VO Puntmann et al. Full text: Outcomes of Cardiovascular Magnetic Resonance Imaging in Patients Recently Recovered From Coronavirus Disease 2019 (COVID-19)
Conclusion: In this study of a cohort of German patients recently recovered from COVID-19 infection, CMR revealed cardiac involvement in 78 patients (78%) and ongoing myocardial inflammation in 60 patients (60%), independent of preexisting conditions, severity and overall course of the acute illness, and time from the original diagnosis. These findings indicate the need for ongoing investigation of the long-term cardiovascular consequences of COVID-19.
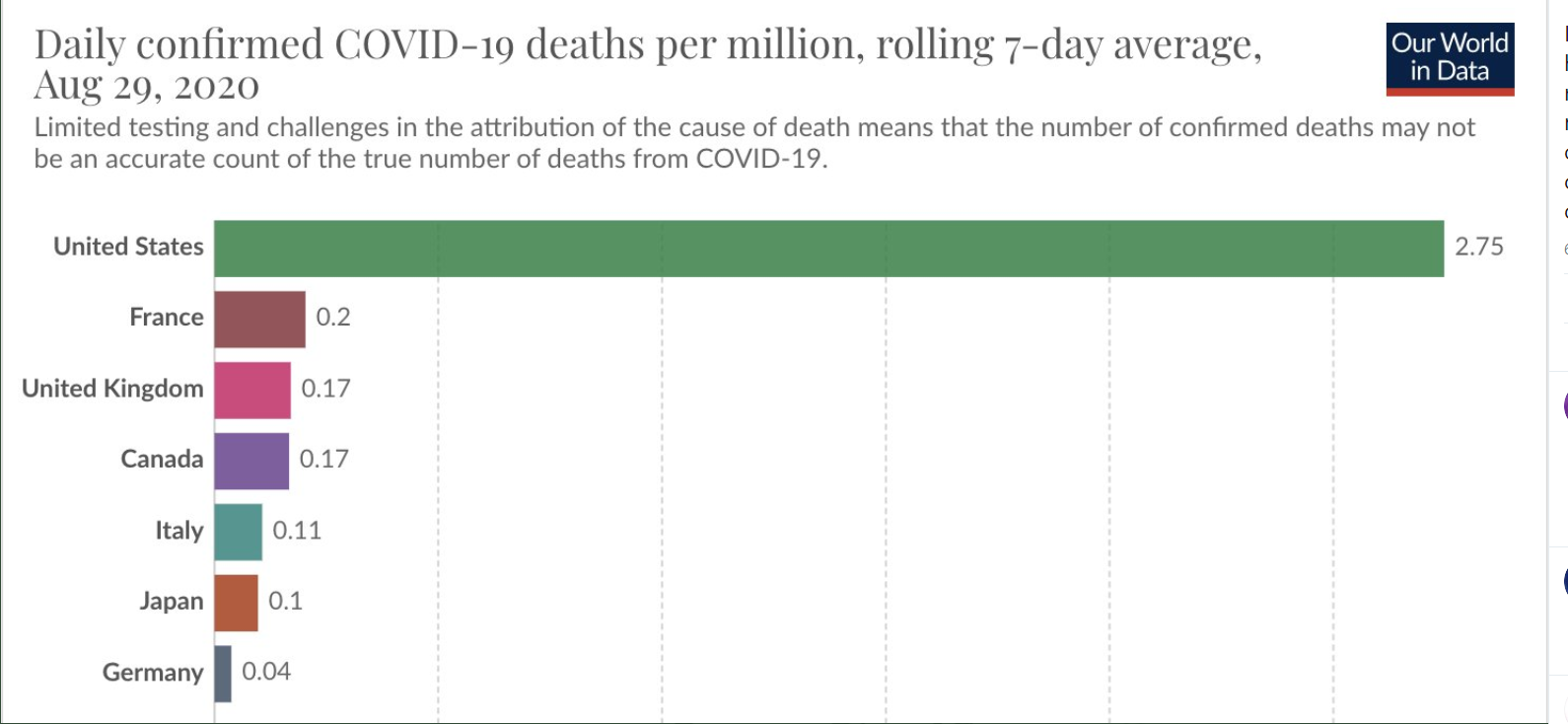
NY Times: E Emanuel et al. Where Is America’s Groundbreaking Covid-19 Research? The U.S. could learn a lot from Britain.
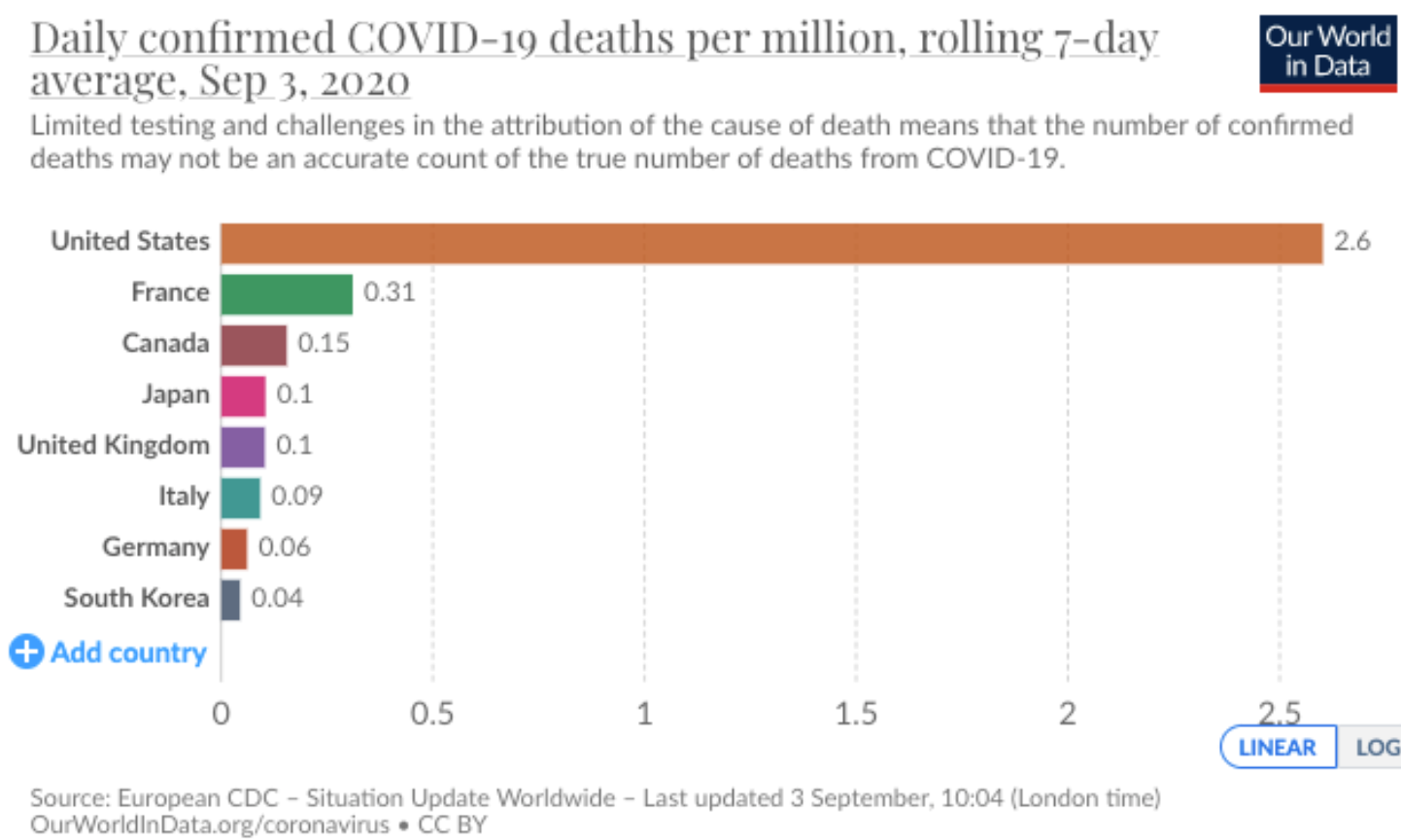
Excerpt: “ Yet with over six million coronavirus cases and 183,000 deaths, the United States has produced little pathbreaking clinical research on treatments to reduce cases, hospitalizations and deaths. Even one of the most important U.S. studies to date, which showed that the antiviral drug remdesivir could reduce the time Covid-19 patients spent in the hospital to 11 days from about 15, had too few subjects to demonstrate a statistically significant reduction in mortality…[British] researchers found no benefits from the use of hydroxychloroquine in hospitalized Covid-19 patients, nor from the lopinavir-ritonavir drug combination. On the other hand, dexamethasone, an inexpensive steroid, was found to reduce mortality by up to one-third in hospitalized patients with severe respiratory complications.”
“Unfortunately, unlike Britain, the United States has lacked a clear, unified message from government health care leaders, major insurance companies and hospital systems to put in place large, simple randomized trials that are considered the standard of care for Covid-19 treatment. We need to change that muddled approach now and reassert the nation’s clinical research excellence.”
NY Times: Roni Rabin. How a Bus Ride Turned Into a Coronavirus Superspreader Event
An excerpt: “A passenger on one of the buses had recently dined with friends from Hubei. She apparently did not know she carried the coronavirus. Within days, 23 fellow passengers on her bus were also found to be infected.
It did not matter how far a passenger sat from the infected individual on the bus, according to a study published in JAMA Internal Medicine on Tuesday. Even passengers in the very last row of the bus, seven rows behind the infected woman, caught the virus…
The new study “adds strong epidemiological evidence that the virus is transmitted through the air, because if it were not, we would only see cases close to the index patient — but we see it spread throughout the bus,” said Linsey Marr…
[THIS] took place on Jan. 19, when there were still no confirmed Covid-19 cases reported in Ningbo…The potential for airborne transmission in close confined spaces raises concern about the winter months, when people will be spending more time indoors, Dr. Marr said. Her advice: “Avoid crowded indoor spaces where people are not wearing masks and the ventilation is poor.”