

Author Archives: gutsandgrowth
Endoscopic Experts Needed In Pediatrics
A recent study (A Schmidt et al. Gastroenterol 2018; 155: 674-86) shows how a new endoscopic technique, over-the-scope clips (OTSC), are more effective than standard endoscopic therapy for patients with recurrent bleeding of peptic ulcers.
Key finding: A multicenter prospective randomized unblinded study with 66 patients (33 in each arm) with found that hemostasis with OTSC had a failure rate (further bleeding) of 15.2% compared with 57.6% in those with standard therapy.
The authors note that standard endoscopic techniques are effective in more than 90% with rebleeding rates of 2-10%. In those with rebleeding, followup endoscopy has a much lower success rate.
My take:
- This study highlights a problem in pediatric endoscopy –the lack of expertise in these rare cases. To learn even ‘standard’ endoscopic therapy, most pediatric GI fellows will need to collaborate with adult gastroenterologists in order to have exposure to a sufficient number of cases.
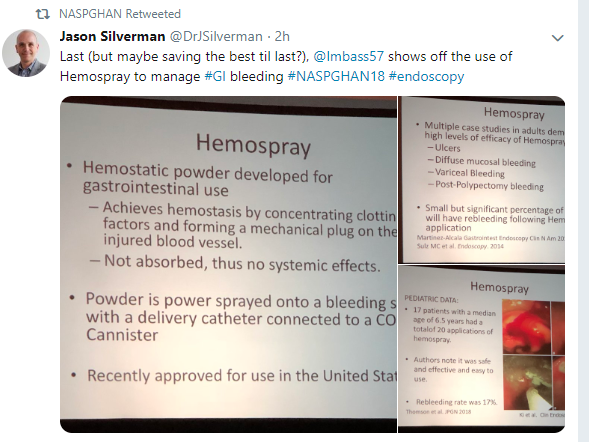
- The development of alternatives like hemospray (Hemospray for GI Bleeding) which is technically-easy should be helpful for pediatric endoscopists with less endoscopic training.
Related article:
P Tran et al. JPGN 2018; 67: 458-63. This retrospective analysis of 11 pediatric cases (median age 14.7 yrs) reported technical success in all cases, though 2 patients with anastomotic ulcers requred additional medical intervention. The article has some pretty cool pictures.
Related blog posts:

Lake Agnes, Banff
Lake Agnes Teahouse Menu
Briefly Noted: Progression of Fatty Liver Disease on MRI
M Mouzaki et al. J Pediatr 2018; 201: 86-92. This study with 65 patients evaluated nonalcoholic fatty liver disease (NAFLD) progression between two MRI studies, with a median time span of 27 months.
Key findings:
- There was no correlation between change in liver stiffness and change in ALT; there was a weak correlation between ALT change and fat fraction.
- MRI fat fraction and stiffness decreased in 29% and 20% of patients respectively and increase in 25% and 22% respectively.
My take: When we find effective therapies, we will need better non-invasive markers to follow NAFLD progression.
Related blog posts
- NAFLD Guidance from AASLD 2018
- Pediatric NAFLD Guidelines 2017
- Concise Review: Fatty Liver in Pediatrics
- Ultrasound Unreliable to Exclude Fatty Liver
- A liver disease tsunami | gutsandgrowth
- Increasing prevalence of pediatric NAFLD | gutsandgrowth

Tea House Trail, near Lake Louise, Banff
Briefly noted: Selective Serotonin Reuptake Inhibitors (SSRIs) and Linear Growth
CA Calarge et al. J Pediatr 2018; 201: 245-51. This study analyzed data from 4 separate trials with a total of 267 boys treated with risperidone. In this cohort, 71% had taken an SSRI.
Key finding: The duration and cumulative dose of SSRI was inversely associated with height z score, especially during Tanner 3 and 4 stages. The effect was approximately 1 cm for every year of treatment.
The authors speculate that SSRIs could “alter serotonin signaling, which is known to control GH secretion.”
My take:
- This study shows an association between SSRIs and linear growth but it remains unclear if this affects adult height (could postpone growth).
- This potential adverse effect needs to be considered in the clinical picture of the severe impairment and distress that can occur due to untreated depression and anxiety.
Related blog post: Brave New World: Psychotropic Manipulation and Pediatric Functional GI Disorders

Lake Louise, Banff
Why I Don’t Check Vitamin D Levels During IBD Flare-ups
A recent study (C Striscuiglio et al. JPGN 2018; 67: 501-6) helps explain the role of inflammation on vitamin D levels in pediatric patients (n=51) with inflammatory bowel disease (IBD).
Key findings:
- The free/total 25-OH D ratio was higher in patients with newly-diagnosed IBD compared to healthy controls (P< .001)
- A significant direct correlation was found between free/total 25-O D ratio and the activity index of disease (P= .01)
- While there was frequent deficiency in total vitamin D levels, the free 25-OH D which is the active form of vitamin D was normal or elevated in patients with newly-diagnosed IBD; this, in turn, was due to a decrease in vitamin-D binding protein which is related to inflammation. The authors hypothesized that at the cellular level in the intestine, there may be peripheral resistance due to inflammation and even supratherapeutic levels of free vitamin D could be needed to produce the active form (1,25-OH D).
My take: This study shows that 25-OH D levels (total) have almost no value at the onset of IBD. Even normal or elevated free levels of 25-OH D which were found in this study does not preclude the potential need to supplement with vitamin D according to the study authors. In addition, as noted in previous posts, Vitamin D levels can normalize without supplementation when the patient’s IBD responds to therapy.
Related blog posts:
- What happens to micronutrient levels in the hospital setting? When CRP concentration is >20 mg/L (>2 mg/dL), “plasma concentrations of selenium, zinc, and vitamins A, B-6, C, and D are clinically uninterpretable.
- Get Here if You Can: Improved Vitamin D Status
- Single High-Dose Oral Vitamin D Therapy (Stoss) for Children …
- Explaining the Vitamin D Paradox | gutsandgrowth
- Vitamin D, IBD, and Causality | gutsandgrowth
- Common to be “D-ficient” | gutsandgrowth
- Vitamin D deficiency and metabolism in pediatric… | gutsandgrowth
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications/diets (along with potential adverse effects) should be confirmed by prescribing physician/nutritionist. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.

Dangerous animal –seen on our hike to the tea house, Banff
#NASPGHAN18 -Our Poster on Antibiotic Stewardship and PEG Placement
Thanks to Chelly Dykes for presenting poster later today and to co-authors for collaborating on this project: Jeffery Lewis, Bonney Reed-Knight and Cate Crenson.
Full abstract below.

ABSTRACT:
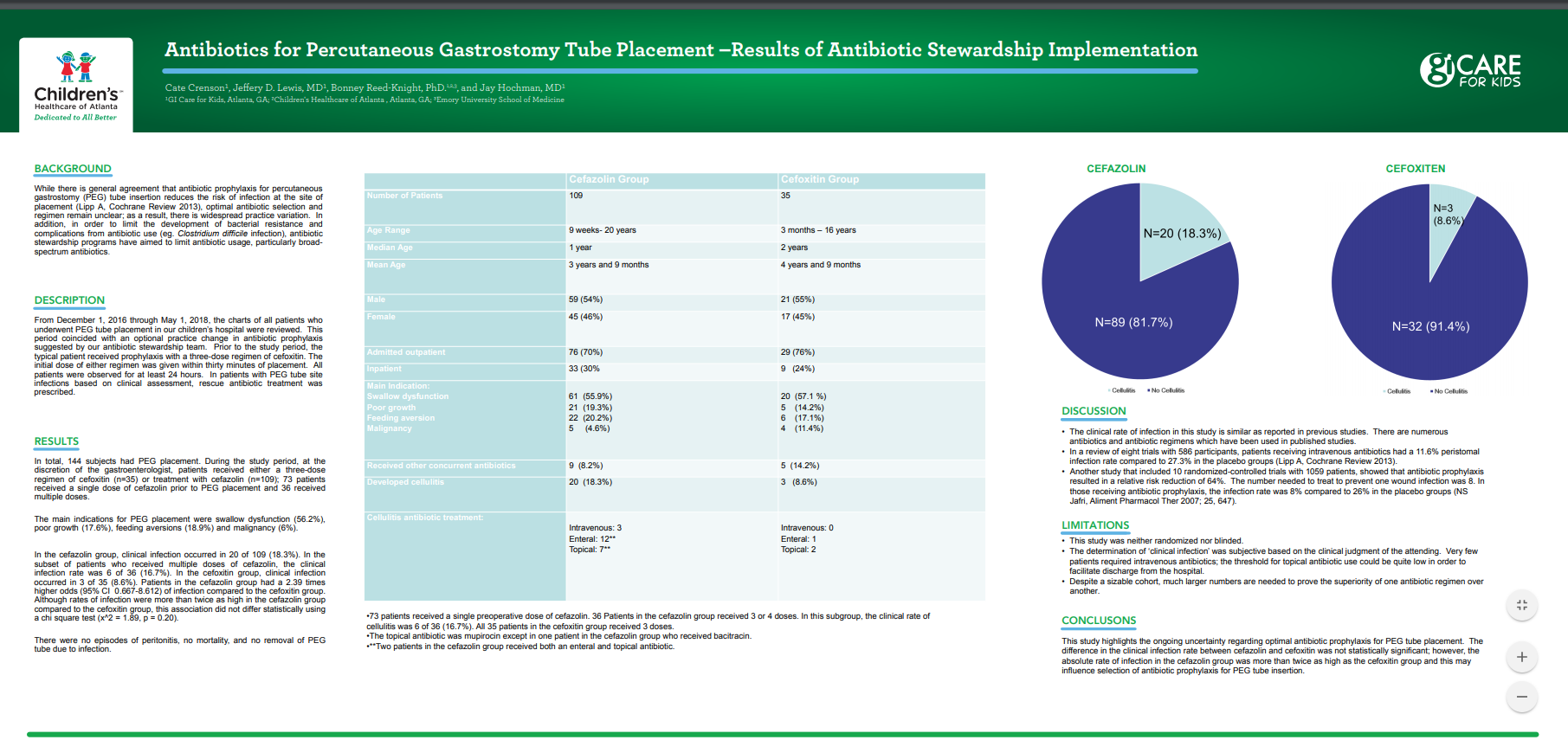
Background: While there is general agreement that antibiotic prophylaxis for percutaneous gastrostomy (PEG) tube insertion reduces the risk of infection at the site of placement (Lipp A, Cochrane Review 2013), optimal antibiotic selection and regimen remain unclear; as a result, there is widespread practice variation. In addition, in order to limit the development of bacterial resistance and complications from antibiotic use (eg. Clostridium difficile infection), antibiotic stewardship programs have aimed to limit antibiotic usage, particularly broad-spectrum antibiotics.
Methods: From December 1, 2016 through May 1, 2018, the charts of all patients who underwent PEG tube placement in our children’s hospital were reviewed. This period coincided with an optional practice change in antibiotic prophylaxis. Prior to the study period, the typical patient received prophylaxis with a three-dose regimen of cefoxitin. During the study period, at the discretion of the gastroenterologist, patients received either a three-dose regimen of cefoxitin (n=38) or treatment with cefazolin (n=109); 73 patients received a single dose of cefazolin prior to PEG placement and 36 received multiple doses. The initial dose of either regimen was given within thirty minutes of placement. All patients were observed for at least 24 hours. In patients with PEG tube site infections based on clinical assessment, rescue antibiotic treatment was prescribed.
Results: In total, 144 subjects had PEG placement. The main indications for PEG placement were swallow dysfunction (56.2%), poor growth (17.6%), feeding aversions (18.9%) and malignancy (6%). In the cefoxitin group, clinical infection occurred in 3 of 35 (8.6%). In the cefazolin group, clinical infection occurred in 20 of 109 (18.3%). In the subset of patients who received multiple doses of cefazolin, the clinical infection rate was 6 of 36 (16.7%). Patients in the cefazolin group had a 2.39 times higher odds (95% CI 0.667-8.612) of infection compared to the cefoxitin group. Although rates of infection were more than twice as high in the cefazolin group compared to the cefoxitin group, this association did not differ statistically using a chi square test (x^2 = 1.89, p = 0.20).
Conclusion: This study highlights the ongoing uncertainty regarding optimal antibiotic prophylaxis for PEG tube placement. The difference in the clinical infection rate between cefazolin and cefoxitin was not statistically significant; however, the absolute rate of infection in the cefazolin group was more than twice as high as the cefoxitin group and this may influence selection of antibiotic prophylaxis for PEG tube insertion.
With Regard to Avoiding Excessive Weight Gain, Breastfeeding is Best
A recent study (AR Goetz et al J Pediatr 2018; 201: 27-33) examines the impact of breastfeeding on the growth of infants with high birth weight (HBW).
Background: “Exclusive breastfeeding is protective against high weight and is recommended by” the AAP for the first 6 months. In this study, the authors hypothesized that “HBW infants would receive a lower percentage of breast milk and consume more formula than NBW infants.”
Key findings:
- HBW infants with high weights at 7-12 months of age demonstrated a rapid decline in the percentage of breast milk feedings compared with HBW infants with normal weights at 7-12 months of age.
- Normal birth weight infants with high weights at 7-12 months of age received a lower percentage of breast milk and more formula intake that those with normal weights at 7-12 months of age.
Because HBW is associated with later risk of obesity/overweight, identifying strategies early in life is important. Furthermore, as a recent study in NEJM has shown (M Geserick et al. NEJM 2018; 379: 1303-12), a lot of weight gain issues happen in the first years of life:
- Almost 90% of children who were obese at 3 years of age were overweight or obese in adolescence
- Among obese adolescents, the most rapid weight gain had occurred between 2 and 6 years of age
My take: This study further shows a strong association between consumption of breast milk and normal weights at 7-12 months of age, both in HBW and NBW.
Related blog posts:

Near Lake Louise, Banff
Direct-Acting Antivirals in Patients Without Advanced Hep C Liver Disease
A recent study (LI Backus et al. Hepatology 2018; 68: 827-38, editorial 804-06) indicates that direct-acting antivirals (DAA) improve mortality in patients with hepatitis C virus (HCV) without advanced liver disease.
Using a registry from the Veterans Affairs, the authors identified 40,664 treated with interferon-free DAA regimens. Overall there was a 96.8% sustained virologic response (SVR). These patients were compare with 62,882 patients who did not receive DAA and without apparent advanced fibrosis.
Background: Long-term benefits have been established in patients with HCV and advanced fibrosis who have had viral eradication with DAA regimens with less hepatic decompensation and less hepatocellular carcinoma.
Key findings:
- SVR in this cohort was associated with a 59% unadjusted reduction in all-cause mortality when compared to those who did not achieve SVR and a 69% reduction compared to the untreated cohort.
- In absolute terms, 1-year mortality rates were reduced by 1.3% with SVR compared to treated group without SVR and by 2.9% compared to no treatments.
These declines in mortality occurred despite the fact that DAA-treated patients had more comorbid conditions and similar access to providers among the three groups. The findings in this population of veterans will need to be replicated in other populations.
My take: This study is a big leap forward by showing that even in groups without advanced fibrosis, treatment with DAA improved a significant clinical endpoint not just a biomarker. There are likely other unmeasured benefits in terms of health and quality of life that are likely to accrue after viral eradication
Related blog posts:
- Word of Caution with New Hepatitis C Medications
- Hepatitis C Reactivation with Chemotherapy
- The Dark Cloud Inside the Silver Lining -What’s Really Going on with Hepatitis C Infection | gutsandgrowth
- Heroin Epidemic Causing Surge in HCV
- HCV now more deadly than HIV | gutsandgrowth
- Updated HCV Guidelines Published | gutsandgrowth

Lake Louise, Banff
Almost Everybody Needs Flu Shot –IBD Patients at Higher Risk
Link: CDC Recommendations for Influenza Vaccination
- Routine annual influenza vaccination is recommended for all persons aged ≥6 months who do not have contraindications.
- Vaccination should be offered by end of October; however, vaccination should continue to be offered as long as influenza viruses are circulating and unexpired vaccine is available.
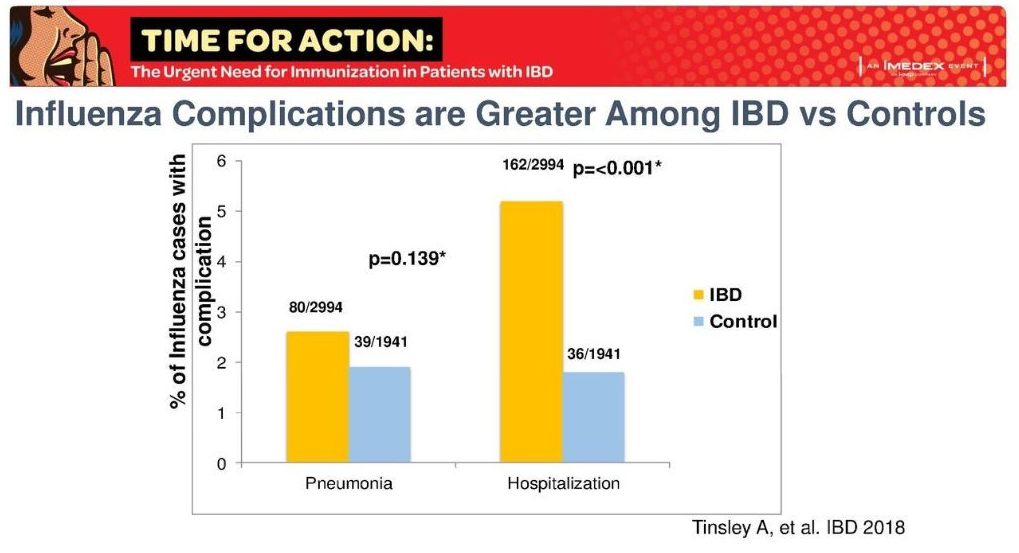

Image Only: Increasing Syphilis in Newborns
Pediatric gastroenterologists/hepatologists need to consider syphilis in infants with elevated liver enzymes and/or cholestasis.

