I am a pediatric gastroenterologist at GI Care for Kids (previously called CCDHC) in Atlanta, Georgia. The goal of my blog is to share some of my reading in my field more broadly. In addition, I wanted to provide my voice to a wide range of topics that often have inaccurate or incomplete information.
Before starting this blog in 2011, I would tear out articles from journals and/or keep notes in a palm pilot. This blog helps provide an updated source of information that is easy to access and search, along with links to useful multimedia sources.
I was born and raised in Chattanooga. After graduating from the University of Virginia, I attended Baylor College of Medicine. I completed residency and fellowship training at the University of Cincinnati at the Children’s Hospital Medical Center. I received funding from the National Institutes of Health for molecular biology research of the gastrointestinal tract.
During my fellowship, I had the opportunity to work with some of the most amazing pediatric gastroenterologists and mentors. Some of these individuals included Mitchell Cohen, William Balistreri, James Heubi, Jorge Bezerra, Colin Rudolph, John Bucuvalas, and Michael Farrell. I am grateful for their teaching and their friendship. During my training with their help, I received a nationwide award for the best research by a GI fellow.
I have authored numerous publications/presentations including original research, case reports, review articles, and textbook chapters on various pediatric gastrointestinal problems. In addition, I have been recognized by Atlanta Magazine as a "Top Doctor" in my field multiple times.
Currently, I am the vice chair of the section of nutrition for the Georgia Chapter of the American Academy of Pediatrics. In addition, I am an adjunct Associate Clinical Professor of Pediatrics at Emory University School of Medicine. Other society memberships have included the North American Society for Pediatric Gastroenterology Hepatology and Nutrition (NASPGHAN), American Academy of Pediatrics, the Food Allergy Network, the American Gastroenterology Association, the American Association for the Study of Liver Diseases, and the Crohn’s and Colitis Foundation.
As part of a national pediatric GI organization called NASPGHAN (and its affiliated website GIKids), I have helped develop educational materials on a wide-range of gastrointestinal and liver diseases which are used across the country. Also, I have been an invited speaker for national campaigns to improve the evaluation and treatment of gastroesophageal reflux disease, celiac disease, eosinophilic esophagitis, hepatitis C, and inflammatory bowel disease (IBD). Some information on these topics has been posted at my work website, www.gicareforkids.com, which has links to multiple other useful resources.
I am fortunate to work at GI Care For Kids. Our group has 17 terrific physicians with a wide range of subspecialization, including liver diseases, feeding disorders, eosinophilic diseases, inflammatory bowel disease, cystic fibrosis, DiGeorge/22q, celiac disease, and motility disorders. Many of our physicians are recognized nationally for their achievements. Our group of physicians have worked closely together for many years. None of the physicians in our group have ever left to join other groups. I have also worked with the same nurse (Bernadette) since I moved to Atlanta in 1997.
For many families, more practical matters about our office include the following:
– 14 office/satellite locations
– physicians who speak Spanish
– cutting edge research
– on-site nutritionists
– on-site psychology support for abdominal pain and feeding disorders
– participation in ImproveCareNow to better the outcomes for children with inflammatory bowel disease
– office endoscopy suite (lower costs and easier scheduling)
– office infusion center (lower costs and easier for families)
– easy access to nursing advice (each physician has at least one nurse)
I am married and have two sons (both adults). I like to read, walk/hike, bike, swim, and play tennis with my free time.
I do not have any financial relationships with pharmaceutical companies or other financial relationships to disclose. I have helped enroll patients in industry-sponsored research studies.
Key finding: In 3 large adult US prospective cohorts (n=208,280), gluten intake was not associated with risk of CD or UC in 5,115,265 person-years of follow-up evaluation.
My take (from authors): These ” findings are reassuring at a time when consumption of gluten has been increasingly perceived as a trigger for chronic gastrointestinal diseases.”
“The basic concept is similar to distraction osteogenesis, which orthopedic surgeons have used for years, applying distraction force to broken bone that will grow up to a millimeter a day,” said Andre Bessette, the CEO and a co-founder of Eclipse Regenesis, Inc…
To regenerate small-bowel tissue, a surgeon inserts the device, which looks like a small, compressed coil, inside the small intestine and secures both ends with plication sutures applied to the outside of the intestine. Over two to three weeks, the device slowly expands to its uncompressed state, stimulating new tissue growth—ultimately two to three times the segment’s original length, about 4 cm...[thus] they’ll need more than one device applied or more than one procedure.
Once this process is complete, the chromic sutures dissolve over about a month, allowing the device to pass through the body to be excreted...
[The researchers] expect to start these [human] trials in the first half of 2022, and they haveidentified two primary investigator sites: Boston Children’s Hospital and Cincinnati Children’s Hospital
Like many clinicians, I would very much like to tell insurance companies how I really feel about their prior authorization policies, and peer-to-peer processes to get approvals needed for treating our patients.
Most of the time I resent the imposition on my time to craft detailed letters explaining my rationale for treatment. Some obstructionist tactics are particularly aggravating. For example, when I am asked to do a peer-to-peer call and find out on the call that the person on the other end is neither a peer (often a pharmacist) and more importantly that this person is not authorized to remedy the situation but only to arrange another call. Another tactic of asking me to write multiple letters at different stages of the authorization process is extremely annoying. All told, these authorization requests are becoming more frequent and further impinging on my free time.
Now it turns out a study has shown the harmful effects of these maneuvers for our patients:
In this retrospective study of 190 pediatric patients ((median age 14.5 years) with IBD initiating biologics at a tertiary care hospital, key findings:
Prior authorization and complicated prior authorizations (requiring appeal, step therapy, or peer-to-peer review) were associated with 10.2-day (95% confidence interval [CI] 8.2 to 12.3) and 24.6-day (95% CI 16.4 to 32.8) increases in biologic initiation time, respectively.
Prior authorizations increased the likelihood of IBD-related healthcare utilization within 180 days by 12.9% (95% CI 2.5 to 23.4) and corticosteroid dependence at 90 days by 14.1% (95% CI 3.3 to 24.8).
In their discussion, the authors note that “in a recent survey conducted by the American Medical Association, 94% of physicians reported that prior authorizations delay access to necessary care, 90% perceived a negative impact on clinical outcomes, and 30% reported that a prior authorization led to a serious adverse event for a patient in their care.”
My take: Prior authorization policies usually delay needed care unnecessarily and lead to complications in children with IBD.
In 2014, one of the posts on this blog addressed stopping anti-TNF therapy: Marriage, Divorce and Separation with Anti-TNF Therapy. My take at that time was “most patients are better off staying married to their anti-TNF therapy.”
Despite changes in therapeutic options, a recent study and editorial come to the same conclusion in 2022:
In the retrospective study, 78 patients with CD and 56 patients with UC underwent endoscopic reassessment. Key findings:
Mucosal healing (MH) was achieved by 32 patients with CD (41%) and 30 patients with UC (53.6%); 26 patients with CD (33.3%) and 22 patients with UC (39.3%) achieved histologic healing (HH)
Among 45 patients (n=24 CD, n=21 UC) with both MH & HH, anti-TNF therapy was stopped & patients received either an immunomodulatory or mesalamine. 76% of patients with CD had clinical relapse within 3 years and 17% within 1 year. Importantly, objective markers of relapse, including calprotectin and endoscopy were NOT performed; thus, this is certainly an underestimation of relapse rate and time to relapse.
In the commentary, the authors note the high rate of relapse in other studies with anti-TNF withdrawal (eg. STORI trial) and high rate of surgery in patients with perianal CD who stopped therapy. In the STORI trial, “the best outcomes [for infliximab withdrawal] were those with subtherapeutic infliximab trough levels, ie, those for whom infliximab was not responsible for maintaining their remission.”
The data are less certain for UC. The editorial notes that 85% of the 21 patients in the Scarallo study had limited left-sided colitis and only 17 were followed for at least 1 year. In adult studies on anti-TNF discontinuation with UC (Kennedy et al. Aliment Pharm Ther 2016; 43: 910-23 and Molander et al. Inflamm Bowel Dis 2014; 20: 1021-28), 42% and 35% relapsed within 12 months, whereas another small study (Farkas et al. World J Gastroenterol 2014; 20: 2995-3001) found 100% of patients on combination therapy who stopped anti-TNF agent had to restart anti-TNF therapy.
My take (from editorial): “The totality of the currently available evidence suggests that discontinuing anti-TNF medications in children with IBD is associated with a greatly increased risk of disease exacerbation, especially if the anti-TNF trough level was therapeutic.”
This retrospective review of 45 patients (n=92 stents) examine the effectiveness of esophageal stenting in patients with esophageal atresia (EA). All patients had multiple dilatations prior to stenting and/or had a stricture diameter that rapidly narrowed within 2 weeks of dilatation to a diameter that was the same or smaller to predilatation. Patients were observed in the hospital after stent placement and outpatient management was considered if oral nutrition was tolerated for at least 3 days.
Key findings:
According to the authors, the stents prevented surgical resection in 41% of patients
ΔD (change in diameter) of ≤4 mm (area under the curve = 0.790; 95% confidence interval: 0.655–0.924; P < 0.001) was the optimal cutoff point in differentiating stent success. If the change in diameter decreases by 4 mm or more after stent removal at endoscopic followup, it is likely that stricture contains significant scar tissue and is not amenable to dilatation/stenting.
Median stent duration was 11.5 days
The most common adverse events were erosions/ulcerations (29%), granulation tissue formation (27%), vomiting/retching (26%) and stent migration (9%). Three stents were complicated by an esophageal leak (treated medically).
My take: Complications were frequent; thus, stenting for refractory strictures requires highly-specialized technical expertise.
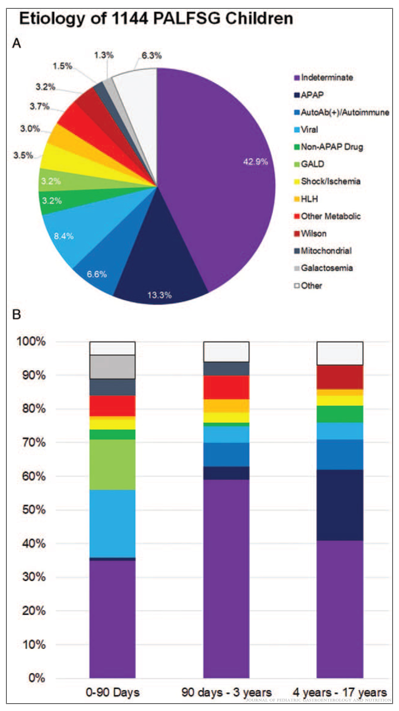
This article provides a terrific summary of the most urgent issues with regard to caring for children with PALF; this article provides helpful information for diagnosis, and management, as well as information on pathophysiology, and associated outcomes.
The article makes a number of recommendations for testing/treatment -here are a few of them:
While the initial testing does list ferritin, it does not list soluble IL2R as an early test (listed lower in Table 4 under section of hepatic encephalopathy). My colleagues at Emory who specialize in liver transplantation have frequently recommended this test early in the evaluation of severe liver disease/acute liver failure (ALF) as a potential marker of HLH and immune dysregulation.
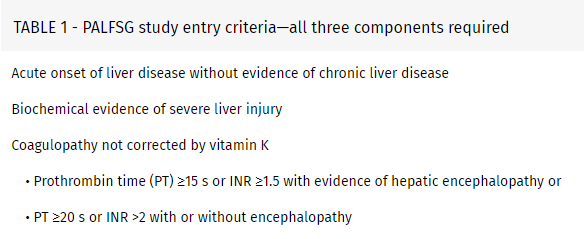
With regard to coagulopathy: “Coagulopathy secondary to vitamin K deficiency should rapidly correct following appropriate repletion. Notably, if coagulopathy persists, efforts to “correct” abnormal coagulation profiles with fresh frozen plasma or other pro-coagulation products should generally be avoided” [in the absence of bleeding or need for invasive procedure].
Initial IV Fluids: ” In the absence of the need for volume resuscitation, total intravenous fluids should initially be restricted to around 90% of maintenance fluids to avoid overhydration. Initial fluids should be similar to hypertonic glucose (D10) one-half normal saline and supplemented with 15 mEq of potassium (K+)/L.”
Nutritional support: “Patients with PALF are likely catabolic and require more calories than basal needs. Enteral feeding is often preferred over total parenteral nutrition (TPN), and both naso-gastric or naso-jejunal feeds should be considered before TPN.”
Neonatal ALF: “GALD results from an intrauterine alloimmune liver injury and is suspected to be the single most common cause of neonatal acute liver failure… Characteristic clinical features of GALD include an ALF presentation usually at birth and almost always in the first days of life. The majority (70–90%) of affected infants are born premature and a history of maternal sibling death is common. Timely exchange transfusion and high-dose intravenous immunoglobulin (IVIG) is the preferred treatment to remove offending antibodies and block their action, including activation of complement (88,91). The mechanism of GALD places subsequent pregnancies at risk, and intrapartum IVIG should be used to prevent recurrences.”
Table 8 list common medications implicated in PALF. “Acetaminophen (APAP) …remains the most common cause of DILI, and is the most common identified cause of ALF in children.”
Time to Adjust the Knowledge Doubling Curve in Hepatology In this post, AASLD expert guidance: for platelets in the setting of cirrhosis: “Given the low risk of bleeding of many common procedures, potential risks of platelet transfusion, lack of evidence that elevating the platelet count reduces bleeding risk, and ability to use effective interventions, including transfusion and hemostasis if bleeding occurs, it is reasonable to perform both low‐ and high‐risk procedures without prophylactically correcting the platelet count.” For INR in setting of cirrhosis: “The INR should not be used to gauge procedural bleeding risk in patients with cirrhosis who are not taking vitamin K antagonists (VKAs)…Measures aimed at reducing the INR are not recommended before procedures in patients with cirrhosis who are not taking VKAs…FFP transfusion before procedures is associated with risks and no proven benefits.”
Figure 3: Etiology of acute liver failure in children. (A) Etiology for 1144 children from the Pediatric Acute Liver Failure Study Group (PALFSG) 1999–2014. (B) Final diagnosis by age (note: figure B includes information on only 985 participants)
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Using several national surveys (2016-2018), the authors provide data on GI diagnoses and expenditures for adults and children
Key findings:
Gastrointestinal health care expenditures totaled $119.6 billion in 2018.
Annually, there were more than 36.8 million ambulatory visits for gastrointestinal symptoms and 43.4 million ambulatory visits with a primary gastrointestinal diagnosis
A total of 22.2 million gastrointestinal endoscopies were performed, and 284,844 new gastrointestinal cancers were diagnosed
Gastrointestinal diseases and cancers caused 255,407 deaths
This article is loaded with statistical details
Abdominal pain, reflux, and constipation are the leading GI diagnoses
GI bleeding, cholelithiasis, pancreatitis and liver disease are the most common diagnoses associated with admission to the hospital
In the pediatric age group, appendicitis, intestinal infection and inflammatory bowel disease are the principal diagnosis associated with GI admissions
Trends in GI cancer frequency over the last three decades are shown (including ethnicity)
Among non-malignancy, alcohol-associated liver disease followed by cirrhosis and GI bleeding were most common causes of death in GI/Liver categories
Data on the frequency of colonoscopies and transplants is provided
In this report, the authors describe nine patients with refractory microscopic colitis (median age 55 years) who were treated with vedolizumab.
Key findings:
Clinical response with induction in 9 (100%); time to >50% response ranged from 1 to 7 weeks with 5 patients responding within 2 weeks.
Sustained response with maintenance therapy in 6 (67%); duration of follow-up ranged from 1 month to 15 months. The three patients without response had symptom duration of 10 yrs, 12 yrs, and 25 yrs prior to institution of vedolizumab.
Only two patients had histologic follow-up. While both had clinical response, the patient with lymphocytic colitis had histologic resolution whereas a patient with collagenous colitis had histologic persistent.
My take: Given vedolizumab’s favorable safety profile, further studies (with endoscopic endpoints) of vedolizumab are needed to define its efficacy for microscopic colitis.
Key finding: The risk of serious infections was not different between vedolizumab and anti-TNF in the overall IBD cohort (HR, 0.95; 95% CI, 0·79-1.13), while the risk was decreased for vedolizumab users in patients with UC (HR, 0.68; 95% CI, 0.50-0.93), but not CD (HR, 1.10; 95% CI, 0.87-1.38)
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Reported prevalence of food allergy after liver transplant ranges from 5% to 40%
Younger age at transplantation is a risk factor for developing de novo post-transplant food allergy (dnPTFA)
Tacrolimus has been implicated as a risk factor for dnPTFA
Common dnPTFA are the same as in the general population: milk, egg, wheat, peanouts/nuts, fish, and soy
Management recommendations:
If the donor has a food allergy, the recipient should be tested within the first months of transplant for food-specific IgE and “it is advisable to introduce the suspected food in a controlled setting”
Elimination diet is mainstay of treatment. Some individuals may need modification of their immunosuppressive medications
Provide self-injectable epinephrine in those with food allergy
Monitoring of specific IgE/skin prick tests is advised
My take: There are increased allergy issues in kids who have had liver transplantation.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.