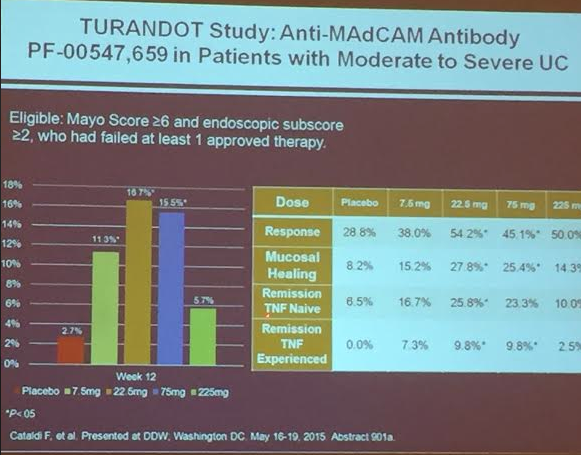
Leukocyte Trafficking Agents:
PF-00547,659
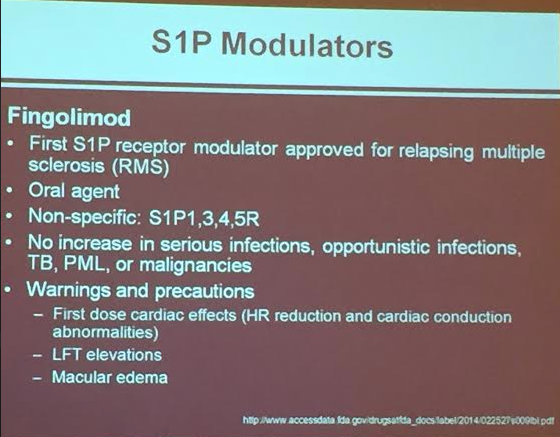
S1P Modulators:
Fingolimod
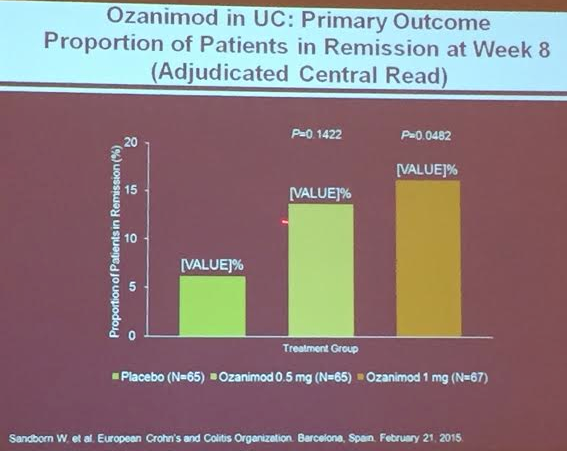
Ozanimod (RPC1063) (oral agent, fairly rapid onset) causes S1P-r on lymphocytes to be internalized –more selective than Fingolimod. Good safety has been noted thus far. No notable cardiac problems. Infrequent elevations of transaminases; this issue will need to be followed.
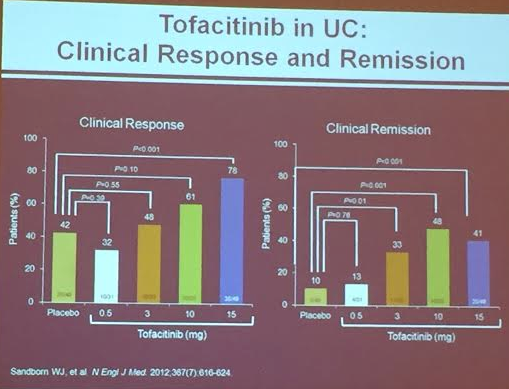
Tofacitinib oral Janus Kinus (JAK) Inhibitor (Sanborn WJ et al. NEJM 2012; 367: 616-24). Dr. Lichtenstein thinks 10 mg will be recommended dose. Follow lipids. For UC
Mongerson related post: Mongerson -Phase II Data Available in NEJM | gutsandgrowth
Ustekinumab
Related article from GI & Hep News: Ustekinumab for complex Crohn’s from ECCO conference/UNITI-1 Study (n=741)
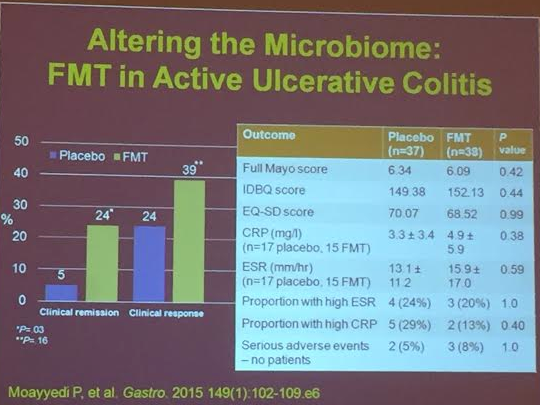
FMT. Further studies are needed
This blog entry has abbreviated/summarized this terrific presentation; most of the material has been covered in this blog in prior entries but still this was a useful review. Though not intentional, some important material is likely to have been omitted; in addition, transcription errors are possible as well.
2nd Lecture: What is Next in Treatments for Pediatric Patients? –Dr. Michael Rosen
I really enjoyed meeting Dr. Rosen. He is super-friendly and knowledgeable.
Combination therapy. Grossi V et al showed improvement in infliximab durability with concomitant therapy.



Now starting COMBINE trial (ImproveCareNow)–randomized to low dose MTX or placebo in combination with anti-TNF agent.

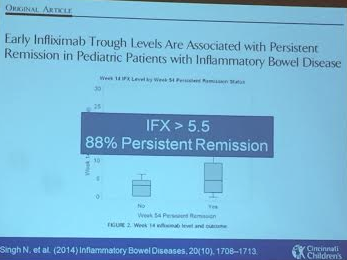
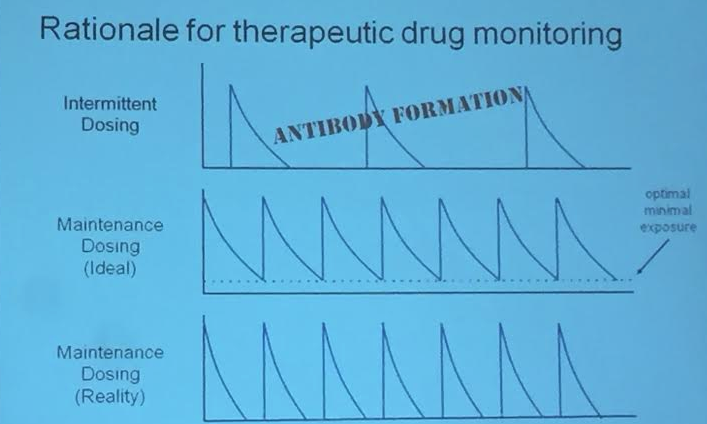
Therapeutic drug monitoring in pediatrics. Is this an alternative to combination therapy? Rationale (see slide): lower antibody formation if trough levels maintained. IFX level >5.5 associated with persistent remission (Singh et al 2014). Children are growing and they may need more adjustments. In Cincy, checking levels at week 14 after initiation and then every 6-12 months.
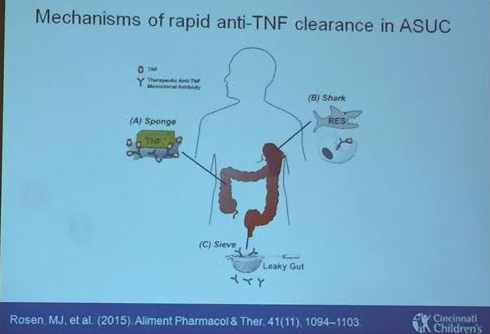
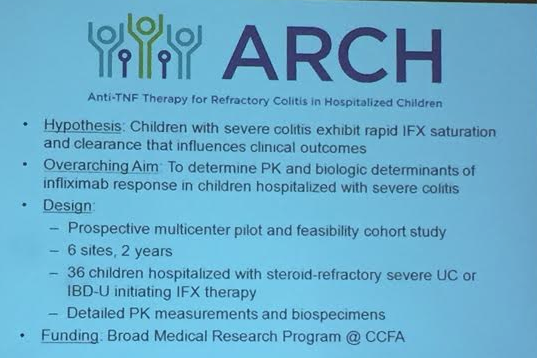
Acute Severe Ulcerative Colitis. High rates of dose escalation in this population. Some of this is due to more rapid clearance of anti-TNF –leaking in gut and other mechanisms as well. Week 8 level of 40 associated with clinical response. Thus, this population may benefit from 10 mg/kg at start (in those with albumin <3) and may need more frequent dosing, especially early into treatment (?0, 2, 6, 10). ARCH study to look into this further
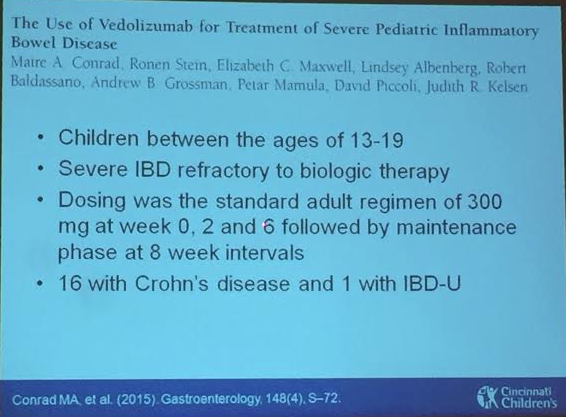
Vedolizumab. Conrad MA 2015. About 1/3rd of these refractory patients in this abstract responded.

Ustekinumab . IL-12 & IL-23 blockage. No studies in pediatrics. Case report reviewed of good response in a refractory case.
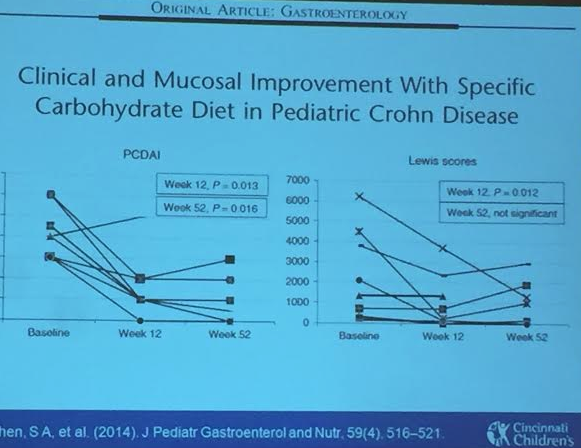
Enteral therapy. Specific carbohydrate diet experience. These diets have some published data, most retrospective studies. Our group (Cohen SA et al) did perform a small prospective study. Sigall-Boneh R et al showed improvement with partial enteral nutrition.




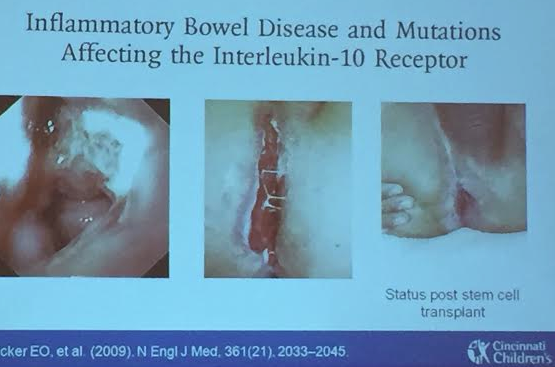
Very early-onset of IBD. IL-10 receptor deficiency was a key early discovery and can be treated with stem cell transplant. STAT3 mutation case reviewed which was managed with tocilizumab. More targeted therapy expected based on specific mutations.
G Broms et al (Clin Gastroenterol Hepatol 2016; 14: 234-41) provide more data on the ‘low risk of birth defects for infants whose mothers are treated with anti-tumor necrosis factor agents during pregnancy.”
From a Danish/Swedish cohort of 1,272,424 live births (2004-2012), the authors found the following (in comparison to healthy infants):
Limitations:
My take: Overall there is a slightly but not significantly increased risk in birth defects based on the use of anti-TNF therapy. Stopping anti-TNF therapy is likely to be more detrimental.
Briefly noted: P Wils et al. Clin Gastroenterol Hepatol 2016; 14: 242-50. This retrospective study of 122 patients showed that 65% had a clinical benefit within 3 months of receiving ustekinumab for Crohn’s disease refractory to anti-TNF therapy. Concomitant immunosuppressant therapy was associated with an increased likelihood of benefit (OR 5.43)
Related blog posts:
This study of Ustekinumab (aka Stelara) was different than previous studies (see previous gutsandgrowth blog from 2012: Ustekinumab for Crohn’s disease) in that this study targeted patients who were NOT ant-TNF failures; however, about 80% of patients had failed corticosteroids.
An excerpt:
Ustekinumab, a monoclonal antibody targeted against interleukins 12 and 23 (IL-12 and IL-23)…
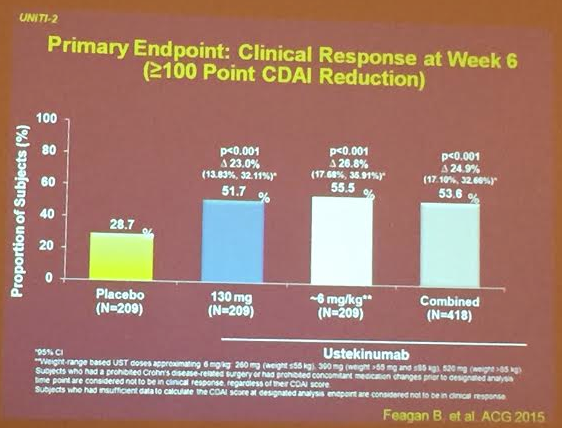
The trial, called UNITI-2, enrolled patients with moderate to severe Crohn’s disease who had failed traditional therapies but were naive to or at least had not failed a tumor necrosis factor (TNF) inhibitor…
In UNITI-2, 628 patients were randomized to placebo, 130 mg of ustekinumab in a fixed subcutaneous dose of 130 mg, or a weight-based dose of 6 mg/kg of subcutaneous ustekinumab…The primary endpoint was a CDAI reduction of at least 100 points at 6 weeks. Clinical remission at 8 weeks, defined as CDAI less than 150, was a secondary endpoint.
The primary endpoint was reached by 28.7% randomized to placebo, 51.7% of those randomized to the fixed dose of ustekinumab, and 55.5% of those randomized to weight-based dosing. The advantage for the active treatment arms was statistically significant (both P less than .001). For the secondary endpoint of clinical remission at 8 weeks, the rates were 19.6% for placebo, 30.6% (P = .009 vs. placebo) for fixed-dose ustekinumab, and 40.2% (P less than .001 vs. placebo) for the weight-based dose…
Ustekinumab was well tolerated with similar rates and types of adverse events reported in the active treatment and placebo groups.
My take: This study indicates that ustekinumab is likely to be another treatment option for patients with Crohn’s disease.
Ustekinumab is emerging as an option for inflammatory bowel disease. A study examining its effectiveness for TNF-refractory Crohn’s disease has been published (NEJM 2012; 367: 1519-28).
In this trial, members of CERTIFI (Crohn’s Evaluation of Response to Ustekinumab Anti-Interleukin-12/23 for Induction) from 153 centers in 12 countries assessed the efficacy of Ustekinumab in 526 adult patients. The primary outcome was a clinical response (CDAI >100 point drop) at 6 weeks.
Ustekinumab (currently approved for plaque psoriasis) is a ‘fully human IgG1κ monoclonal antibody’ which blocks the activity of interleukin-12 (IL-12) and interleukin-23 (IL-23) by inhibiting receptors on T cells, natural killer cells, and antigen-presenting cells. IL-12 and IL-23 have been implicated in the pathophysiology of Crohn’s disease.
This study of ustekinumab was a 36-week randomized, double-blind, placebo-controlled phase 2b trial. The first 8 weeks were for induction. After induction, based on response, patients were enrolled in a 28-week maintenance phase. Initial dosing was 1, 3, or 6 mg/kg of intravenous ustekinumab or placebo. Maintenance dose was 90 mg subcutaneously.
Patients were permitted to continue receiving stable doses of drugs. However, entry requirements included a washout period for intravenous glucocorticoids (3 weeks), TNF antagonists (8 weeks), and natalizumab (12 months).
Results:
Overall, in this study, patients dosed at 6 mg/kg during induction were more likely to have a response but not more likely to have a remission. Since all patients in this study had failed at least one TNF antagonist and 50% had failed at least two, the benefit of ustekinumab in other Crohn’s disease patients remains undefined.
Related blog entries:
CHOOSE TNF TRIAL | gutsandgrowth
