About gutsandgrowth
I am a pediatric gastroenterologist at GI Care for Kids (previously called CCDHC) in Atlanta, Georgia. The goal of my blog is to share some of my reading in my field more broadly. In addition, I wanted to provide my voice to a wide range of topics that often have inaccurate or incomplete information.
Before starting this blog in 2011, I would tear out articles from journals and/or keep notes in a palm pilot. This blog helps provide an updated source of information that is easy to access and search, along with links to useful multimedia sources.
I was born and raised in Chattanooga. After graduating from the University of Virginia, I attended Baylor College of Medicine. I completed residency and fellowship training at the University of Cincinnati at the Children’s Hospital Medical Center. I received funding from the National Institutes of Health for molecular biology research of the gastrointestinal tract.
During my fellowship, I had the opportunity to work with some of the most amazing pediatric gastroenterologists and mentors. Some of these individuals included Mitchell Cohen, William Balistreri, James Heubi, Jorge Bezerra, Colin Rudolph, John Bucuvalas, and Michael Farrell. I am grateful for their teaching and their friendship. During my training with their help, I received a nationwide award for the best research by a GI fellow.
I have authored numerous publications/presentations including original research, case reports, review articles, and textbook chapters on various pediatric gastrointestinal problems. In addition, I have been recognized by Atlanta Magazine as a "Top Doctor" in my field multiple times.
Currently, I am the vice chair of the section of nutrition for the Georgia Chapter of the American Academy of Pediatrics. In addition, I am an adjunct Associate Clinical Professor of Pediatrics at Emory University School of Medicine. Other society memberships have included the North American Society for Pediatric Gastroenterology Hepatology and Nutrition (NASPGHAN), American Academy of Pediatrics, the Food Allergy Network, the American Gastroenterology Association, the American Association for the Study of Liver Diseases, and the Crohn’s and Colitis Foundation.
As part of a national pediatric GI organization called NASPGHAN (and its affiliated website GIKids), I have helped develop educational materials on a wide-range of gastrointestinal and liver diseases which are used across the country. Also, I have been an invited speaker for national campaigns to improve the evaluation and treatment of gastroesophageal reflux disease, celiac disease, eosinophilic esophagitis, hepatitis C, and inflammatory bowel disease (IBD). Some information on these topics has been posted at my work website, www.gicareforkids.com, which has links to multiple other useful resources.
I am fortunate to work at GI Care For Kids. Our group has 17 terrific physicians with a wide range of subspecialization, including liver diseases, feeding disorders, eosinophilic diseases, inflammatory bowel disease, cystic fibrosis, DiGeorge/22q, celiac disease, and motility disorders. Many of our physicians are recognized nationally for their achievements. Our group of physicians have worked closely together for many years. None of the physicians in our group have ever left to join other groups. I have also worked with the same nurse (Bernadette) since I moved to Atlanta in 1997.
For many families, more practical matters about our office include the following:
– 14 office/satellite locations
– physicians who speak Spanish
– cutting edge research
– on-site nutritionists
– on-site psychology support for abdominal pain and feeding disorders
– participation in ImproveCareNow to better the outcomes for children with inflammatory bowel disease
– office endoscopy suite (lower costs and easier scheduling)
– office infusion center (lower costs and easier for families)
– easy access to nursing advice (each physician has at least one nurse)
I am married and have two sons (both adults). I like to read, walk/hike, bike, swim, and play tennis with my free time.
I do not have any financial relationships with pharmaceutical companies or other financial relationships to disclose. I have helped enroll patients in industry-sponsored research studies.
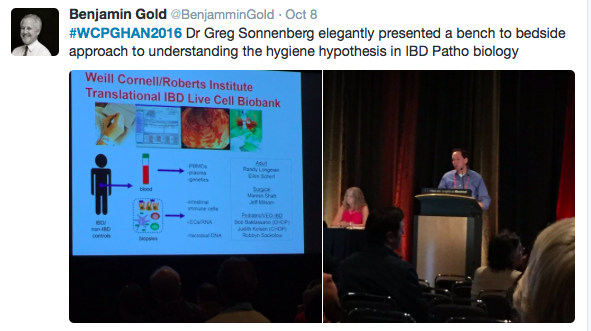
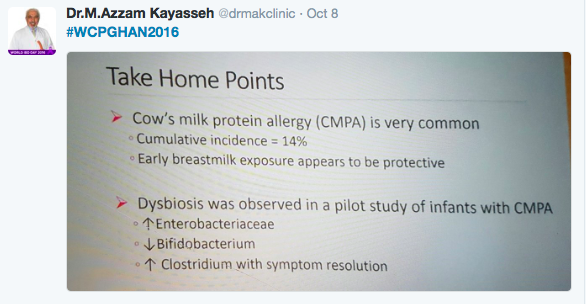
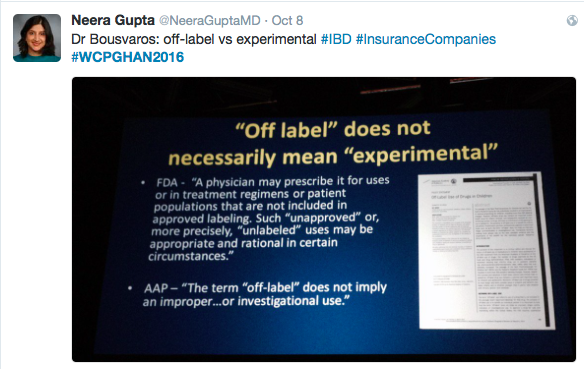
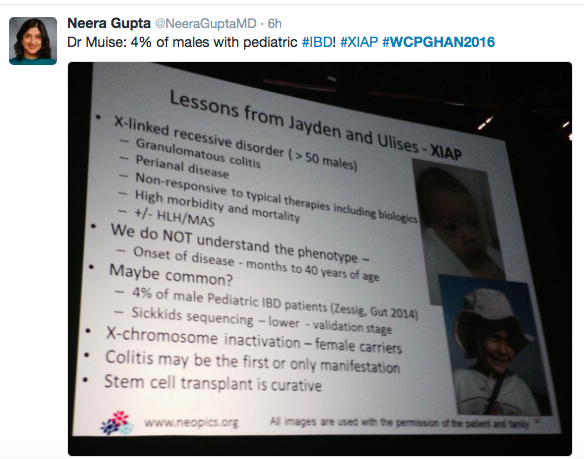
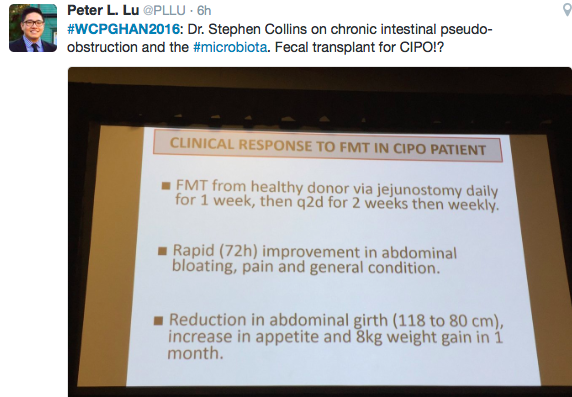
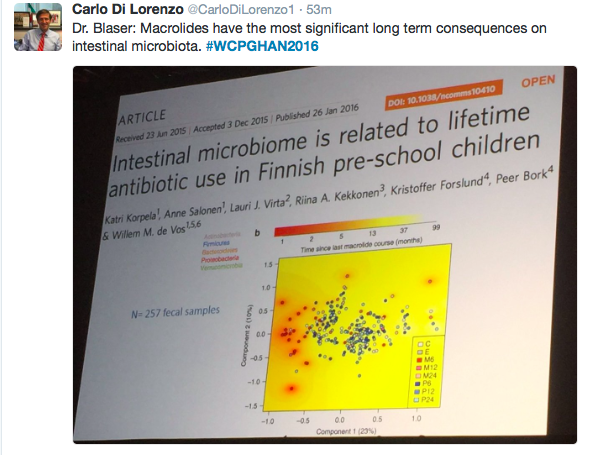
For those who are not attending this year’s national/international GI meeting, I’ve compiled some of the best tweets. These tweets are from 10/6/16.





A recent commentary (G Cholankeril et al. Gastroenterol 2016; 151: 382-86) provides a succinct summary regarding the trends in liver transplantation multiple listing and its implications on notions of utility and justice.
Key points:
- UNOS was established based on Congressional act in 1984: 42 U.S.C. § 274. The principles of “justice” and “utility” were to be key in governing an equitable allocation system.
- Due to allocation inequities, however, some prospective liver transplant candidates seek multiple listings. From 2010 to 2015, 1082 of 70,080 (2%) liver transplant candidates on the waitlist had multiple listings. During that same time frame, 862 (multiply-listed) of 32,431(total transplants) (3%) underwent liver transplantation.
- Candidates who migrated had “shorter waiting time before liver transplantation and higher probability of receiving an organ (multiple listings 80% versus primary listing 46%; P<.001)”
- Multiple listing candidates had lower severity of illness and lower MELD score at time of liver transplantation (multiple listings 25 versus primary listing 28; P<.001)
Regional distribution:
- 46% of the 862 multiply-listed patients who underwent liver transplantation received their organ in UNOS region 3 (Alabama, Arkansas, Florida, Georgia, Louisiana, Mississippi, Puerto Rico)
- 67% of those 862 emigrated away from Regions 2, 5, and 9 -which have the longest waiting times. Figure 1 shows the 11 Regions. Region 2 & 9 include New York, New Jersey, Delaware, West Virginia, Maryland, and Pennsylvania. Region 9 includes California, Nevada, Arizona, New Mexico, and Utah.
My take: Under the current system, liver transplant candidates capable of travelling/multiple listing, are rewarded with earlier liver transplantation & higher likelihood of receiving a liver transplant. Thus, until inequities in organ distribution are better addressed, patient’s may need to consider telling their transplant team: ‘Need Liver, Will Travel’
Related blog posts:

Public Art, New Orleans
Full text: My Vision for Universal, Quality, Affordable Health Care –NEJM
From NEJM: The editors invited the Democratic and Republican presidential nominees, Hillary Clinton and Donald Trump, to answer the following question for Journal readers: What specific changes in policy do you support to improve access to care, improve quality of care, and control health care costs for our nation? Secretary Clinton responded. Mr. Trump did not respond.
The main topics in Hillary Clinton’s commentary include expanding insurance coverage through the affordable care act (i.e. Obamacare), improve affordability in health care with proposals that affect both insurance companies and pharmaceutical companies, improve access to primary care/community care, and to continue to promote innovation/research.

A recent study (MR Nicholson et al. J Pediatr 2016; 176; 50-6) examined the use of multiplex molecular testing to determine the etiology of acute gastroenteritis in children. It is interesting that little has been published about this increasingly common practice of sending a 12 to 15 panel PCR assay when faced with acute GI symptoms, mainly diarrhea.
This study was a prospective population-based study of children <6 years with acute gastroenteritis (2008-2011).
Findings:
- 70.4 % (152/216) samples tested positive for a pathogen, with norovirus the most frequent (n=78, 36.1%). Clostridium difficile was next at 16.2% (n=35).
- 22.7% (n=49) tested positive for more than 1 pathogen including 25 with a C difficile detection
- In this study, the authors noted C difficile colonization in 8% of healthy children aged 0-51 months and in 14% of children <12 months
Implications of this study and this technology:
- Prior to this technology, traditional approaches typically identified less than 15% of the cases of acute gastroenteritis. Thus, this new technology increases the likelihood of a definitive diagnosis.
- Multiple pathogens, particularly with C difficile, illustrate how this new technology will present some difficulties with interpretation. C difficile has very high rates of colonization in infants (anywhere from 25-80%) without AGE symptoms and lower rates of colonization in toddlers. High colonization/detection has been noted in inflammatory bowel disease patients (17%) and pediatric oncology patients (30-55%).
- For C difficile, molecular testing is much less likely to correlate with clinical disease than toxin-based assays. “A recent study in adults found that virtually all CDI-related complications occurred in patients with a positive toxin immunoassay.” (JAMA Intern Med 2015; 175: 1792-801)
My take: These panels are helpful in identifying infectious etiologies of AGE and may help prevent unnecessary endoscopic procedures. Due to their limitations, careful selection of which patients to test and cautious interpretation of the results are needed.
Related blog posts:

Sunset from Bar Harbor, ME
A recent editorial (EW Campion et al. NEJM 2016; 375: 993-4) made a few worthwhile points and shows how NEJM has been successful and innovative over 20 years of using the web and social media.
- This has allowed more widespread access to its content, even by resource-poor countries.
- The use of the web has facilitated quick distribution of multiple resources for outbreaks like Ebola and Zika.
- Currently, every article back to 1812 is available online (over 173,000 with more than 570,000 pages)
- NEJM has 340,000 twitter followers and 1.3 million followers on facebook
- Despite the importance of NEJM, as well as other healthcare media, important caution is needed.
“We do need to be wary of challenges and dangers that the new media have created. On the Internet, speed and simplicity often displace depth and quality, especially on complex subjects. Our privacy is increasingly vulnerable. Misinformation, misrepresentation, and piracy are common. There are health scams and even sham medical conferences and fake medical journals.”
My take: Careful use of internet resources has been incredibly helpful. But, beware of the inherent hazards that have accompanied these advances.
Related blog posts:

Balancing Rock, Bar Harbor
Briefly noted: RM Navari et al. NEJM 2016; 375: 134-42. Olanzapine (marketed as Zyprexa), compared with placebo, in combination with dexamethasone, aprepitant (or fosaprepitant) and a 5-hydroxytryptomaine type 3 antagonist (eg palonosetron, ondansetron, or granisetron) helped reduced nausea/vomiting. Among a total of 380 patients, 74% in the olanzapine group had no nausea/vomiting compared with 45% in the placebo group in the first 24 hours. In the 1st 120 hours, the rates of no nausea/vomiting were 37% vs. 22%. A “complete response,” defined as no emesis episodes and no rescue medications, occurred in 64% vs 41% in the 1st 120 hours. The most concerning side effect reported was severe sedation which was reported in 5%.

Arthur Ravenel Jr Bridge