For those unable to grasp the fact that the current EPA director is harmful to our health, it may not be their fault. According to this commentary (VA Rauh. N Engl J Med 2018; 378:1171-1174), organophosphates like chlorpyrifos have likely resulted in the loss of ~17 million IQ points among 0 to 5 year olds; by extrapolation, this affects those older than 5 years too. Link: Polluting Developing Brains — EPA Failure on Chlorpyrifos
An excerpt: The regulatory plan developed by the U.S. Environmental Protection Agency (EPA) just before the 2016 elections was excellent: revoke all allowances for foods to contain residue of the organophosphate insecticide chlorpyrifos (“food tolerances”), essentially prohibiting agricultural and all remaining uses of the chemical… A total ban was the logical conclusion after decades of risk assessment showing increasing evidence of threats to human health, and children’s safety in particular…
However, the plan was scrapped in March 2017 by incoming EPA Administrator Scott Pruitt, who overrode the recommendation of agency scientists to ban all commercial use of chlorpyrifos… this action essentially violates the EPA’s statutory duty to protect human health, ignoring explicit child health policy dating back to 1995 that requires all national public health standards to address the special vulnerability of infants and children…
Harmful effects of chlorpyrifos on the developing brain are hardly surprising, given that this chemical was initially developed to attack the nervous system by inhibiting neurotransmitters in the body. First introduced as nerve-gas agents during World War II, organophosphate chemicals were later repurposed by chemical companies as insecticides and other pesticides…
Among the most worrisome findings are the corroborative results from several prospective cohort studies of children, which show an inverse dose–response effect of prenatal exposure to chlorpyrifos on cognition at 7 years of age..
In fact, one review (assuming a population of 25.5 million children 0 to 5 years of age in the United States) calculates a total loss of 16.9 million IQ points due to exposure to organophosphates, of which chlorpyrifos is the most widely used..
Because adult occupational exposures to chlorpyrifos have been clearly linked to Parkinson’s disease, there is good reason to worry that early exposures may set in motion a pathogenic trajectory potentially leading to neurodegenerative disease…
The EPA …may be putting an entire generation of young brains in harm’s way.

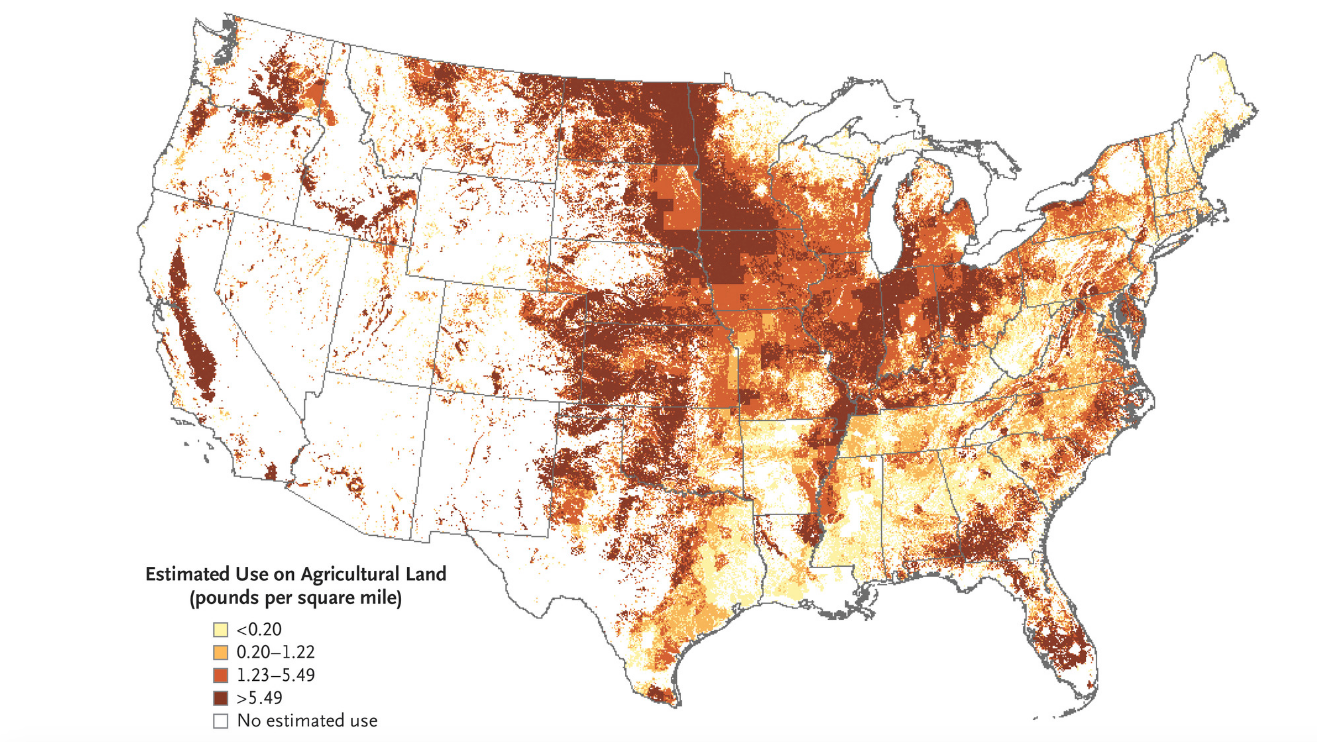
Estimated Agricultural Use for Chlorpyrifos, 2015 (Preliminary).
Estimates are from the U.S. Geological Survey National Water-Quality Assessment Project.