I am a pediatric gastroenterologist at GI Care for Kids (previously called CCDHC) in Atlanta, Georgia. The goal of my blog is to share some of my reading in my field more broadly. In addition, I wanted to provide my voice to a wide range of topics that often have inaccurate or incomplete information.
Before starting this blog in 2011, I would tear out articles from journals and/or keep notes in a palm pilot. This blog helps provide an updated source of information that is easy to access and search, along with links to useful multimedia sources.
I was born and raised in Chattanooga. After graduating from the University of Virginia, I attended Baylor College of Medicine. I completed residency and fellowship training at the University of Cincinnati at the Children’s Hospital Medical Center. I received funding from the National Institutes of Health for molecular biology research of the gastrointestinal tract.
During my fellowship, I had the opportunity to work with some of the most amazing pediatric gastroenterologists and mentors. Some of these individuals included Mitchell Cohen, William Balistreri, James Heubi, Jorge Bezerra, Colin Rudolph, John Bucuvalas, and Michael Farrell. I am grateful for their teaching and their friendship. During my training with their help, I received a nationwide award for the best research by a GI fellow.
I have authored numerous publications/presentations including original research, case reports, review articles, and textbook chapters on various pediatric gastrointestinal problems. In addition, I have been recognized by Atlanta Magazine as a "Top Doctor" in my field multiple times.
Currently, I am the vice chair of the section of nutrition for the Georgia Chapter of the American Academy of Pediatrics. In addition, I am an adjunct Associate Clinical Professor of Pediatrics at Emory University School of Medicine. Other society memberships have included the North American Society for Pediatric Gastroenterology Hepatology and Nutrition (NASPGHAN), American Academy of Pediatrics, the Food Allergy Network, the American Gastroenterology Association, the American Association for the Study of Liver Diseases, and the Crohn’s and Colitis Foundation.
As part of a national pediatric GI organization called NASPGHAN (and its affiliated website GIKids), I have helped develop educational materials on a wide-range of gastrointestinal and liver diseases which are used across the country. Also, I have been an invited speaker for national campaigns to improve the evaluation and treatment of gastroesophageal reflux disease, celiac disease, eosinophilic esophagitis, hepatitis C, and inflammatory bowel disease (IBD). Some information on these topics has been posted at my work website, www.gicareforkids.com, which has links to multiple other useful resources.
I am fortunate to work at GI Care For Kids. Our group has 17 terrific physicians with a wide range of subspecialization, including liver diseases, feeding disorders, eosinophilic diseases, inflammatory bowel disease, cystic fibrosis, DiGeorge/22q, celiac disease, and motility disorders. Many of our physicians are recognized nationally for their achievements. Our group of physicians have worked closely together for many years. None of the physicians in our group have ever left to join other groups. I have also worked with the same nurse (Bernadette) since I moved to Atlanta in 1997.
For many families, more practical matters about our office include the following:
– 14 office/satellite locations
– physicians who speak Spanish
– cutting edge research
– on-site nutritionists
– on-site psychology support for abdominal pain and feeding disorders
– participation in ImproveCareNow to better the outcomes for children with inflammatory bowel disease
– office endoscopy suite (lower costs and easier scheduling)
– office infusion center (lower costs and easier for families)
– easy access to nursing advice (each physician has at least one nurse)
I am married and have two sons (both adults). I like to read, walk/hike, bike, swim, and play tennis with my free time.
I do not have any financial relationships with pharmaceutical companies or other financial relationships to disclose. I have helped enroll patients in industry-sponsored research studies.
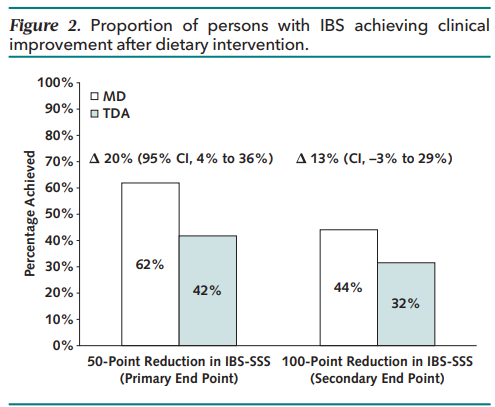
Methods: Randomized noninferiority clinical trial (n=139 Adults from UK) — 6 weeks of the MD (Mediterranean diet) (n = 68) versus TDA (traditional diet advice) (n = 71). Primary end point was the proportion achieving clinical response, defined as 50-point or greater reduction in IBS Symptom Severity Scale (IBS-SSS).
Traditional dietary advice’s main elements are to “adopt sensible eating habits and avoid excess fatty foods, spicy foods, processed foods, caffeine, fizzy drinks, and alcohol. The principal components of the MD are a diet rich in fruit, vegetables, pulses (aka legumes), whole grains, nuts, fish, and olive oil.”
Key findings:
The primary end point was met by 62% following a MD versus 42% following TDA (P = 0.017)
There was a greater reduction in the mean IBS-SSS after a MD than TDA (−101.2 vs. −64.5)
My take: I agree with the authors: The Mediterranean diet “represents a viable first-line dietary intervention for IBS.”
Methods: In this systematic review and meta-analysis, the authors identified “4595 articles, of which 59 randomised controlled trials were included, representing 7045 participants with functional constipation. Interventions included polyethylene glycol (n=36 studies), lactulose (n=18), magnesium oxide or magnesium hydroxide (n=7), picosulfate (n=1), liquid paraffin (n=4), prucalopride (n=1), lubiprostone (n=2), linaclotide (n=3), plecanatide (n=1), enemas (n=2), and domperidone (n=1).”
Key findings:
Meta-analyses for treatment success showed that polyethylene glycol was probably more effective than placebo (RR 1·74, moderate certainty of evidence) and may be more effective than lactulose (1·35], low certainty of evidence)
Linaclotide probably leads to higher defecation frequency than placebo
Prucalopride is probably not more effective than placebo
“Most other therapies provided evidence that was of very low certainty, due to methodological limitations and insufficient information to assess the risk of bias, precluding any evidence-based conclusions”
The discussion reviews the problems with trial design, problems with underpowered studies, and “pervasive issues with heterogeneity. The use of concomitant therapeutics or permitted interventions and the disease severity of the patient populations varied greatly from study to study.”
My take: This study outlines what is needed to improve future research for pediatric constipation. For now, there is little certainty regarding the effectiveness of most constipation medications.
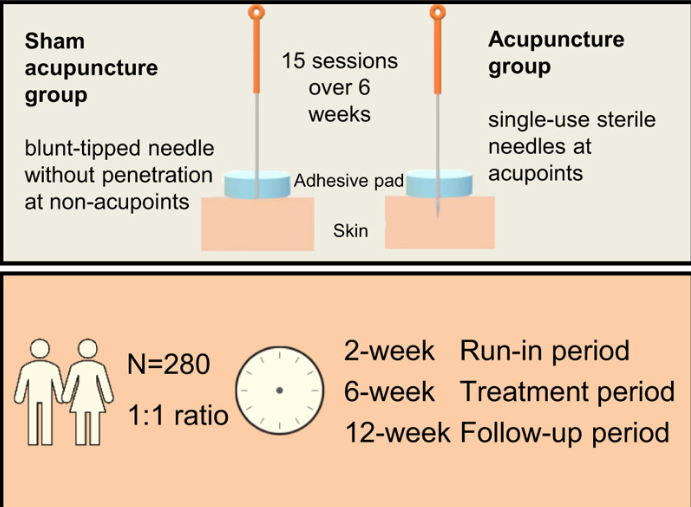
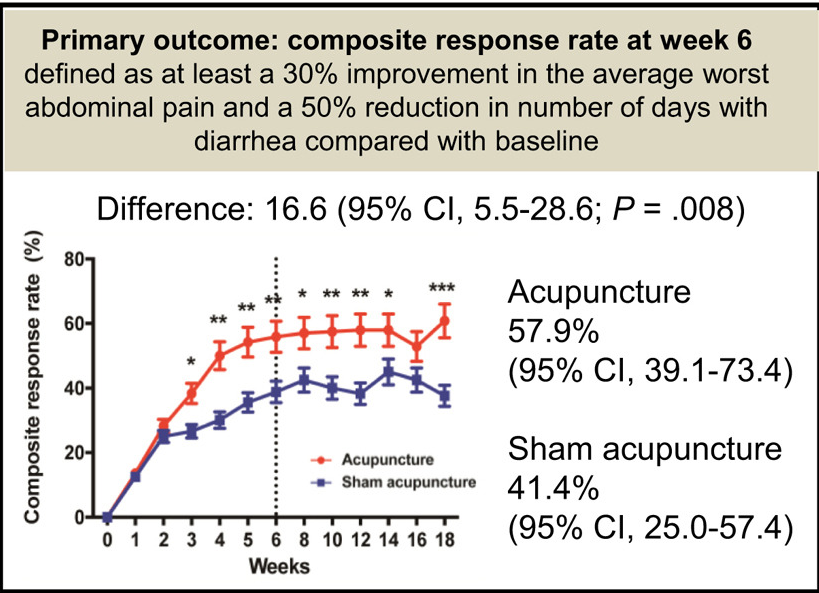
This ACTION study enrolled 280 patients (18-75 yrs) with IBS-D in a multicenter randomized controlled trial in 6 hospitals in China. “For the sham acupuncture group, blunt-tipped placebo needles with a similar appearance to real needles were used over the adhesive pads with no skin penetration. Five fixed pairs of non-acupoints (10 stimulation points in total) away from meridians or conventional acupoints were used.”
Key finding:
The primary outcome (see below) was reached by 71 (57.9%) patients in the acupuncture group compared with 47 (41.4%) patients in the sham acupuncture group (risk ratio 1.40; P = .008)
The effects of acupuncture in symptomatic improvements of IBS-D persisted 3 months after treatment with minimal to no side effects
Limitations including the difficulty of acupuncture blinding (despite the identical treatment setups)
My take: Acupuncture, especially given its safety, is a reasonable therapy for IBS-D; though, it is not recommended in recent pediatric guidelines. “The rub” in many locations is finding qualified practitioners.
Acupuncture for irritable bowel syndrome (2012). In this study, true acupuncture was not shown to be more effective than sham acupuncture; however, there was a high placebo response with sham acupuncture
Dr. B Li, emeritus professor of Pediatrics (Medical College of Wisconsin), gave this year’s Billy Meyers Lecture. Dr. Li is considered the world’s foremost authority on cyclic vomiting syndrome (CVS) (‘the emperor of emesis’). He gave a fantastic update. I have taken some notes and shared many of his slides. There may be inadvertent omissions and mistakes in my notes. More information on the CVS 2025 guidelines is noted in a separate post: 2025 Pediatric Cyclic Vomiting Syndrome Guidelines
Historical background of CVS: Early descriptions of CVS date back to 1880s and Samuel Gee (who also is credited with the first modern description of celiac disease). Charles Darwin was likely affected by CVS
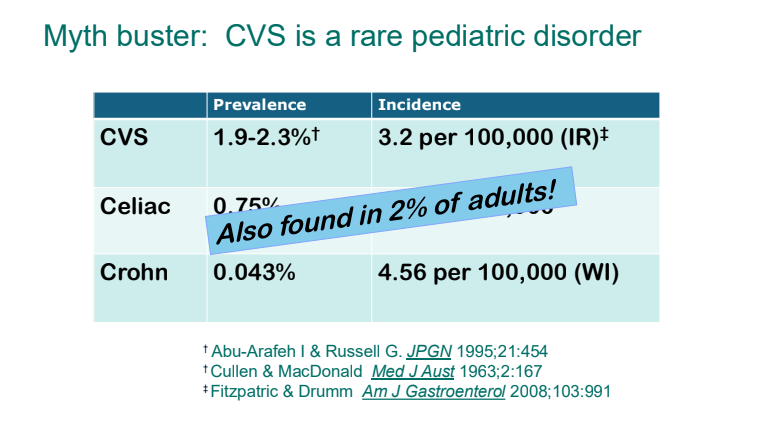
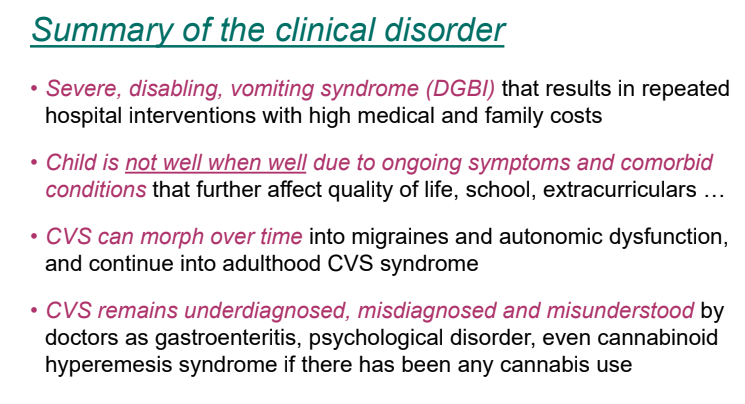
Epidemiology: CVS is nota rare disorder. It likely affects ~2% of kids and adults
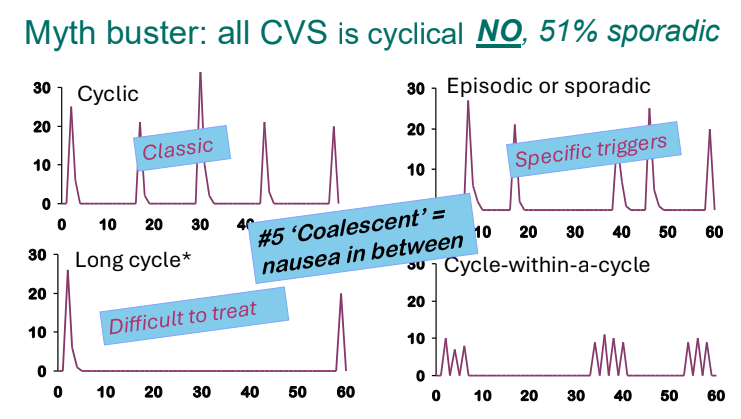
There are several patterns of CVS. Many patients who have CVS do not have a cyclical pattern
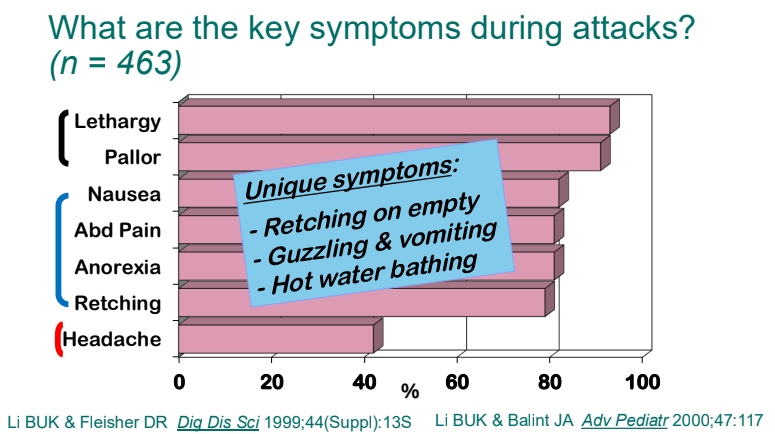
Lethargy and pallor are common symptoms which make patients appear more ill
Retching on an empty stomach and severe emesis are hallmarks and likely indicate that the primary mechanism is not due to the GI tract. Though there are some food poisonings (eg. Bacillus cereus) that can have some of these symptoms but typically milder in severity
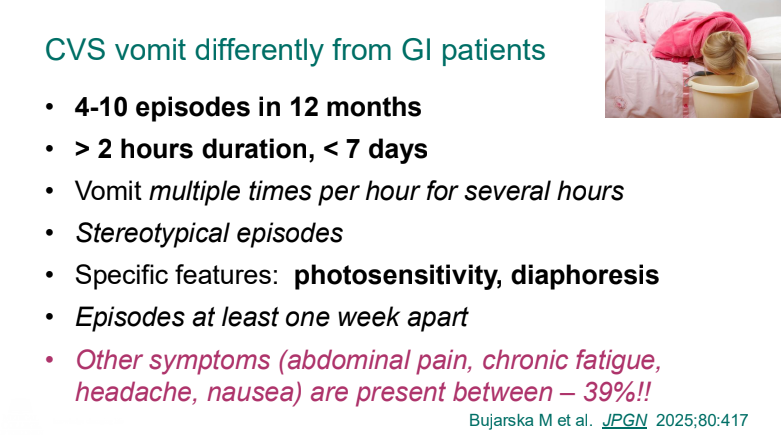
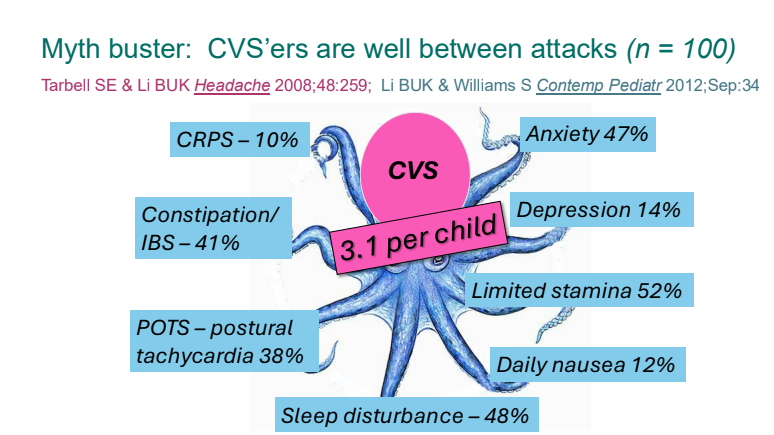
Previously, CVS patients were thought to be well in between episodes. However, ~40% have inter-episode symptoms
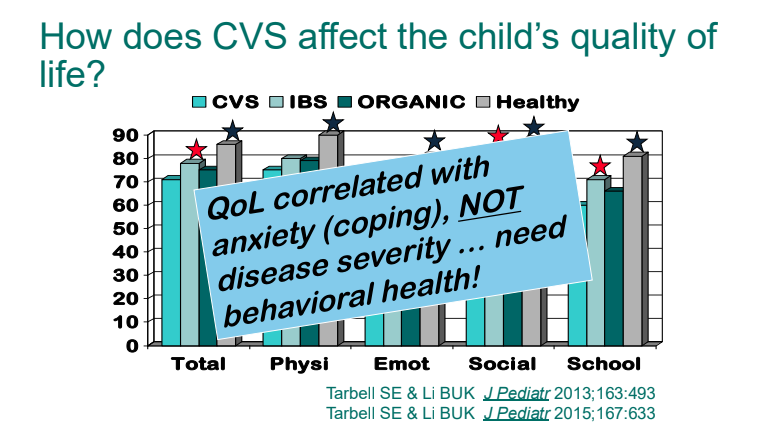
Quality of life is correlated mainly with anxiety/coping rather than the severity of episodes
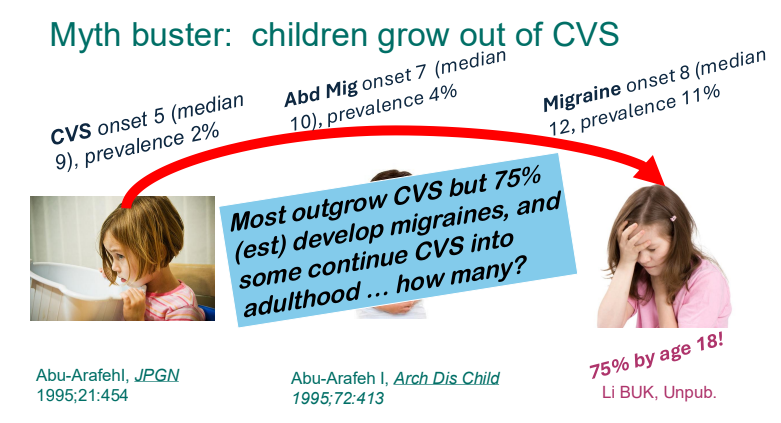
Children with CVS often (~75%) develop migraines by adulthood
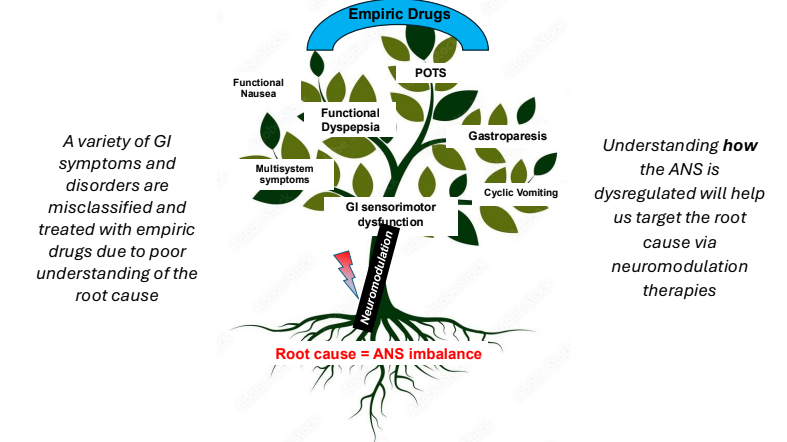
Underlying pathophysiology likely involves the autonomic nervous system
2025 CVS Guidelines — took about 3 years to develop. It is noted that the 2008 guideline diagnostic criteria missed about 48% of cases (Bujarska et al. JPGN 2025; 80: 417)
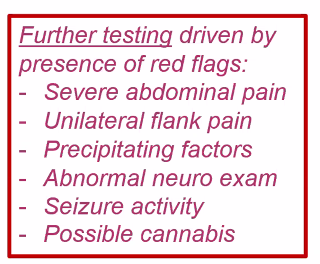
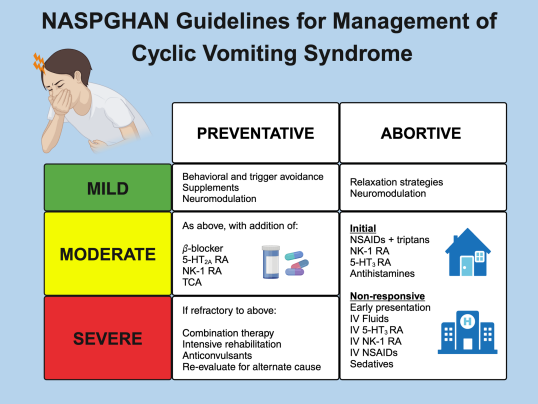
2025 Guidelines emphasize limited diagnostic workup at presentation (eg. UGI and basic labs) unless there are alarm symptoms. Alarm symptoms include the following:
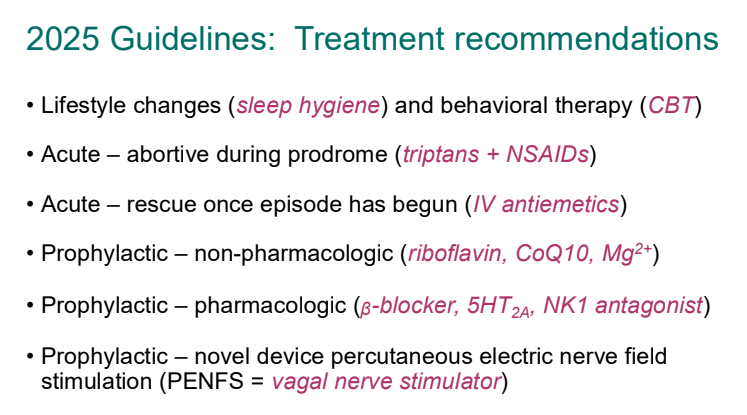
For abortive therapy, the new guidelines favor aprepitant over ondansetron, and generally favor D5 over D10 IVFs.
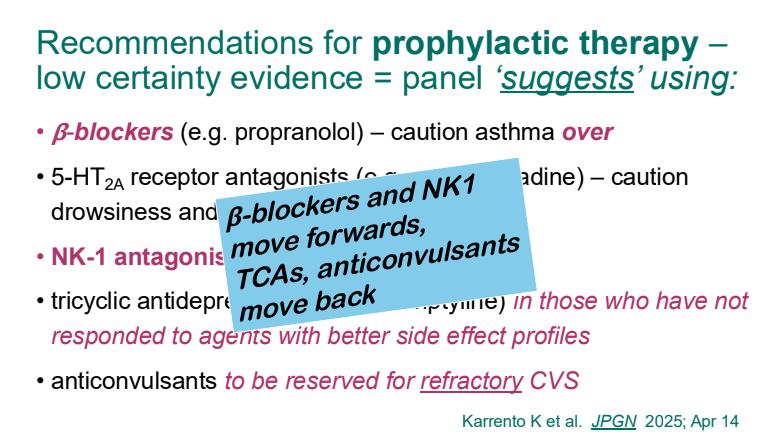
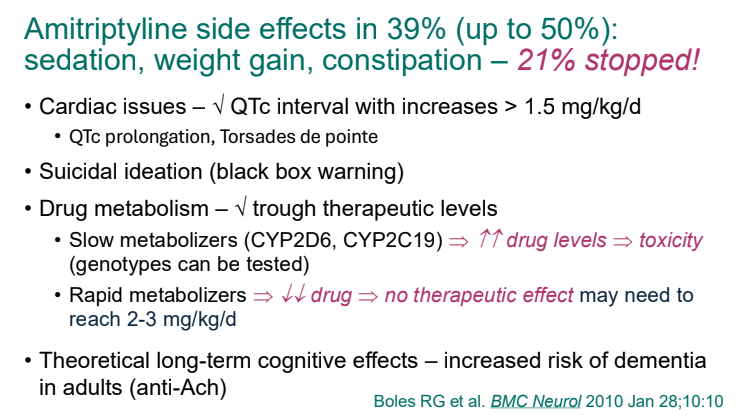
For prophylactic therapy, there is now an emphasis on non-pharmacologic therapy in addition to pharmacologic agents and PENFS. Propranolol and aprepitant are favored prior to use of TCA agents like amitriptyline due to side effect profile
Action plan for ED may help speed care and lower likelihood of admission
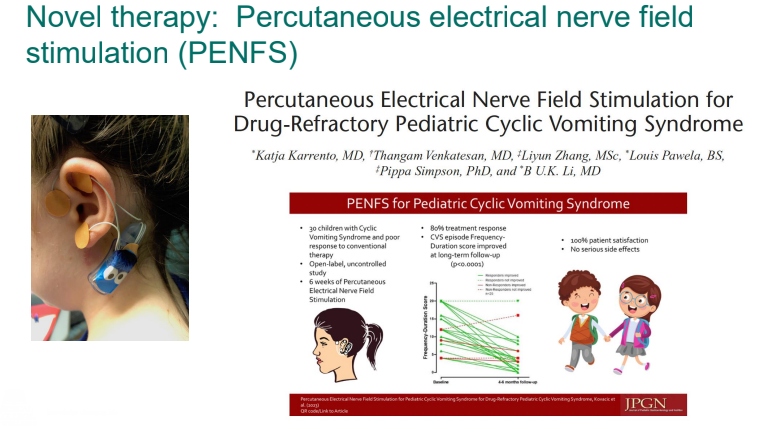
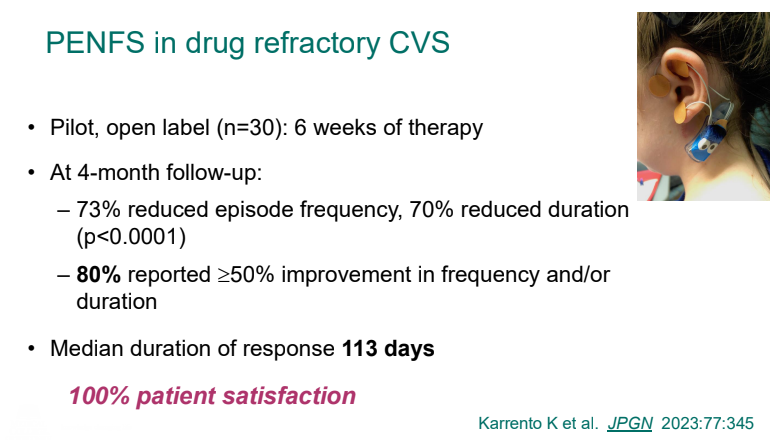
PENFS for prophylactic therapy had a durable response (113 days) in a recent study
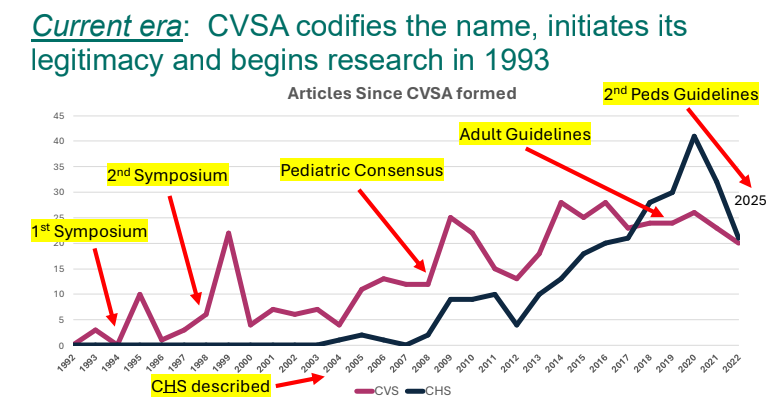
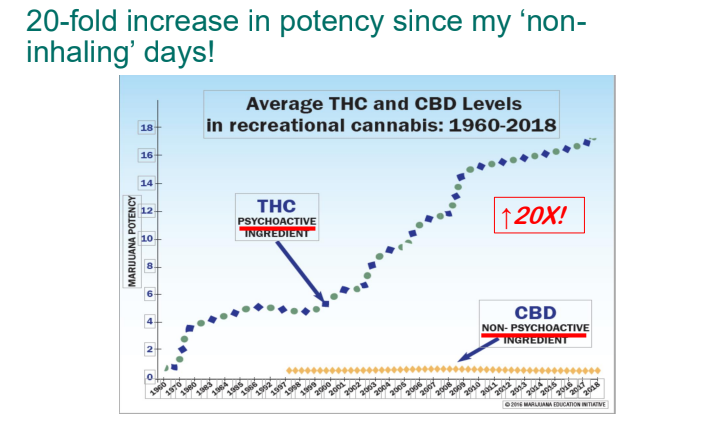
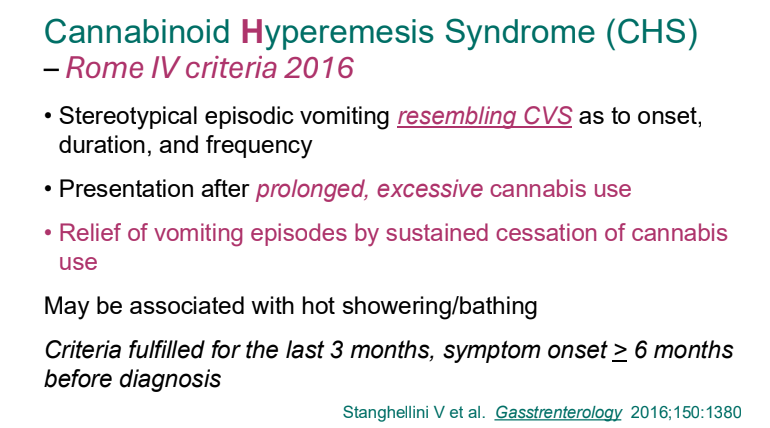
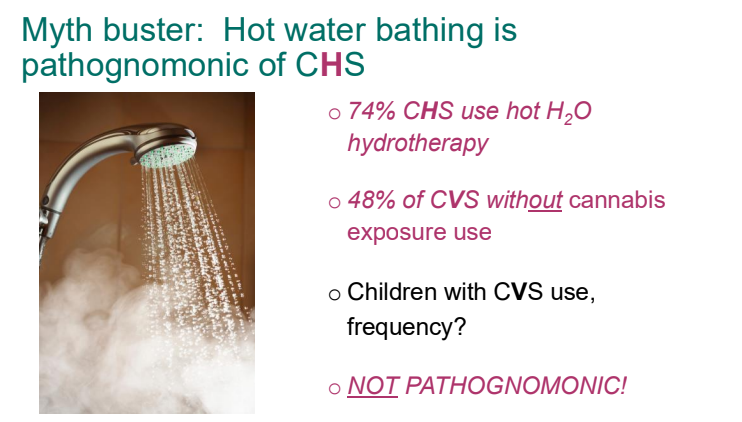
Cannaboid hyperemesis syndrome (CHS) was first described in 2004 and has been rapidly increasing related to increased use and potency of THC products. Haloperidol, topical capsaicin and hot water (prolonged) bathing are often effective
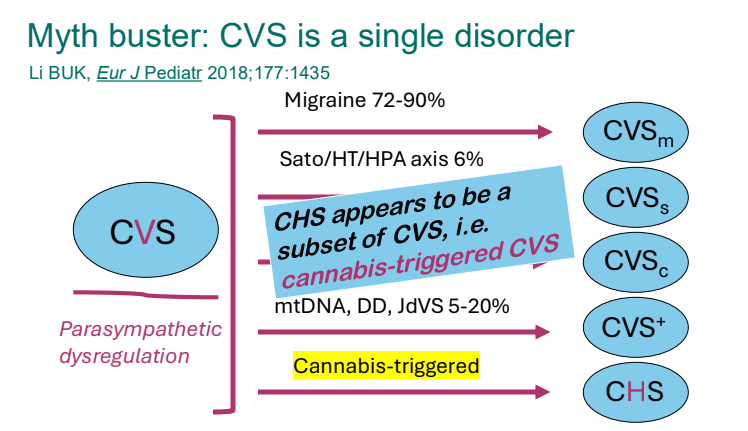
Variants include the CVS associated with mitochondrial dysfunction, the Sato variant associated with increased BP, increase ACTH/cortisol, Catmaenial CVS is related to menses, and CHS (CVS-like) associated with cannabis use
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition
A Phillip et al. J Pediatr Gastroenterol Nutr. 2025;81:913–921. A narrative review of the ileal pouch in pediatric inflammatory bowel disease and familial adenomatous polyposis
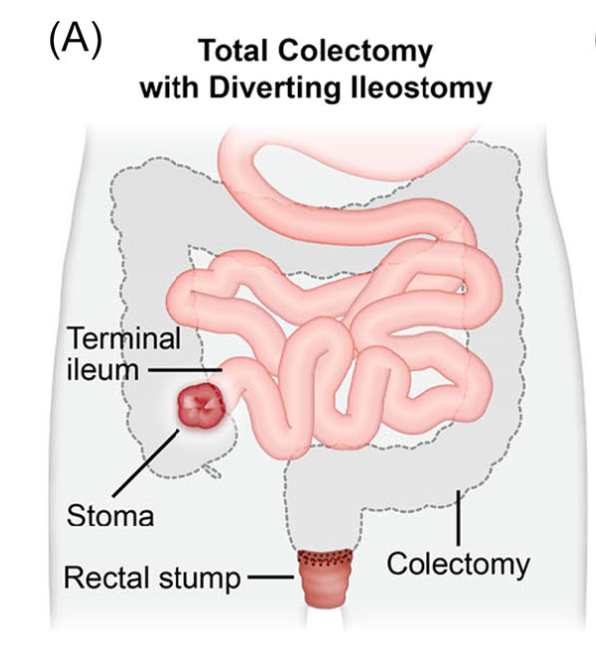
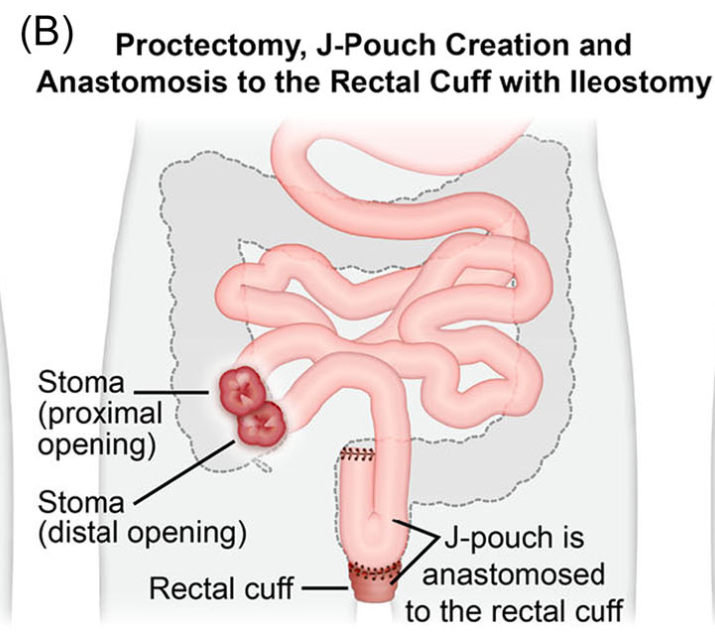
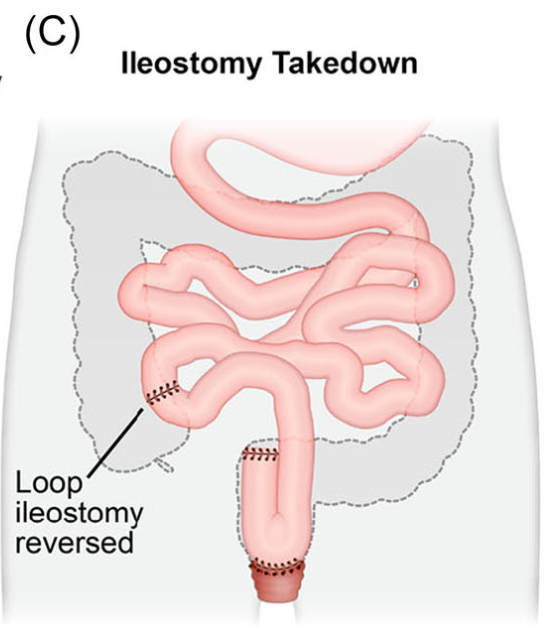
Introduction: Total proctocolectomy with ileal pouch-anal anastomosis (IPAA) can be a life changing solution for a subset of pediatric inflammatory bowel disease (IBD) and familial adenomatous polyposis (FAP) patients. For patients with severe disease a three-stage approach is commonly performed.
Creation of IPAA -Three Stages:
Endoscopic Images and IPAA Anatomy:
The article provides guidance on complications including pouchitis, CD-like inflammation of the pouch, J-pouch failure, fertility after IPAA along with follow-up/screening recommendations.
As for screening, adult guidelines recommend annual screening for IBD patients with high risk features—previous dysplasia, primary sclerosing cholangitis, type C mucosa, refractory pouchitis. In those without these features, guidelines are variable, with one suggesting screening every 5 years. In FAP patients, the recommendation for surveillance screening following IPAA is pouchoscopy every 1–2 years.8
My take: Most pediatric gastroenterologists are not proficient in pouch management due to the small number of our patients needing IPAA. This review provides a terrific review/resource.
This was a two-part study. First the authors examined the frequency of monogenetic rare diseases among patients with primary diagnosis of multiple sclerosis, inflammatory bowel disease (IBD), or atopic dermatitis using the UK Biobank. The UK Biobank is a prospective cohort with >500,000 participants.
In the second part of the study, the authors examined populations with these diseases who had participated in clinical trials. For IBD, the authors utilized five (phase 3) clinical trials includingthe two SERENE trials (SERENE CD, SERENE UC) which examined the use of adalimumab, two risankizumab trials, and one trial of upadacitinib. In total, exome sequencing was performed in 580 with Crohn’s disease and 900 with ulcerative colitis.
This summary of this article focuses on the findings relative to IBD.
Key findings:
In the UK Biobank a diagnosis of a rare monogenetic disease was identified in 53 of 1850 (2.86%) with multiple sclerosis, 75 of 6681 (1.12%) with a diagnosis of inflammatory bowel disease, and 25 of 998 (2.50%) with a diagnosis of atopic dermatitis
Among 1480 clinical trial IBD participants with sequencing data, the authors identified 70 (4.73%) who had a molecular diagnosis of a rare disease
Patients with rare clinical variants responded poorly to medical treatments. For example, in the SERENE-adalimumab studies, 31 of 33 (94%) did not have clinical or endoscopic remission within a year
Discussion Points:
“It is estimated that collectively 4 to 6% of the general population are affected by some form of a rare disease.37” In the absence of routine exome sequencing, diagnosing rare diseases has been a lengthy and difficult process
“The higher fraction of rare diseases identified in the clinical trials cohort (4.73%) than in the U.K. Biobank cohort (1.12%) may be attributed to the targeted recruitment of patients with moderate-to-severe inflammatory bowel disease“
TNFRSF13B was the most common pathogenetic variant in both the Biobank group (25 of 75) and the trials cohort (39 of 70). This variant causes common variable immunodeficiency and “is probably misdiagnosed as inflammatory bowel disease or primarily manifests with inflammatory bowel disease–like symptoms.”
“Rare disease–associated genes may offer insights into potential mechanisms of nonresponse, as we found in this study, and may help in the identification of novel therapeutic targets for inflammatory bowel disease. Conversely, some patients with rare diseases could present opportunities for drug repurposing when they have a serendipitous response to treatments in clinical trials.”
My take:
This study shows that misdiagnosis of rare disease as common conditions is not infrequent.
If the trial IBD population had enrolled young children, the frequency of rare monogenetic diseases would have been higher and captured a wider variety of disorders.
For IBD, use of exome sequencing is widely recommended in those with very early onset disease and is a good idea in those with unusual features and in those who are not responding favorably to treatment.
Recently, Dr. Jennifer Lee gave our group an excellent update on artificial intelligence (AI) for pediatric gastroenterology. My notes below may contain errors in transcription and in omission.
AI is ubiquitous -it helps you login into your phone, helps with traffic apps, filters spam from email, and even edits Bowel Sounds (gets rid of the ‘umms’)
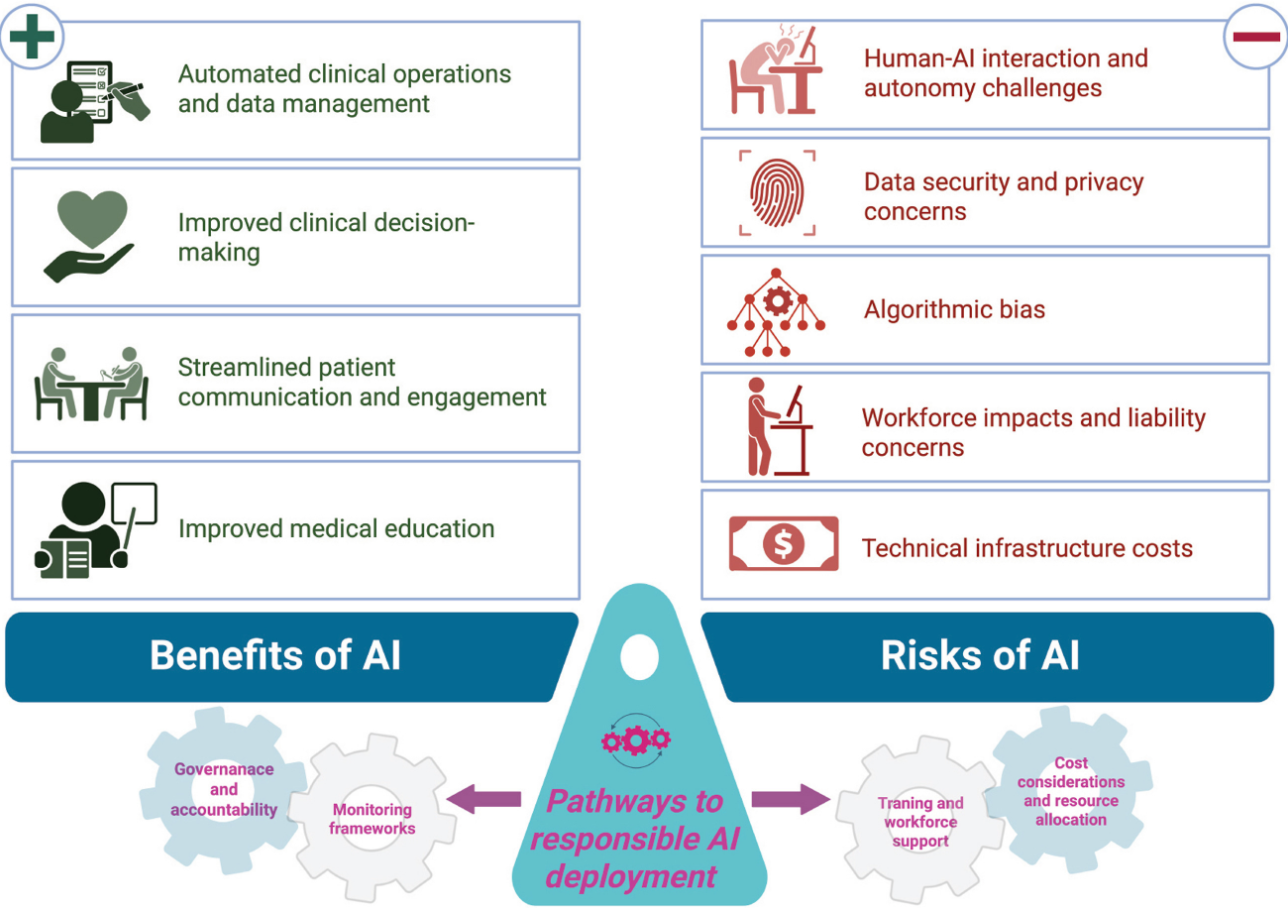
AI can help and AI can harm
Dr. Lee thinks that AI is not going to replace doctors and may help doctors in their clinical work
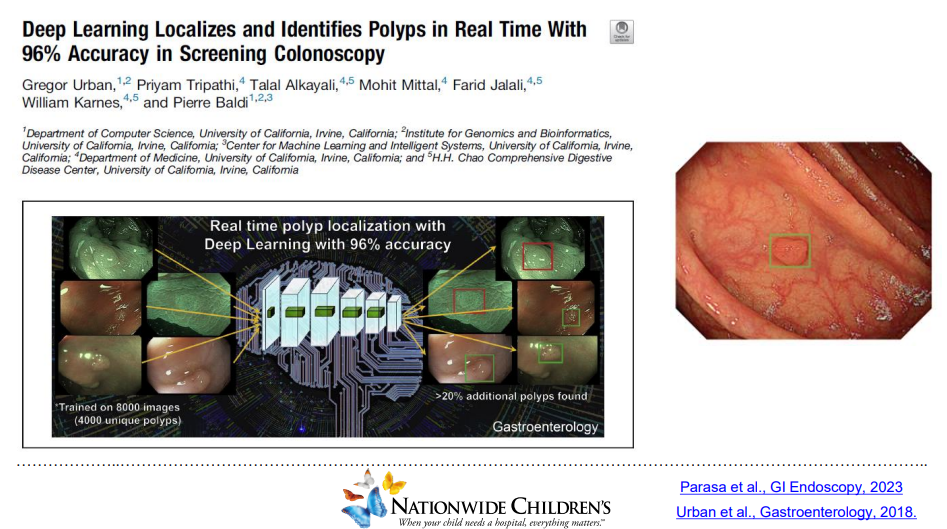
AI is teaching computers to think and predict problems. This can include analyzing radiology images, endoscopic findings (eg. polyps), interpreting EKGs, help with voice recognition, and scribe office visits (still in early stages)
For colonoscopy, AI may aid polyp detection but whether this is clinically meaningful is unclear
With more complex analysis, AI is less transparent
AI algorithms can increase bias
Reliance on AI could lead to skill deterioration. MIT did a study showing less brain activity when using ChatGPT
Generative AI can create a summary of a patient chart. EHRs are partnering with AI
Agentic AI is when AI is set up to act autonomously like reminding patients to get vaccines, reminding to make appointments, or helping schedule appointments
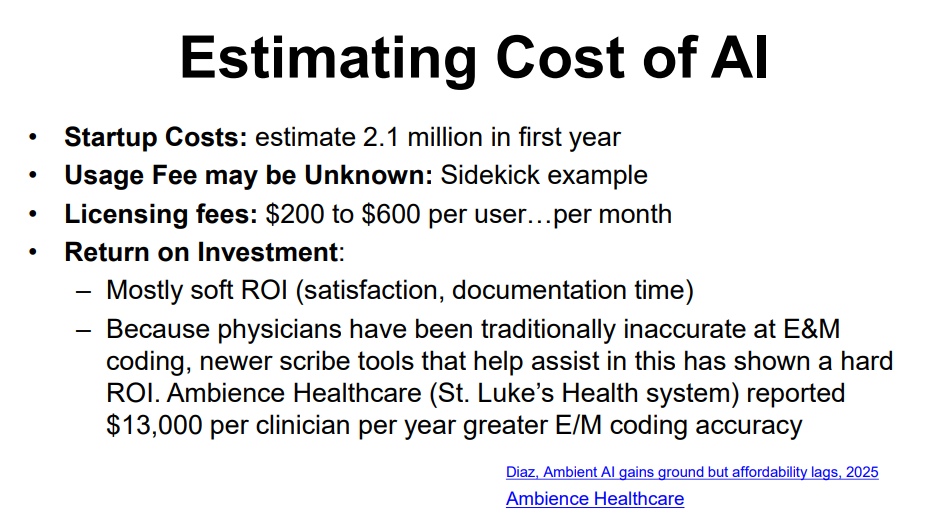
AI in the clinic and hospital may help reduce documentation burden, improve satisfaction and improve safety for patients
AI does have a problem of hallucination (‘making stuff up’) (my comment: so can people). Case report of man admitted to the hospital after following ChatGPT advice in substituting sodium bromide to reduce salt intake (Eichenberger et al. Annal Internal Medicine, 2025. A Case of Bromism Influenced by Use of Artificial Intelligence)
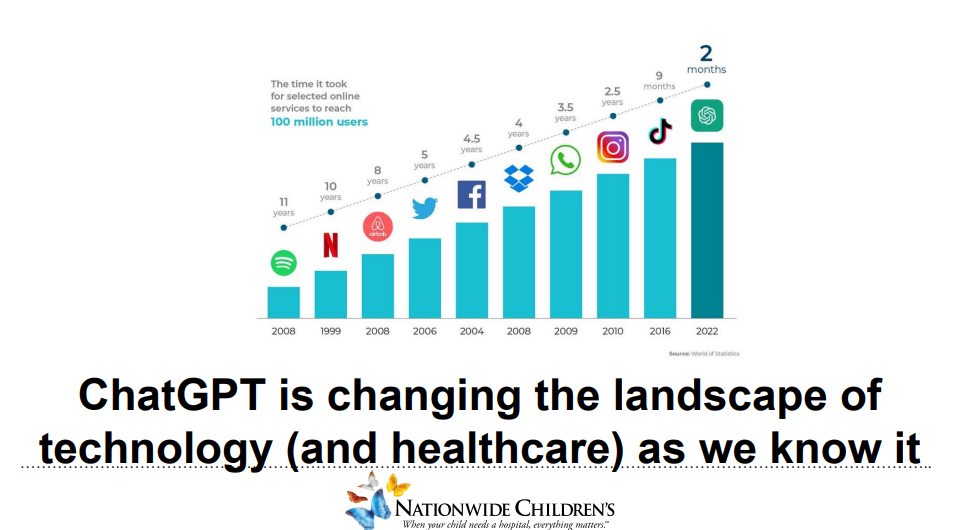
AI tools are still in early stages; however, ChatGPT uptake has been much quicker than previous internet tools
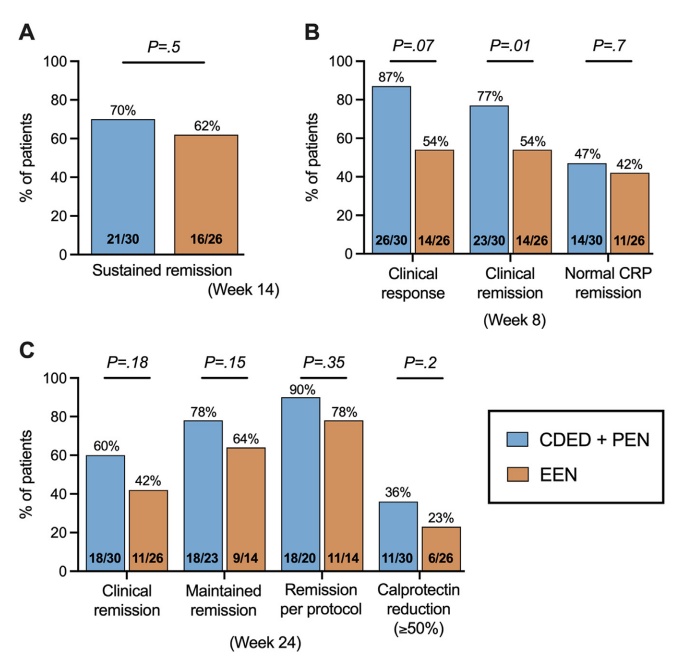
In this “DIETOMICS” study with 56 children with mild-to-severe Crohn’s disease, after a 2 week exclusive enteral nutrition (EEN) diet, 30 patients were randomized to CDED and 26 to EEN.
Diet intervention: The CDED group followed 3 diet phases over 24 weeks: phase 1 (weeks 3–8) supplemented with 50% PEN; phase 2 (weeks 9–14) with 25% PEN, as described previously16; and phase 3 (weeks 15–24) with gradual introduction of more foods, including 1 and 2 free meals per week from weeks 15 and 18, respectively.17 Patients in EEN group received 8 weeks of EEN followed by gradual introduction of free diet with 25% PEN up to week 24.
Key findings:
This study with a relatively small number of enrolled patients had a lot of variables in dietary parameters. “An additional potential confounder in this study is the use of IMM therapy. Although both groups were recommended to initiate IMM therapy from weeks 4 to 5 to maintain remission, several CDED patients opted for monotherapy with CDED and preferred to delay medication initiation. Interestingly, 90% of patients on CDED without IMM therapy were in remission at week 14 and 100% were in remission at week 2” (possibly impacting decision not to use IMM).
My take: This study adds another piece of information to the puzzle on dietary therapy for Crohn’s disease. The authors note the following: “while CDED shows promise as a standalone therapy in some cases, in more severe cases it may be more appropriately as an adjuvant to top-down treatment with early anti-TNF.4 Recent research and guidelines advocate for a top-down approach (anti-TNF ± nutrition) for more severe disease, emphasizing the integration of anti-TNF therapy with nutrition.8,29 This approach is crucial during critical growth stages, as the conventional step-up method may lead to ineffective use of IMM with prolonged steroid exposure and growth issues.12“
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition
The approval for pediatric IBS-C was supported by extrapolation of efficacy from adequate and well-controlled studies in adults and a 12-week double-blind, randomized, parallel-group trial in pediatric patients 7-17 years of age who met modified Rome III criteria for child/adolescent IBS-C. The recommended dosage for this indication is 145 mcg orally once daily.1…
In 2023, the FDA approved linaclotide for the treatment of pediatric patients aged 6-17 years with functional constipation at a recommended dosage of 72 mcg orally once daily.
Also, NBC news (11/08/25): ByHeart baby formula recalled amid 10-state outbreak of infant botulism The U.S. Food and Drug Administration said the outbreak includes 13 hospitalizations since August of children who consumed ByHeart Whole Nutrition Infant Formula. No deaths have been reported.
The recall includes two lots of the powdered formula with Dec. 1 “use by” dates, the FDA said in a statement Saturday. The lot numbers are 206VABP/251261P2 and 206VABP/251131P2…The FDA says ByHeart makes up less than 1% of the baby formula sold in the U.S.
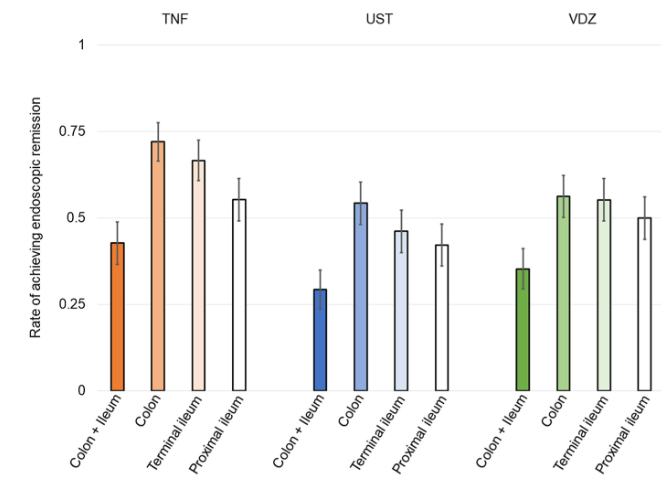
This multicenter prospective study (n=253) examined efficacy of treatment in patients with proximal ileal disease using balloon-assisted enteroscopy (BAE). The recruited patients had a mean disease duration of 4 years. 52% were naive to biologic treatment at baseline.
Key findings:
At baseline, 74 patients (29.2%) had proximal ileal ulcerations without terminal ileal ulcerations
At week 26, after treatment with anti-TNF therapy (n=103), ustekinumab (n=99) or vedolizumab (n=51), endoscopic remission was achieved in 91 patients (36.0%). Of the patients with complete ulcer healing of the terminal ileum, 28.6% (22/77) had residual ulcers in the proximal ileum
The rate of endoscopic remission in the proximal ileum (50.9%) was relatively lower compared with the colon (63.4%) and terminal ileum (56.7%)
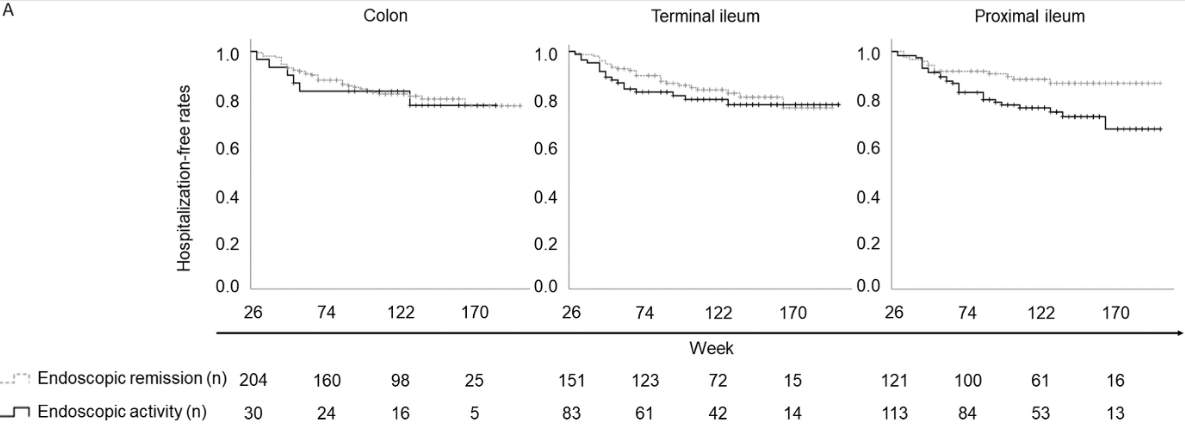
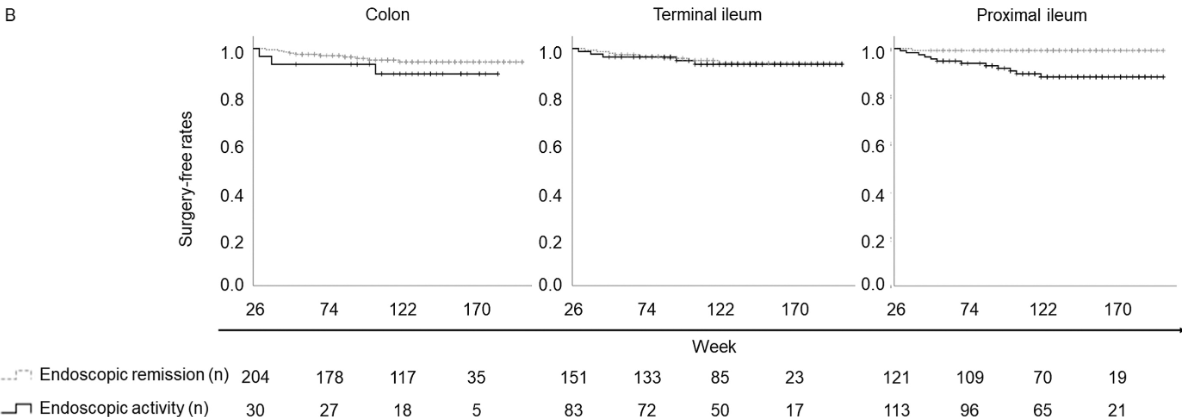
After a median follow-up of 134 weeks, residual ulcerations in the proximal ileum were associated with a poorer prognosis (P = .0126 for hospitalization and P = .0014 for surgery). In contrast, there was no significant differences in hospitalization and surgery associated with endoscopic activity vs remission in the colon or terminal ileum.
Discussion: Residual “proximal ileal ulcerations … are associated with a poorer prognosis…Additionally, we confirmed that proximal ileal inflammation is less responsive to biologic therapies compared with colonic inflammation. Although the reasons for this disparity remain unclear”
My take: Balloon-assisted enteroscopy is not frequently used in the setting of inflammatory bowel disease, particularly in pediatrics. MRE is typically used to follow proximal small bowel disease, though it has less sensitivity for luminal mucosal disease.