It’s hard not to be fascinated by the emerging treatments in gene therapy. A great summary of this topic as it relates to gastroenterology:
RL Kruse et al. Gastroenterol 2022; 162: 1019-1023. Open Access: How to Embrace Gene Therapy in Gastroenterology
Key points:
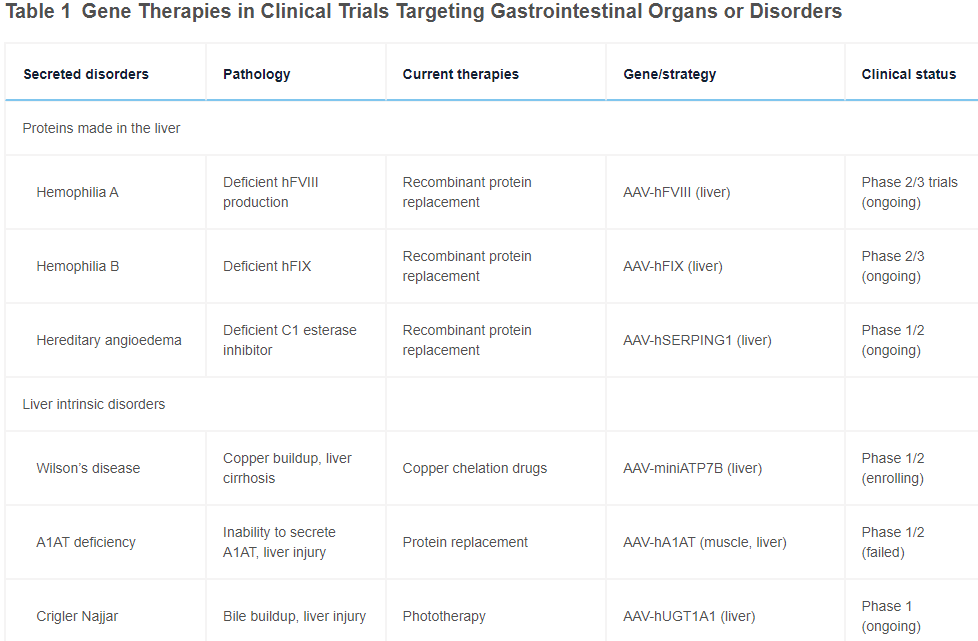
- Researcher’s have utilized viruses to introduce exogenous DNA in efforts to correct defects in genetic diseases. Adeno-associated virus (AAV) vectors are the most common vectors used. In addition, AAV have a natural tropism to the liver following intravenous infusion
- “Highlighting programs with the most advanced efficacy, hemophilia gene therapies in the liver have advanced into phase 2/3 and have shown promising efficacy based on factor VIII or IX levels achieved and reduction in bleeding events, with the main questions being long-term expression and safety of the approach”

Limitations:
- “Integrated AAV have been associated with an increased incidence of hepatocellular carcinoma in mice”
- Antibodies to AAV may be present or develop after infusion…” this factor has precluded any redosing in trials because antibodies would neutralize all incoming vectors”
- In hemophilia trials, in the liver there has been a slow decrease in the levels of expression over time 6 which indicates that years into the future patients will need to be redosed to maintain efficacy
- “Practically, AAV can only achieve delivery in a fraction of cells within an organ”
Newer Approaches for Gene Delivery:
- mRNA delivery: mRNA is being explored as a tool for gene therapy, because mRNA only requires cytoplasmic delivery for expression.
- “mRNA can also express gene-editing enzymes like Cas9….However, gene editing presents inherent risks of off-targeting cutting or base editing that would occur in millions of hepatocytes, potentially leading to cancer”
- “Nonviral approaches of DNA delivery could drop the costs of vector production at least 100-fold versus AAV…delivery of DNA through LNPs [lipid nanoparticles] has largely yielded inefficient gene expression”
- “Hydrodynamic injection is a process where fluid pressure is used to deliver naked DNA directly into cell…injection into the biliary system through endoscopic retrograde cholangiopancreatography”
The authors note that gene delivery could be important in modifying more common disorders including nonalcoholic steatohepatitis, diabetes and autoimmune diseases.
My take: While this field of study is quite exciting, to me it is definitely a shiny object, like all of precision medicine, in that it may distract researchers and physicians away from more pressing common problems.
Related blog posts:
- “Our Gene-Edited Future”
- What is Wrong with the Glimmer of “Precision Medicine”
- Zip Code or Genetic Code -which is more important for …
- Genetically Modified Humans: Genome Editing 101
- “Issue-attention cycle” problem. “This pattern occurs when initial public alarm over the discovery of a problem and optimism about its quick resolution are replaced by the realization that solving the problem will require some public sacrifice and will displace powerful societal interests.”from Weight of the Nation | gutsandgrowth
- The Narrow Path of Personalized Cancer Medicine | gutsandgrowth