
A recent randomized controlled trial study (Gastroenterol 2015; 148: 1311-9) examined the effectiveness of larazotide acetate in 342 adults with Celiac disease (CD) who had ongoing symptoms despite the use of a gluten-free diet for at least 12 months.
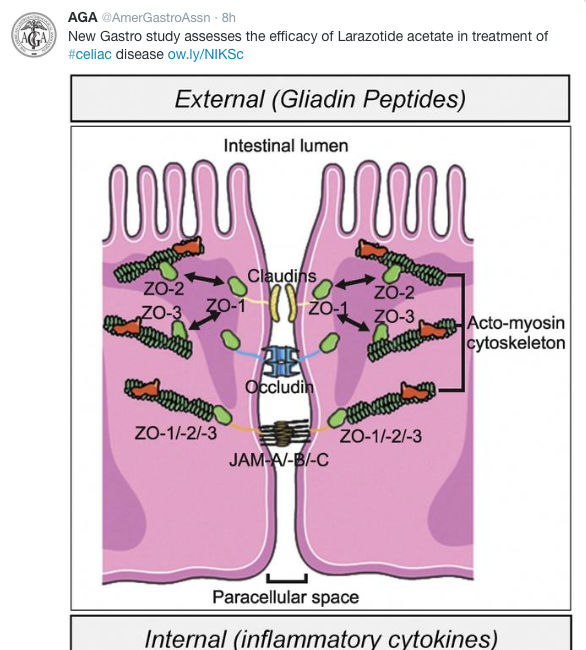
Larazotide acetate is a locally acting, nonsystemic 8-amino acid oral peptide which is a tight junction (TJ) regulator. “Larazotide acetate appears to prevent opening of intestinal TJs by promoting TJ assembly and actin filament rearrangement, which prevents gluten from reaching the intestinal submucosas and triggering an inflammatory response.”
Patients received either placebo, 0.5 mg, 1 mg, 2 mg three times daily. The majority of patients had normalized serology at the start of the study. Key findings:
- “The 0.5 mg dose showed a 26% decrease in celiac disease patient-reported outcome symptomatic days (P =.017), a 31% increase in improved symptom days (P =.034), a 50% or more reduction from baseline of the weekly average abdominal pain score for 6 or more of 12 weeks of treatment (P =0.022), and a decrease in the nongastrointestinal symptoms of headache and tiredness (P =0.010).”
- The 1- and 2-mg doses were no different from placebo for any end point.
- Safety was comparable to placebo.
The authors state that is unclear why the higher doses were not effective “but may involve peptide aggregation … reducing activity in vivo.”
Bottomline: There would be a benefit for an adjunct to a gluten-free diet due to the difficulty in adherence and due to ongoing symptoms in some despite the use of a GFD; in some cases, symptoms may be induced by inadvertent deviation from GFD. More data is needed to determine if larazotide acetate will be useful in this role.
Related blog post: Good Educational Two Minute Celiac Video | gutsandgrowth







