A recent clinical report (E Barfield et al. JPGN 2018; 66: 680-86) will be influential. This guideline is from the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition. Congratulations to my partner, Chelly Dykes, who is one of the coauthors.
Full text: Assuring Quality for Non-Hospital Based Biologic Infusions in Pediatric Inflammatory Bowel Disease: A Clinical Report from the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition
For many years, our office has had an office-based infusion center which has provided infusions in a safe and cost-effective manner. Recently, there have been some situations in which home-based infusions have been proposed either to lower costs and/or for convenience. This report succinctly describes the hurdles that need to be addressed before recommending this treatment pathway. As noted below, patient safety encompasses a great deal more than infusion reactions. Delays in infusions (which can increase risk of loss of response) due to reactions and lapses in communication are additional issues.
Recommendation 1: Home- or office-based infusions should ensure safe administration of the biologic infusion, provide reliable execution of infusion-related orders (eg, laboratories for therapeutic drug monitoring, dose optimization protocols, etc), and be equipped to recognize and respond to potential complications.
- Infusion reactions: ” Infusion reactions associated with infliximab and vedolizumab can range from mild reactions such as fever and chills, dyspnea, pruritus, or urticaria (in approximately 5%–10%), to severe reactions including anaphylaxis, convulsions, and hypotension (<1%)”
- Emergencies: “In the event of an urgent or emergent reaction during home- or office-based infusions, the in-home services agency (IHSA) nurse needs to be able to contact the appropriate ordering medical team member expeditiously by phone or pager to review/clarify specific concerns or needs to have an established clear policy on how to proceed with managing the reaction.”
- Communication: “We identified the lack or inconsistency of on-call coverage by the primary medical team when home- or office-based infusions occur as a significant barrier to safely initiating or continuing home- or office-based infusion programs. Difficulty in reaching a knowledgeable team member is a breach in reliable care and represents serious patient risk.”
- Related work: “In addition to administering the biologic infusion, executing all other infusion-related orders is an important safety consideration. Implementing unique home infusion protocols is linked to treatment efficacy.”
Recommendation 2: Pediatric home- or office-based infusions, particularly for patients 12 years and younger, should be staffed by a pediatric nurse professional with Pediatric Advanced Life Support (PALS) certification and clinical experience with pediatric patients.
Recommendation 3: Evidence-based standard of care for biologic therapy maximizing effectiveness and treatment sustainability should be established before initiating home or office-based infusions.
Recommendation 4: Home- or office-based infusion pathways that decrease opportunity loss for patients and families and deliver high-quality, patient-centered care should be supported and reproduced.
Recommendation 5: Pediatric gastroenterologists should ensure appropriate shared liability with IHSAs to deliver high-quality care in home-based infusions for children by executing pragmatic steps as outlined below:
- “Document discussion with the patient and family about the indication, risks, and adverse event management …
- Refer the patient to an accredited, licensed IHSA based on patient’s insurance coverage. If no accredited, licensed IHSA for the pediatric patient exists, this is grounds for not initiating home- or office-based infusions…
- & 4. Use an infusion protocol… with clear directives on recognition of signs/symptoms of reactions and administration of reaction medications and use of EMS or parent transport to an emergency room.
- Maintain accurate documentation and communication of therapy type, dose, and frequency.
- Provide a reliable communication mechanism for the IHSA to notify provider of changes or infusion-related events
- Regularly reviewing ongoing IHSA performance with regard to delivery of services, accurate laboratory ordering and turnaround time, safety and quality concerns and timely redressal of these issues.
- Switch to another IHSA if the performance reliability is unsatisfactory. …we acknowledge that changing IHSAs may be difficult.”
Recommendation 6: A more equitable division of labor should be established to offset increased administrative burden placed on the pediatric gastroenterologist and medical team to effectively facilitate and maintain home- or office-based infusions, especially when driven by payer-mandated policies.
Recommendation 7: …Among patients receiving home- or office-based infusions, unreliable follow-up care with the provider as scheduled is grounds for discontinuation of home- or office-based biologic therapy.
Recommendation 8: A proper appeals process should be in place to prevent cost transference from payer to patient in payer-mandated decisions for home- or office-based infusions.
Our office practice:
- Emergencies: In our office, there is always one physician dedicated to being available to assess patients who are receiving infusions. This helps insure safety and in addition, helps to make sure that minor medical problems do not needlessly postpone important treatment.
- Documentation: With our office-based infusions, each infusion is documented by the administering nurse. This documentation along with labs are embedded in the medical record (EPIC) to help modify treatment.
- Communication: In our office, prior to each infusion, each patient’s chart is reviewed and specific orders are given. This assures that needed blood tests/imaging, additional treatments (eg. iron infusion), insurance authorizations, necessary followup, and personalized adjustments are made. This type of communication needs to be replicated for home-based infusions; hence, the use of home-based infusions could result in a huge increase in uncompensated work for the treating physician.
My take: In my experience, office-based infusions can be provided safely and in a cost-effective manner. While the convenience of home-based infusion is desirable, before implementing broadly, issues regarding communication, safety protocols, and documentation to allow modifications in therapy need to be proactively addressed. Families may not realize some of the complexities involved in managing infusions and how these issues could affect their child’s long-term response to biologic therapy.
Related blog posts:
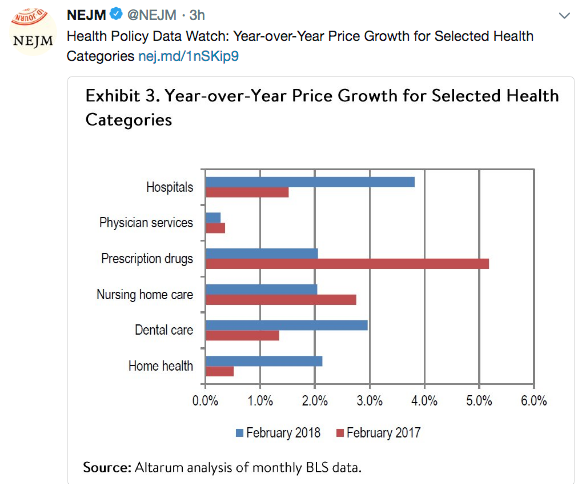
The following image relates to another convenience-related health trend:

Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications/diets (along with potential adverse effects) should be confirmed by prescribing physician/nutritionist. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.













{kind=link}