I am a pediatric gastroenterologist at GI Care for Kids (previously called CCDHC) in Atlanta, Georgia. The goal of my blog is to share some of my reading in my field more broadly. In addition, I wanted to provide my voice to a wide range of topics that often have inaccurate or incomplete information.
Before starting this blog in 2011, I would tear out articles from journals and/or keep notes in a palm pilot. This blog helps provide an updated source of information that is easy to access and search, along with links to useful multimedia sources.
I was born and raised in Chattanooga. After graduating from the University of Virginia, I attended Baylor College of Medicine. I completed residency and fellowship training at the University of Cincinnati at the Children’s Hospital Medical Center. I received funding from the National Institutes of Health for molecular biology research of the gastrointestinal tract.
During my fellowship, I had the opportunity to work with some of the most amazing pediatric gastroenterologists and mentors. Some of these individuals included Mitchell Cohen, William Balistreri, James Heubi, Jorge Bezerra, Colin Rudolph, John Bucuvalas, and Michael Farrell. I am grateful for their teaching and their friendship. During my training with their help, I received a nationwide award for the best research by a GI fellow.
I have authored numerous publications/presentations including original research, case reports, review articles, and textbook chapters on various pediatric gastrointestinal problems. In addition, I have been recognized by Atlanta Magazine as a "Top Doctor" in my field multiple times.
Currently, I am the vice chair of the section of nutrition for the Georgia Chapter of the American Academy of Pediatrics. In addition, I am an adjunct Associate Clinical Professor of Pediatrics at Emory University School of Medicine. Other society memberships have included the North American Society for Pediatric Gastroenterology Hepatology and Nutrition (NASPGHAN), American Academy of Pediatrics, the Food Allergy Network, the American Gastroenterology Association, the American Association for the Study of Liver Diseases, and the Crohn’s and Colitis Foundation.
As part of a national pediatric GI organization called NASPGHAN (and its affiliated website GIKids), I have helped develop educational materials on a wide-range of gastrointestinal and liver diseases which are used across the country. Also, I have been an invited speaker for national campaigns to improve the evaluation and treatment of gastroesophageal reflux disease, celiac disease, eosinophilic esophagitis, hepatitis C, and inflammatory bowel disease (IBD). Some information on these topics has been posted at my work website, www.gicareforkids.com, which has links to multiple other useful resources.
I am fortunate to work at GI Care For Kids. Our group has 17 terrific physicians with a wide range of subspecialization, including liver diseases, feeding disorders, eosinophilic diseases, inflammatory bowel disease, cystic fibrosis, DiGeorge/22q, celiac disease, and motility disorders. Many of our physicians are recognized nationally for their achievements. Our group of physicians have worked closely together for many years. None of the physicians in our group have ever left to join other groups. I have also worked with the same nurse (Bernadette) since I moved to Atlanta in 1997.
For many families, more practical matters about our office include the following:
– 14 office/satellite locations
– physicians who speak Spanish
– cutting edge research
– on-site nutritionists
– on-site psychology support for abdominal pain and feeding disorders
– participation in ImproveCareNow to better the outcomes for children with inflammatory bowel disease
– office endoscopy suite (lower costs and easier scheduling)
– office infusion center (lower costs and easier for families)
– easy access to nursing advice (each physician has at least one nurse)
I am married and have two sons (both adults). I like to read, walk/hike, bike, swim, and play tennis with my free time.
I do not have any financial relationships with pharmaceutical companies or other financial relationships to disclose. I have helped enroll patients in industry-sponsored research studies.
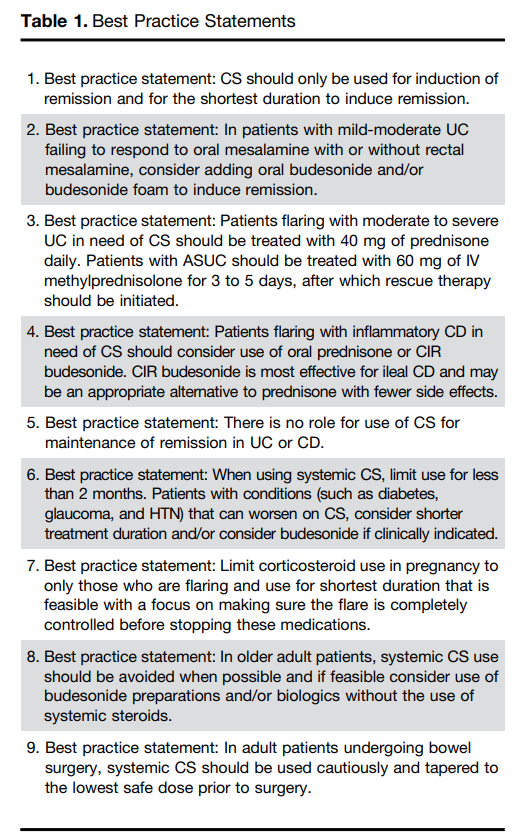
Steroids are commonly used and misused for inflammatory bowel disease. This article reviews best practices, steroid formulations/dosing, and potential complications.
For moderate to severe ulcerative colitis (in adults), the authors recommend treatment with 40 mg of prednisone daily. Patients with ASUC (acute severe ulcerative colitis) should be treated with 60 mg of IV methylprednisolone for 3 to 5 days, after which rescue therapy should be initiated
Use of budesonide is recommended as an option for many clinical situations to minimize steroid adverse effects. These situations include mild-moderate UC failing to respond to mesalamine, ileal CD and older patients
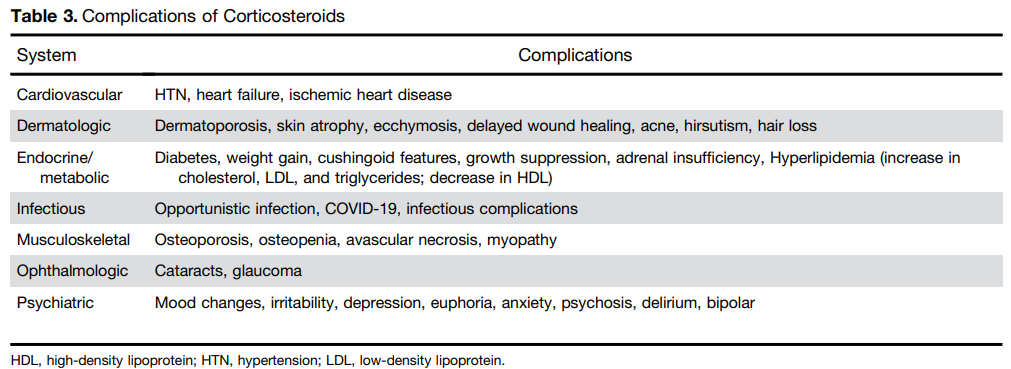
Postoperative complications: “In the postoperative period, patients treated with CS had a higher risk of both infectious complications (aOR, 3.69; 95% CI, 1.24–10.97) and major infectious complications (aOR, 5.54; 95% CI, 1.12–27.26) [Abrerra et al].135 Subramanian pooled data from 7 studies showing that preoperative CS use is associated with increased postoperative complications (OR, 1.41; 95% CI, 1.07–1.87) as well as infectious complications.
The authors note that corticosteroids “remain widely available and are an effective short-term option for induction of remission in patients with active UC or inflammatory CD. However, their well-described and significant safety profile warrants proactive strategies to limit their use through non-systemic formulations, short-term exposures, steroid-sparing maintenance options, and most recently, complete steroid avoidance strategies.”
My take: Continuing steroids when they are not effective prior to potential surgery (eg. ASUC) remains a frequent problem. Sometimes, it is difficult to know it they are helping some.
“This 3-paper Series reviews the evidence about the increase in ultra-processed foods in diets globally and highlights the association with many non-communicable diseases. This rise in ultra-processed foods is driven by powerful global corporations who employ sophisticated political tactics to protect and maximize profits. Education and relying on behavior change by individuals is insufficient. Deteriorating diets are an urgent public health threat that requires coordinated policies and advocacy to regulate and reduce ultra-processed foods and improve access to fresh and minimally processed foods. The Series provides a different vision for the food system with emphasis on local food producers, preserving cultural foods transitions and economic benefits for communities.”
In one of the papers, led by Dr. Monteiro, the authors identified 104 studies linking ultraprocessed foods to health conditions, including Type 2 diabetes, obesity, heart disease, kidney disease and Crohn’s disease…
The authors suggested that governments adopt policies, like taxes on sugary drinks and warning labels for certain ultraprocessed foods, especially those high in sugar, fat or salt. They also recommended restrictions on marketing ultraprocessed foods to children and reducing their use in school meals. The proposed policies are similar to those that have worked to reduce smoking rates…
Robert F. Kennedy Jr., the nation’s health secretary, and his “Make America Healthy Again” movement have drawn attention to the links between poor health and ultraprocessed foods. But so far, Mr. Kennedy has focused on reducing the use of artificial colors and certain food additives, efforts that Dr. Popkin said would do little to improve the healthfulness of the food supply. And this year, the Trump administration cut SNAP benefits and programs that funded schools and food banks to purchase foods from local farms.”
M Hook et al. JPGN 2025; DOI: 10.1002/jpn3.70221. Esophageal coin with moth eaten appearance: A cause for caution
This case report describes a penny ingestion by a 10 yo with autism that likely happened nine months before attempted retrieval. The coin was not able to be retrieved due to stricturing but was advanced into the stomach (the authors note advancement into duodenum would be better); in addition, there was an esophageal diverticulum that was identified likely secondary to the caustic damage.
In the discussion, the authors note that “the ‘moth eaten’ appearance is a rare finding that indicates prolonged foreign body retention and unforeseen mucosal injury…It is specific to post-1982 pennies, composed of 97.5% zinc.4 Hydrochloric acid exposure dissolves zinc, forming caustic zinc chloride.”
My take: Future generations will not see this radiologic finding. For now, if this finding is seen, it likely indicates a more difficult foreign body removal.
For those trying to understand the success of the current HBV immunization strategy and why altering the timing of HBV vaccinations is a bad idea, this is a worthwhile article.
Key points:
“To date, more than 1 billion doses of HepB vaccines have been administered worldwide, and they are considered one of the safest and most effective vaccine ever made.1,2,6“
“Because of the high risk for chronic HBV infection, the CDC/Advisory Committee on Immunization Practices (ACIP), WHO, and health ministries of many countries recommend universal HBV vaccination of all infants beginning with a “birth dose” for newborns, preferably within the first 24 hours of birth, followed by completion of the 3-dose infant vaccination schedule…Implementation of routine infant and childhood vaccination, including birth dose HBV vaccine, prevented an estimated 210 million infections globally between 1980 and 2015.4“
“In 1991, with evidence showing substantial number of infants and others at risk were missed by a risk-based approach to HepB vaccination, the ACIP recommended universal HepB vaccination for all infants, with the first dose administered before hospital discharge along with hepatitis B immune globulin (HBIG) for infants born to mothers who tested positive for HBsAg or whose HBsAg status was unknown.5,6,14“
“In 2018, the CDC/ACIP recommendation specified that the birth dose of HepB vaccine should be administered within 24 hours of birth including for preterm infants, regardless of maternal HBsAg status.14 …Timely birth dose HepB vaccination regardless of maternal HBsAg status serves as a safety net for perinatal transmission from HBsAg-positive mothers missed by HBsAg screening programs and protects against the small but non-zero risk of HBV infections from household and other exposures for infants born to HBsAg-negative mothers.”
“HepB vaccination alone prevents 75% to 80% of perinatal HBV transmission.2 The addition of maternal HBsAg screening and further testing for hepatitis B e antigen or HBV DNA if HBsAg test is positive allows for additional interventions to eliminate mother-to-child transmission of HBV.”
US CDC recommendations for HBV vaccination. Decline in reported number of acute HBV infections in the United States in association with CDC recommendations for HBV vaccination, 1980–2022.
My take (borrowed in part from authors): It would be a big mistake to resume the risk-based approach to newborn HepB vaccination. “HepB vaccine is a safe and highly effective vaccine. HepB vaccination prevents an incurable chronic infection and related morbidity and mortality from cirrhosis and HCC. Indeed, HepB vaccine is the first cancer-prevention vaccine…Universal HepB birth dose vaccination regardless of maternal HBsAg status is the most effective as well as the most cost-effective strategy in eliminating HBV infection. Newborns and infants are those at highest risk of chronic HBV infection. Delaying the first dose of HepB vaccine even by a few days exposes the infants to increased risk of developing lifelong infection,18 chronic liver disease, and premature death.”
“Delaying the first vaccine in the series to one-month, four years, or 12 years of age will undermine the vaccine’s effectiveness, and relying on just screening pregnant women for hepatitis B is insufficient.
Although some of the changes that have been discussed by ACIP sound small, they are not grounded in new evidence and would undo more than three decades of a prevention strategy that has nearly eliminated early childhood hepatitis B in the United States.“
The review of pediatric MASLD addresses epidemiology, pathophysiology, natural history, screening, diagnosis, treatment, comorbidity management, outcome monitoring, and transition of care. It also discusses the implications of the 2023 nomenclature revision, which emphasizes evaluating both hepatic steatosis and cardiometabolic risk factors.
Some key points:
Box 1 outlines numerous (32) research priorities, including the need for prospective longitudinal cohort studies.
“Globally, the estimated prevalence of MASLD in children is 7.6%, making it the most common cause of chronic liver disease in children”
Figure 4 describes the interplay between risk factors for MASLD included genetic predisposition, prenatal factors and environmental exposures
Figure 5 summarizes comorbid conditions which include obstructive sleep apnea, prediabetes/diabetes, cardiovascular disease (dyslipidemia, hypertension, left ventricular hypertrophy), anxiety/depression, reduced bone mineral density, renal dysfunction and polycystic ovarian syndrome. Table 6 summarizes evaluation and initial management with most of these conditions. Yearly screening for diabetes in children with MASLD is recommended.
ALT remains most common screening test with >26 U/L for adolescent males and >22 U/L for adolescent females having optimal sensitivity (>80-85%). We recommend “screen for MASLD in children aged 10 years or older with overweight and cardiometabolic risk factors or family history or obesity.” Annual screening recommended if at risk.
Table 2 provides a long list of medications which may promote weight gain. These include antihistamines, steroids, some contraceptives, anticonvulsants, antidepressants, antipsychotics, methotrexate, and doxycycline
Diagnostic evaluation:
Diagnosis of MASLD requires confirmation of steatosis (by imaging or biopsy) in addition to the presence of at least one cardiometabolic risk factor. ALT elevation with a cardiometabolic risk factor is insufficient.
“Consider liver biopsy in cases where there is uncertainty, especially if ALT levels are persistently elevated (>2 times the ULN)”
Table 3 lists inborn errors of metabolism and monogenetic diseases which may cause childhood-onset steatotic liver disease. Evaluation of inborn errors of metabolism should be considered if atypical signs or symptoms, such as early onset (<3 yrs), rapidly progressive, absence of obesity, or other organ involvement (especially neurological)
Table 4 summarizes imaging modalities to assess steatosis and fibrosis in children. Only MRI-PDFF has been validated in children (for steatosis)
Table 5 describes BMI classification in children (WHO and AAP)
Lifestyle treatments are detailed including diet (reduction of added sugars, Mediterranean diets) and exercise
Emerging medications are reviewed. However, practice statement notes “No pharmacotherapies are currently recommended or approved as specific treatments for MASLD or MASH in children…Medications approved for use in children ages 12 years and older to treat obesity or type 2 diabetes may be considered for children with MASLD.”
My take: This is a comprehensive practice guidance. It emphasizes an extensive diagnostic evaluation. The threshold for liver biopsy is relatively low in this guidance. As more data emerges, it is likely that more emphasis will be placed on the use of pharmacotherapies.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
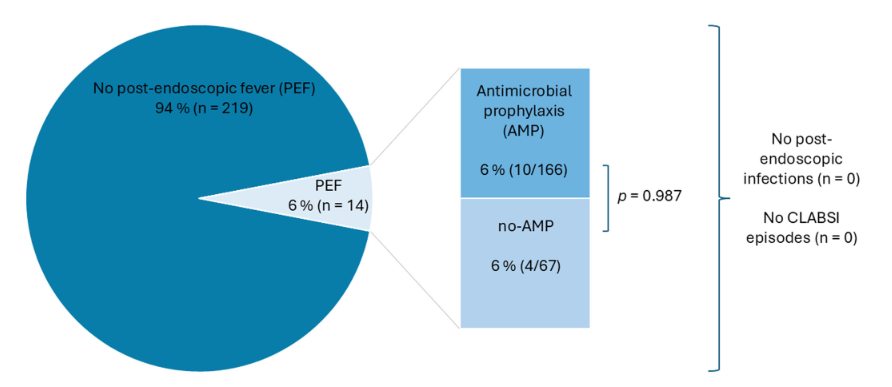
Methods: This was a retrospective single-center observational study which included children with IF and CVC who underwent GI endoscopy between 2019 and 2024. Intravenous antibiotic prophylaxis was used in 71.2% of the procedures.
Key findings:
The overall post-endoscopic fever (PEF) rate was 6%, with no significant difference between the group that received prophylactic antibiotics and the group that did not. Specifically, there were 10 with PEF that had received prophylactic antibiotics and 4 that had PEF with no prophylaxis
No infections, including central line-associated bloodstream infections, were observed
5/14 of the cases with PEF had an interventional procedure. The remainder had a diagnostic EGD, colonoscopy or both.
Interventional Cases:
Discussion Points:
“PEF in children with IF was 6%, which is approximately 10 times higher than the recently published 0.55% in pediatric patients following endoscopic procedures by Boster et al.” (see: Must-Read: How to Handle Post-Procedure Fevers)
A strength of this study was that the comparison of children with IV antibiotics versus those without was due to an institutional policy change in 2022. This helps eliminate selection bias in the determination that IV antibiotics were not beneficial in preventing PEF
My take: The high rate (6%) of PEF should be discussed with families prior to endoscopic procedures. The rate was increased (36%) in those with interventional procedures. It is reassuring that no definitive infections were identified despite the fevers.
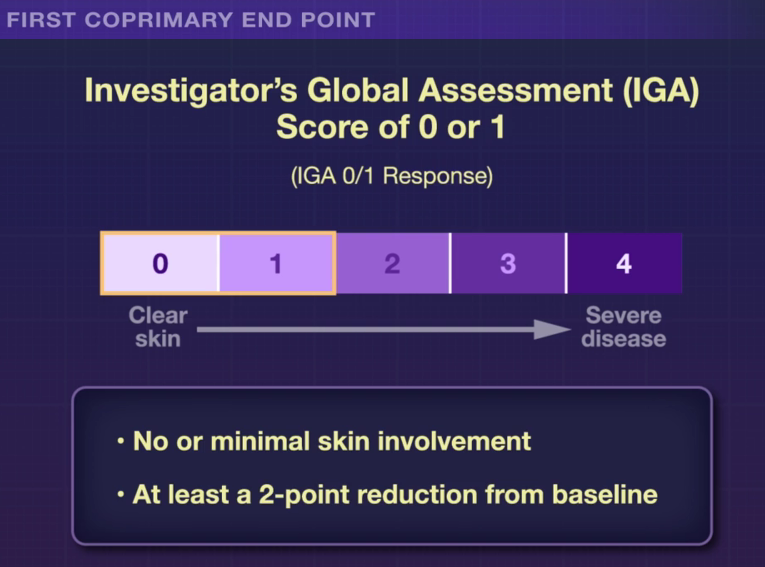
R Bissonnette et al. NEJM 2025; 393: 1784-1795. Oral Icotrokinra for Plaque Psoriasis
RS Stern. NEJM 2025; 303: 1854-1855. Oral Psoriasis Therapy — For Whom and at What Cost and Risk?
S Wharton et al. NEJM 2025; 303: 1796-1806. Orforglipron, an Oral Small-Molecule GLP-1 Receptor Agonist for Obesity Treatment
In the ICONIC-LEAD study (Bissonnette et al), 684 adolescents and adults participated in a DBPC trial with an oral peptide, icotrokinra, which binds the IL-23 receptor. This medication is of interest as there are ongoing trials with it for inflammatory bowel disease. Other injectable medications targeting IL-23 are already approved for IBD.
Key Findings:
The associated editorial notes that this new therapy is likely to cost ~$70,000 per year. The cost of psoriasis care has increased more than 2000% since 1997. “Because of these high prices, rebates and discounts to pharmacy benefit managers that often guide formulary preferences are likely to govern clinician’s selection of immune-based oral and parenteral therapies for psoriasis.”
In the ATTAIN-1 Trial (Wharton et al), the authors share the results of an oral GLP-1 Receptor Agonist, Orforglipron, monotherapy for obesity.
My take: There are similar injectable alternatives to each of these medications for psoriasis, obesity and diabetes. The availability of oral medications could reduce one barrier to treatment. Cost barriers may preclude their use in many patients when they become available. In addition, long-term outcome data are still needed.
This article reviews the growing health concerns regarding microplastics and nanoplastics (MNPs) specifically regarding the GI tract.
Key points:
“As these [plastic] products degrade, they break down into smaller particles, forming microplastics (< 5 microm) and nanoplastics (<1 microm), collectively referred to as MNPs”
“Although many plastic products are deemed recyclable, in the United States, less than 10% are actually recycled…annual global production projected to reach 1.1 billion tons by 2025. Simultaneously, over 12 billion tons of plastic wastes are expected to accumulate in landfills”
“The average American ingests approximately 5g of plastic per week, equivalent to 1 credit card, and 39,000–50,000 particles annually”
Potential association of MNPs with metabolic-associated steatotic liver disease, liver and pancreatic cancer and inflammatory bowel disease. “Studies have reported significantly higher levels of MNPs in patients with IBD compared with healthy controls.”
In a related article in Gastroenterology and Endoscopy News (October 2025), Dr. Johnson noted that “reduction of plastic intake from bottled water to tap water in one study reduced microplastic intake, the number of particles within human tissues, from 90,000 to 4,000…Avoid heating food in plastics…the effect of microwave increased the evidence of microplastics by over 4.2 million and the nanoplastics, 2 billion, just in three minutes in the microwave.”
My take: Something that almost everyone could agree on – they would like less plastic in their food and environment. How to achieve this is much more difficult.
JM Perrin, TL Cheng. NEJM 2025; 393: 1869-1872. “Truly Prioritizing Child Health — The Missed Opportunities of the MAHA Commission”
This commentary welcomes the attention to child health which was a focus of the MAHA commission. This review provides perspectives on the stated policy aims and on what else is needed.
An excerpt:
The [MAHA] commission has highlighted four specific areas of concern: poor diet, environmental chemicals, lack of physical activity and chronic stress, and overmedicalization. The strategy outlined in the MAHA Commission’s recent report, however, misses real opportunities to address the chronic disease epidemic and “whole-person health”…
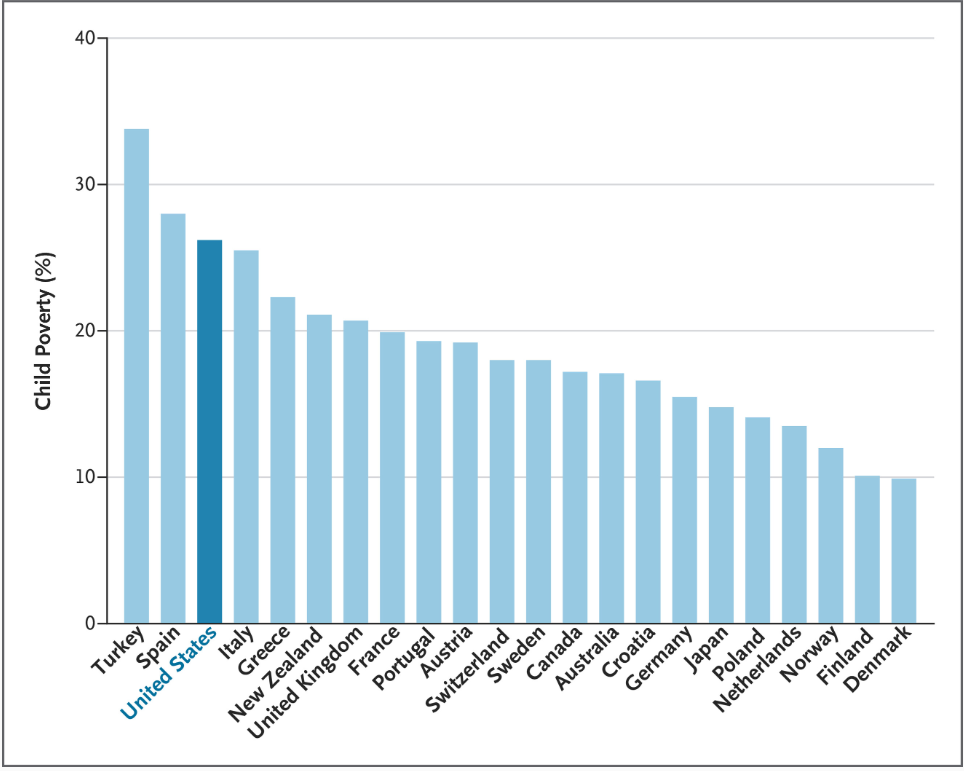
The MAHA Commission’s view of the state of U.S. child health ignores leading contributors to rising childhood morbidity and mortality: firearm injuries (the leading cause of death among U.S. children), drug overdoses, and motor vehicle injuries. Most striking is the commission report’s silence regarding the association of poverty with poor child health… which contributes to higher rates of asthma, obesity, and mental health conditions...
The first MAHA priority, children’s diets, has long been a concern of the U.S. child health community, particularly the intake of sugar-sweetened beverages, excessive portion sizes, and food additives. But pediatricians and researchers also know that food insecurity, food-industry marketing practices, and limited access to healthy foods are prime drivers of childhood obesity rates. Nutritious meals require money…
The MAHA strategy recommends marginal changes to the diets of U.S. children, such as reducing the use of food dyes and reducing consumption of ultraprocessed foods, even as the government is increasingly limiting public food assistance.
The commission’s focus on environmental chemicals is appropriate, given that exposures to potentially toxic chemicals in foods, household supplies, cleaning agents, farm supplies, and elsewhere have grown dramatically. The MAHA strategy provides little relief, however: a few research projects and no regulatory change…The MAHA report stops short of recommending the research and regulatory reform necessary for identifying, restricting, and mitigating harmful exposures.
Concerns about physical activity and stress are also justified. Many studies have documented alarming declines in physical activity, examined the causes and effects, and found associations with mental health and well-being… Strengthening early-childhood, school-based, and community-based physical activity programs, as well as social media strategies for promoting lifestyle changes, could improve health and reduce stress among young people, but the MAHA Commission mainly orders schools and communities to increase physical activity.
Finally, the commission has raised concerns about medications, especially stimulants and psychotropic agents…In response, the MAHA Commission primarily proposes studying prescribing patterns and “solutions that can be scaled up to improve mental health.” It does not address more fundamental ways of changing medication use…
Despite its attention to children’s health, the MAHA Commission’s lengthy list of aspirations and recommended changes is unlikely to make a real impact. Instead, next steps should include implementing policies, programs, and research supported by the strong evidence base that clinicians and investigators have built painstakingly for many years.
My take: The policies pursued by the current administration like limiting food dyes do not target the big drivers of poor health outcomes in children.
The authors of this commentary also “chaired the National Academies of Sciences, Engineering, and Medicine (NASEM) study described in “Launching Lifelong Health by Improving Health Care for Children, Youth, and Families”1 [which] provides clear, evidence-based lessons that could help in achieving MAHA objectives.”
Childhood Poverty Rates: Shown is the percentage of children in households with incomes below 60% of the median national income. Data are from UNICEF and reflect averages from 2019 through 2021.
It is well-recognized that patients with prior intestinal malrotation have frequent GI symptoms after repair. This retrospective study with 354 children (using TriNetX EMR database) quantitates these problems compared to a control group.
Key findings:
Symptoms were less severe at years 3-5 post-index for IM group: constipation 29.4%, Abdominal pain 16.4%, Nausea/Vomiting 21.2%, Diarrhea 9.6%, and GERD 22.3%.
My take: While database studies have numerous limitations, it is clear that having a history of intestinal malrotation poses a significant risk of persistent GI symptoms after repair. It will be worthwhile for families to be informed of this at the time of IM repair.